Convergence of Epidemiology and Modifiable Causal Risk Factors in Inflammatory Bowel Disease and Alzheimer’s Disease
1The First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325035, Zhejiang, China
2Affiliated Cixi Hospital, Wenzhou Medical University, Ningbo 315300, Zhejiang, China
3State Key Laboratory of Brain and Cognitive Sciences, Laboratory of Neuropsychology & Human Neuroscience, The University of Hong Kong, Hong Kong SAR 999077, China
4Human Anatomy Experimental Training Center, School of Basic Medical Sciences, Wannan Medical College, 241002, Wuhu, Anhui, China
5JiaXing University College of Medicine, Jiaxing 314001, Zhejiang, China
6Oujiang Laboratory (Zhejiang Lab for Regenerative Medicine, Vision and Brain Health), National Key Laboratory of Macromolecular Drugs and Large-scale Preparation, School of Pharmaceutical Science, Wenzhou Medical University, Wenzhou 325000, China
7State Key Laboratory of Bioelectronics, School of Biological Science & Medical Engineering, Southeast University, Nanjing 210096, Jiangsu, China
8Integrative Muscle Biology Laboratory, Division of Regenerative and Rehabilitative Sciences, University of Tennessee Health Science Center, Memphis 38163, TN, USA
aThese authors contributed equally to this work.
*Correspondence to: Liuxi Chu, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325035, Zhejiang, China; Affiliated Cixi Hospital, Wenzhou Medical University, Ningbo 315300, Zhejiang, China, E-mail: clx0605@wmu.edu.cn; Zunyong Feng, Oujiang Laboratory (Zhejiang Lab for Regenerative Medicine, Vision and Brain Health), National Key Laboratory of Macromolecular Drugs and Large-scale Preparation, School of Pharmaceutical Science, Wenzhou Medical University, Wenzhou 325000, China, E-mail: fengzy@wmu.edu.cn; Xiaokun Li, Oujiang Laboratory (Zhejiang Lab for Regenerative Medicine, Vision and Brain Health), National Key Laboratory of Macromolecular Drugs and Large-scale Preparation, School of Pharmaceutical Science, Wenzhou Medical University, Wenzhou 325000, China, E-mail: xiaokunli@wmu.edu.cn; Zhouguang Wang, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325035, Zhejiang, China; Oujiang Laboratory (Zhejiang Lab for Regenerative Medicine, Vision and Brain Health), National Key Laboratory of Macromolecular Drugs and Large-scale Preparation, School of Pharmaceutical Science, Wenzhou Medical University, Wenzhou 325000, China, E-mail: wangzhouguang@wmu.edu.cn
Received: February 11 2026; Revised: April 6 2026; Accepted: April 14 2026; Published Online: May 12 2026.
Cite this paper:
Chu L, Dai Z, Wang S et al. Convergence of Epidemiology and Modifiable Causal Risk Factors in Inflammatory Bowel Disease and Alzheimer’s Disease. BIO Integration 2026; 7: 1–17.
DOI: 10.15212/bioi-2026-0023. Available at: https://bio-integration.org/
Download citation
© 2026 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Background: Inflammatory bowel disease (IBD) and Alzheimer’s disease (AD) are major global health burdens that are rising in prevalence but are typically studied as distinct disorders. This study systematically characterizes the convergent risk architecture between IBD and AD using integrated epidemiological, causal, and molecular approaches.
Methods: Global epidemiology, Mendelian randomization (MR), and in silico transcriptomic cross-validation were integrated. Global Burden of Disease 2021 data from 204 countries (1990–2021) were analyzed. Two-sample MR was conducted using inverse-variance weighted (IVW) as the primary method, with weighted median, MR-Egger, and MR-PRESSO as sensitivity analyses to assess causal effects of genetically proxied lifestyle and socio-environmental factors on IBD and AD. Cross-disease transcriptomic analyses were performed to identify shared pathways.
Results: Parallel increases in IBD and AD burden were observed, with pronounced sociodemographic disparities and a steep rise in AD in aging, high-sociodemographic index (SDI) populations. Higher genetically proxied educational attainment was associated with reduced risk of IBD (odds ratio [OR] = 0.87, 95% confidence interval [CI] = 0.80–0.94) and AD (OR = 0.82, 95% CI = 0.74–0.91). Higher coffee consumption increased IBD (OR = 1.20, 95% CI = 1.09–1.33) and AD risk (OR = 1.19, 95% CI = 1.05–1.35). Higher beef intake had an inverse association with IBD (OR = 0.48, 95% CI = 0.27–0.88) and AD (OR = 0.0012, 95% CI = 0.0006–0.0025). Transcriptomic analyses demonstrated concordant dysregulation of inflammatory and immune pathways, including TNF/NF-κB signaling. Projections indicated a continued escalation of AD burden to 2050.
Conclusions: Convergent epidemiologic, causal, and molecular evidence indicates that IBD and AD share modifiable determinants along the gut–brain axis. These findings highlight opportunities for coordinated prevention strategies targeting chronic inflammatory disease trajectories.
Keywords
Alzheimer’s disease, genome-wide association studies, GBD, IBD, Mendelian randomization.
Introduction
The Global Burden of Disease (GBD) 2021 Study provides a comprehensive assessment of global health trends, covering data from 1990–2021 across 204 countries and territories. Within this extensive framework, inflammatory bowel disease (IBD) and Alzheimer’s disease (AD) have emerged as conditions of particular concern due to the increasing prevalence, profound morbidity, and escalating societal and economic burden [1–4]. IBD, including Crohn’s disease and ulcerative colitis, is a chronic inflammatory disorder of the gastrointestinal tract [3, 5], whereas AD is a progressive neurodegenerative disease characterized by cognitive decline [6, 7]. Despite distinct clinical manifestations, both conditions disproportionately affect aging populations and pose significant challenges to healthcare systems.
Mounting epidemiologic and biological evidence indicates an intriguing association between IBD and AD that is largely mediated by systemic inflammation and gut-brain interactions. For example, population-based studies have reported a higher incidence of AD in patients with IBD that is independent of traditional risk factors [8]. Chronic systemic inflammation and dysbiosis of the gut microbiota, which are hallmarks of IBD, have been mechanistically linked to cognitive impairment and neurodegeneration [9]. Meta-analyses further substantiate these findings, demonstrating increased risks of AD and IBD among individuals with Crohn’s disease and ulcerative colitis, thereby implicating gut microbiota as a pivotal modulator of gastrointestinal and neurologic pathology [9].
Mendelian randomization (MR), an emerging method that is applied in genetic epidemiology, provides a unique opportunity to test causality by using genetic variants as instrumental variables for modifiable exposures [10]. MR minimizes confounding factors and reverse causation that often challenge traditional observational studies by exploiting the random allocation of alleles at conception. This approach provides a more robust inference of causality, especially when investigating complex diseases influenced by multiple genetic and environmental factors [11]. Consequently, MR serves as a powerful tool to clarify the directionality and causality of the links between these interconnected conditions, guiding more targeted prevention and intervention efforts.
Moreover, recent MR analyses support a bidirectional association between IBD and AD, implying that systemic inflammation and gut-derived metabolites might influence neurodegeneration, while neuroinflammation could also impact gastrointestinal health [12]. This evidence underscores the importance of exploring the interconnected mechanisms underpinning these diseases, which could open avenues for early intervention and integrated treatment strategies. Given these compelling findings, studying IBD and AD together can enhance our understanding of the shared pathogenic pathways and risk factors. The use of advanced genetic epidemiology tools, such as MR, allows us to infer causal relationships between modifiable exposures and disease outcomes more reliably, reducing bias inherent in observational studies [13].
In this study global-scale epidemiologic data from the GBD 2021 were integrated with large-scale MR analyses to systematically characterize the burden, temporal trends, and regional variation of IBD and AD, while interrogating the causal effects of lifestyle, dietary, and socioeconomic factors. We aimed to delineate shared determinants and uncover mechanistic insights into gut–brain interactions by combining population-level projections with genetically informed causal inference. Ultimately, the findings can be utilized to inform public health policy and highlight novel opportunities for prevention and intervention in these two increasingly prevalent and interconnected diseases.
Methods
Data source
This study was based on data from the GBD 2021 Study. The GBD 2021 database is comprised of cross-sectional global data collected between 1990 and 2021 from 204 countries and territories. The GBD 2021 database evaluates the burden of 371 diseases and injuries, including IBD and AD. Data are categorized by gender (male, female, and total population), age groups (≥ 40 years of age), geographic region (204 countries and territories), and sociodemographic index (SDI) for these conditions. The ICD-10 codes used for IBD were K50 for Crohn’s disease and K51 for ulcerative colitis. Data sources included census records, household surveys, vital registration systems, hospital records, and disease registries, all of which were compiled and stored within the Global Health Data Exchange (GHDx).
Estimated risk factors
The temporal trends of age-standardized disease rates were quantified using the estimated annual percentage change (EAPC), which summarizes the average yearly change over the study period. A log-linear regression model fitted the following form for each outcome:

where ASR_t denotes the age-standardized rate (e.g., incidence, prevalence, mortality, or disability-adjusted life years [DALYs]) in calendar year t, α is the intercept, β is the slope, and ε_t is the error term. The EAPC and the 95% confidence interval (CI) were then calculated as follows:

with the 95% CI derived from the β standard error. This approach facilitated the quantification of the direction and magnitude of temporal trends in disease burden.
Sociodemographic index
The sociodemographic index (SDI) is a composite measure that captures the social and economic factors influencing health outcomes across different regions [14]. The SDI is calculated as the geometric mean of three components: the total fertility rate among individuals < 25 years of age (TFU25); the average education level of individuals ≥ 15 years of age (EDU15+); and the lag-distributed income per capita (LDI). The SDI values were multiplied by 100 in the GBD 2021 study to produce a scale that ranges from 0–100. Log-transformed age-standardized DALY rates were modeled as a function of calendar year, SDI category, and the interaction using linear regression to formally assess whether temporal trends differed across SDI categories. EAPCs and 95% CIs were derived from the estimated slopes and heterogeneity in EAPCs across SDI categories was evaluated using a global Wald (F) test for the interaction term.
Auto regressive integrated moving average (ARIMA) analysis
In this study the ARIMA model was used to project future DALYs related to AD and IBD from 2022–2050. ARIMA is a widely used time series analysis method that models data based on past values and errors, providing reliable short- and long-term forecasts. These projections offer valuable insights for public health planning and the development of preventive strategies.
Mendelian randomization analysis
A two-sample MR approach was used to evaluate the causal associations between a broad spectrum of risk factors and neurodegenerative diseases (IBD and AD). Summary statistics for the genome-wide association study (GWAS) were sourced from large-scale European ancestry studies, as detailed in Supplementary Table S1. These datasets encompassed traits related to education, intelligence, smoking behaviors (e.g., age of initiation, lifetime smoking, peer smoking, cessation, and initiation), alcohol consumption (frequency, use disorder, and drinks per week), coffee intake, sleep characteristics (chronotype, insomnia, and sleep duration), physical activity (moderate-to-vigorous activity, strenuous exercises, and sedentary behavior), dietary factors (e.g., cereal, vegetable, fish intake, processed meat, cheese, and fruit intake), obesity-related traits (BMI, birth weight, childhood BMI, waist and hip circumference, waist-to-hip ratio, body fat percentage, and visceral adiposity), serum biomarkers (ferritin, transferrin, iron, zinc, magnesium, and glucose), and other exposures.
Instrumental variables were selected as genome-wide significant single nucleotide polymorphisms (SNPs) for each exposure (P < 5 × 10−8) and clumped for linkage disequilibrium (r2 < 0.01 within a 10,000 kb window). The number of SNPs used for each trait is presented in the corresponding result tables. The primary causal estimates were obtained using the inverse-variance weighted (IVW) method under fixed- and random-effects models. Between-variant heterogeneity was assessed using Cochran’s Q statistic. Median-based estimators (weighted median and simple median) were applied to provide more robust causal estimates in the presence of substantial heterogeneity.
Horizontal pleiotropy was evaluated using several complementary approaches. Directional (unbalanced) pleiotropy was tested with the MR-Egger intercept. A non-significant intercept was interpreted as no strong evidence of directional pleiotropy. MR-PRESSO was applied to detect and correct for outlier SNPs that may introduce horizontal pleiotropy, as appropriate, reporting both the global test and outlier-corrected estimates. Leave-one-out analyses was performed by iteratively excluding each SNP and re-estimating the causal effect to assess the influence of individual variants. The causal direction of associations was examined using the MR Steiger test, which compares the variance explained in the exposure and the outcome.
Multiple testing was addressed using the Bonferroni correction with adjusted significance thresholds based on the number of exposures tested. All analyses were performed in R using the TwoSampleMR package together with MR-PRESSO and related functions for heterogeneity and pleiotropy assessment. Effect sizes are reported per standard deviation increase in genetically predicted exposure or per log-odds unit, when applicable. This combination of primary and sensitivity analyses was used to ensure the robustness and reliability of the inferred causal effects of the evaluated risk factors on IBD and AD.
Public transcriptomic cross-validation
An ancillary in silico transcriptomic cross-validation was performed using publicly available bulk RNA-sequencing datasets to explore potential biological mechanisms underlying the observed epidemiologic association between IBD and AD. Colonic mucosa biopsies from patients with Crohn’s disease or ulcerative colitis and non-IBD controls obtained from the Gene Expression Omnibus [GEO] (GSE16879 and GSE57945) were analyzed. Bulk RNA-sequencing data from post-mortem temporal cortex samples of pathologically confirmed AD cases and age-matched cognitively normal controls from the AMP-AD Knowledge Portal and GEO (GSE7621 and GSE49036) were used.
Raw count matrices were pre-processed by removing genes with low expression, then normalized for library size and compositional bias using the trimmed mean of M values (TMM) method. Differential expression analysis was performed separately for each IBD versus control and AD versus control datasets using the limma-voom pipeline, with voom transformation applied to model the mean–variance relationship. All models were adjusted for available covariates, including age, gender, and technical or batch effects, for which such information was provided.
Genes were considered differentially expressed if both of the following criteria were met: false discovery rate (FDR) < 0.05 (Benjamini–Hochberg adjustment) and an absolute log2 fold-change (|log2FC|) ≥ 1. Differentially expressed gene (DEG) lists were generated at the gene level for each disease and stratified by direction of change (up- and down-regulated). Shared DEGs between IBD and AD were identified by taking the intersection of the respective DEG sets at the gene symbol level. Whether shared DEGs exhibited concordant (both up-regulated or both down-regulated) or discordant directions of change across the two diseases were recorded for interpretability.
Pathway enrichment analyses were performed separately for IBD-specific DEGs, AD-specific DEGs, and the shared DEG set using the clusterProfiler R package. Gene Ontology (GO) biological process terms and KEGG pathways were interrogated using the expressed genes in each dataset as the background (gene universe). Enrichment results with a FDR < 0.05 were considered statistically significant. Enrichment of curated immune-related gene sets derived from established immune and inflammation-focused annotations were evaluated to further characterize the shared inflammatory signature. This transcriptomic cross-validation provided complementary biological context for the epidemiologic association between IBD and AD.
Ethical statement
This study was based exclusively on secondary analyses of publicly available, de-identified data, including GBD estimates, GWAS summary statistics, and bulk transcriptomic datasets obtained from the GEO and the AMP-AD Knowledge Portal. All original studies received ethical approval from the respective institutional review boards, as stated in the corresponding publications. No new data were collected and no individual-level identifiable information was accessed. Therefore, additional ethical approval and informed consent were not required for the present analyses.
Results
Global burden analysis from 1990–2021
The global burden of IBD has increased substantially between 1990 and 2021, as illustrated in Table 1. The total DALYs were approximately 610,132 (95% uncertainty interval [UI]: 507,914–738,219) in 1990, increasing to 1,231,977 (95% UI: 1,013,999–1,466,718) in 2021. The number of DALYs cases increased from 610,132 (95% UI: 507,914–738,219) in 1990 to 1,231,977 (95% UI: 1,013,999–1,466,718) in 2021, while the age-standardized DALYs rate decreased slightly from 46.42 to 40.71 per 100,000 population (EAPC: −0.37%). Similarly, the total number of deaths increased from approximately 18,151 (95% UI: 14,566–22,067) in 1990 to 42,735 (95% UI: 35,153–50,247) in 2021 with the age-standardized death rate decreasing from 1.61 to 1.44 per 100,000 (EAPC: −0.26%). The incidence of age-standardized deaths increased from 109,189 (95% UI: 83,938–138,993) to 255,428 (95% UI: 194,351–326,259) and the prevalence increased from 1,433,658 (95% UI: 1,174,138–1,741,835) to 2,977,293 (95% UI: 2,399,155–3,648,902). The age-standardized incidence rate increased modestly from 7.78 to 8.41 per 100,000, while the prevalence rate decreased slightly from 102.93 to 97.71 per 100,000. The number of years lived with disability (YLDs) increased from 214,439 to 440,185 and the number of years of life lost (YLLs) increased from 395,694 to 791,793 with respective slight decreased in the age-standardized rate.
Table 1 Overall Burden of Global Disease Metrics
| Metric | Number of DALYs Cases (95% UI) in 1990 | Age-standardized DALYs Rate Per 100,000 (95% UI) in 1990 | Number of DALYs Cases (95% UI) in 2021 | Age-standardized DALYs Rate Per 100,000 (95% UI) in 2021 | EAPC [% Per Year] (95% CI) |
|---|---|---|---|---|---|
| IBD | |||||
| DALYs | 610132.36 (507913.89–738219.03) | 46.42 (38.66–56.06) | 1231977.48 (1013997.32–1466717.94) | 40.71 (33.46–48.49) | −0.37 (−0.45–0.29) |
| Deaths | 18150.55 (14566.45–22066.81) | 1.61 (1.29–1.94) | 42734.66 (35153.33–50246.86) | 1.44 (1.18–1.7) | −0.26 (−0.42–0.11) |
| Incidence | 109188.74 (83937.6–138993.27) | 7.78 (5.98–9.9) | 255427.91 (194351.01–326259.33) | 8.41 (6.4–10.75) | 0.28 (0.24–0.33) |
| Prevalence | 1433658.76 (1174138.74–1741835.48) | 102.93 (84.14–125.23) | 2977292.88 (2399155.53–3648902.99) | 97.71 (78.73–119.73) | −0.1 (−0.2–0.01) |
| YLDs | 214438.78 (140935.93–303780.97) | 15.34 (10.08–21.73) | 440184.95 (285535.99–621546.94) | 14.46 (9.37–20.42) | −0.12 (−0.22–0.02) |
| YLL | 395693.58 (313946.8–488835.01) | 31.08 (24.72–38.19) | 791792.53 (654127.82–945748.83) | 26.25 (21.64–31.38) | −0.5 (−0.58–0.42) |
| AD | |||||
| DALYs | 13484443.02 (5933327.64–29466174.51) | 1298.21 (563.25–2828.16) | 39650953.2 (17519808.02–84041018.74) | 1344.5 (592.66–2845.85) | 0.08 (0.05–0.1) |
| Deaths | 666141.56 (158115.4–1765947.99) | 72.92 (17.43–191.14) | 2197548.23 (541615.57–5501603.42) | 76.39 (18.86–190.7) | 0.12 (0.1–0.14) |
| Incidence | 3737151.14 (2645259.14–5121096.08) | 337.83 (241.06–460.44) | 10486625.88 (7386116.99–14376465.36) | 351.07 (247.62–480.98) | 0.06 (0.03–0.08) |
| Prevalence | 21118019.98 (16555241.18–26514550.02) | 1927.82 (1515.25–2412.05) | 60277075.06 (47015177.29–75719554.27) | 2021.43 (1576.88–2539.09) | 0.07 (0.05–0.1) |
| YLDs | 4226574.12 (2849938.11–5871672.7) | 392.11 (264.98–540.92) | 12203988.6 (8218710.26–16923785.62) | 410.34 (276.36–568.52) | 0.06 (0.04–0.09) |
| YLLs | 9257868.9 (2156019.55–25031478.83) | 906.1 (213.27–2418.1) | 27446964.59 (6629615.56–70321786.65) | 934.15 (226.27–2383.9) | 0.08 (0.06–0.1) |
UI: uncertainty interval; EAPC: estimated annual percentage change; DALYs: disability-adjusted life years; YLDs: years lived with disability; YLLs: years of life lost; IBD: inflammatory bowel disease; AD: Alzheimer’s disease.
The global burden associated with AD also increased markedly between 1990 and 2021. The total DALYs increased from approximately 13.48 million (95% UI: 5.93–29.47 million) in 1990 to approximately 39.65 million (95% UI: 17.52–84.04 million) in 2021. The number of DALYs cases increased from 13,484,443 (95% UI: 5,933,327–29,466,174) to 39,650,953 (95% UI: 17,519,808–84,041,018). The age-standardized DALYs rate increased slightly from 1,298.21 to 1,344.5 per 100,000 (EAPC: 0.08%). The total deaths increased from 666,142 (95% UI: 158,115–1,765,948) to 2,197,548 (95% UI: 541,616–5,501,603) with the age-standardized death rate increasing from 72.92 to 76.39 per 100,000 (EAPC: 0.12%). The incidence of deaths increased from about 3,737,151 (95% UI: 2,645,259–5,121,096) to 10,486,626 (95% UI: 7,386,116–14,376,465) and the prevalence increased from 21,118,019 (95% UI: 16,555,241–26,514,550) to 60,277,075 (95% UI: 47,015,177–75,719,554). The age-standardized incidence and prevalence death rates showed slight upward trends with YLDs increasing from 4,226,574 to 12,203,988 and YLLs from approximately 9,257,869 to 27,446,965.
Regionally, Australasia experienced the most significant increase in DALYs due to IBD, increasing from approximately 5,616.57 (95% UI: 3,962.54–7,680.81) in 1990 to 16,753.08 (95% UI: 12,525.05–21,792.74) in 2021 with an EAPC of 0.89%. East Asia showed the most notable decline in the age-standardized DALYs rate, decreasing from 28.23 to 13.67 per 100,000 population (EAPC: −2.49%). Western Europe had the largest increase in deaths, from 532.63 (95% UI: 461.31–640.7) in 1990 to 925.24 (95% UI: 808.49–1,045.78) in 2021 with an EAPC of 0.39%. East Asia experienced the most significant decline in the age-standardized death rate, decreasing from 1.60 to 0.67 per 100,000 (EAPC: −3.2%). Central Asia had the largest increase in the incidence of deaths, from 1,290.9 (95% UI: 951.27–1,745.52) to 3,146.31 (95% UI: 2,319.34–4,256.38) with an EAPC of 0.38%. Finally, East Asia had the most substantial increase in the prevalence of deaths, increasing from 32,983.27 (95% UI: 25,355.14–42,792.08) in 1990 to 131,524.09 (95% UI: 102,113.29–171,728.08) in 2021 with an EAPC of 2.29% (Figure 1A, B).
Figure 1 Descriptive statistics of IBD- and AD-related indicators across GBD 2021 data for 21 regions. (A) and (B) depict the distribution of IBD-related burden across the 21 GBD regions with (A) showing the age-standardized rates (DALYs, deaths, and incidence) and (B) illustrating the absolute number of cases. (C) and (D) illustrate the similar distribution for Alzheimer’s disease (AD) with (C) displaying age-standardized rates and (D) showing the number of cases for DALYs, deaths, and incidence across the same regions.
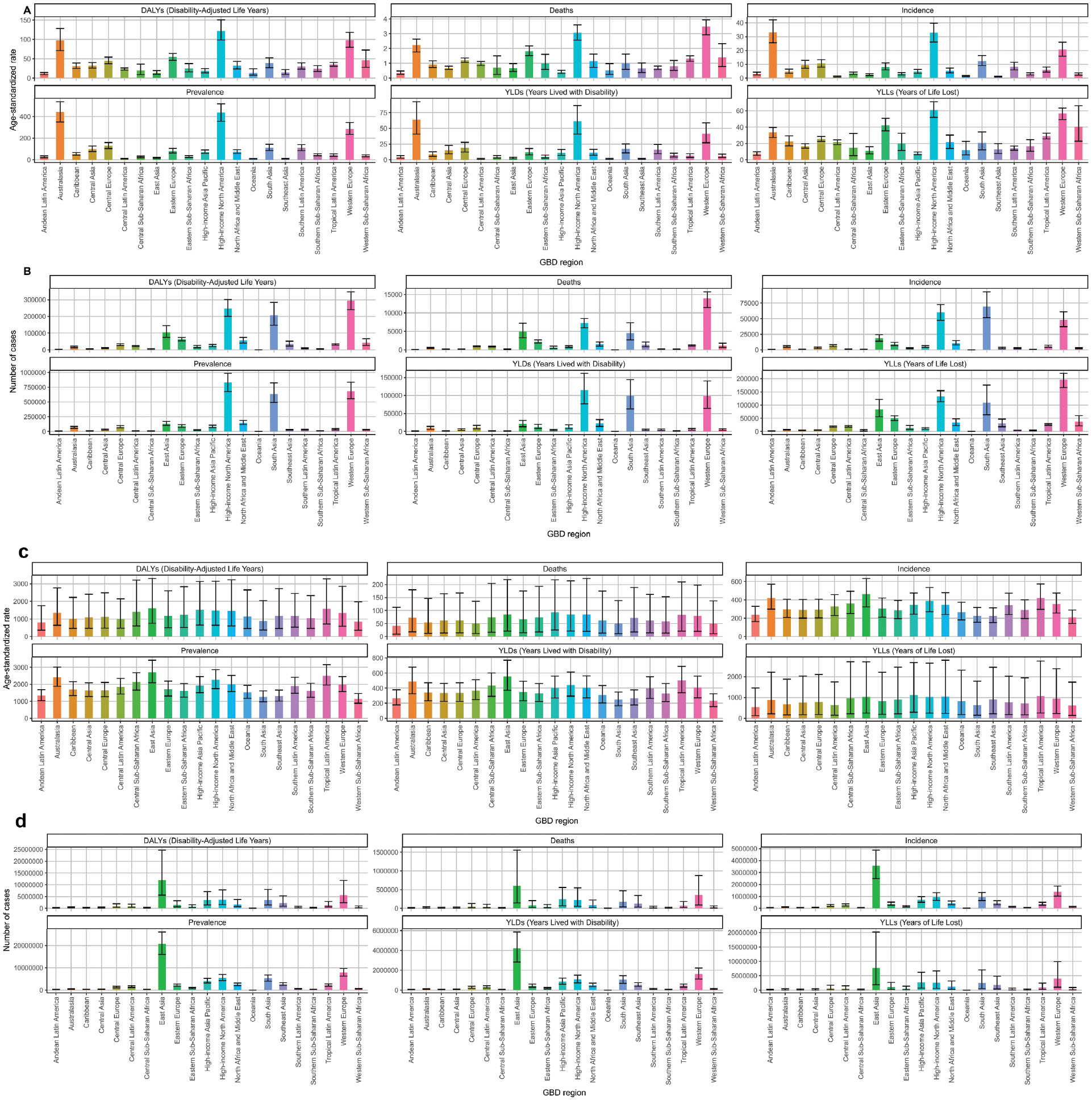
Regionally, East Asia had the most significant number of DALYs cases for IBD with approximately 2,885,697 (95% UI: 1,250,618–6,802,704) and the highest age-standardized DALYs rate at 1,507.26 per 100,000 (95% UI: 644.2–3,529.96) in 1990. East Asia continued to have the largest number of DALYs cases by 2021, increasing to 11,950,683 (95% UI: 5,626,996–24,652,262) with a rate of 1,599.07 per 100,000 (95% UI: 748.24–3,296.66). East Asia also had the most substantial burden of DALYs deaths in 1990 with 125,517,668 (95% UI: 29,318,250–364,830,350) cases and the highest age-standardized death rate (82.72 per 100,000). East Asia remained the region with the highest death count in 2021, reaching 602,800 (95% UI: 147,256–1,551,834) and a rate of 85.07 per 100,000. East Asia had the highest incidence of deaths in 1990 with 776,332 (95% UI: 533,974–1,083,370) cases, increasing to 3,547,183 (95% UI: 2,481,054–4,863,099) in 2021. The prevalence of deaths in East Asia increased from 4,466,977 (95% UI: 3,420,477–5,679,887) cases in 1990 to 20,700,390 (95% UI: 16,043,617–26,091,250) in 2021, making East Asia the region with the most substantial disease burden across multiple metrics (Figure 1C, D).
Differences in IBD and AD burden across age and gender
The 50–54-year age group had the highest number of DALYs cases for IBD (73,398; 95% UI: 60,143–90,604) and the highest age-standardized DALYs rate (34.46 per 100,000; 95% UI: 28.23–42.53) in 1990. The same age group continued to bear the highest number of cases by 2021, increasing to 125,251 (95% UI: 98,989–154,291) with a rate of 27.57 per 100,000 (95% UI: 21.79–33.96). The overall trend had a slight decline in the age-standardized DALYs rate across all age groups with the most notable decrease in the 60–64-year age group, which declined from 46.37 to 40.97 per 100,000 (EAPC: −0.29). The highest death counts in 1990 were in the 65–69-year age group (1747; 95% UI: 1,419–2,104), increasing in 2021 to 3427 (95% UI: 2,990–4,009) with an overall decline in the age-standardized death rate from 1.41 to 1.19 per 100,000 (EAPC: −0.59). The incidence was highest in the 50–54-year age group, increasing from 16,250 (95% UI: 12,099–21,098) cases in 1990 to 37,624 (95% UI: 27,733–48,990) in 2021 with a slight increase in the age-standardized incidence rate. The prevalence followed a similar pattern, peaking in the 50–54-year age group, increasing from 214,300 (95% UI: 176,481–257,917) cases in 1990 to 433,499 (95% UI: 346,603–530,226) in 2021 (Figure 2A, B).
Figure 2 Age-related distribution of IBD- and AD-related burden across GBD 2021 data for 21 regions. (A) and (B) display the distribution of IBD-related indicators across different age groups with (A) showing age-standardized rates (DALYs, deaths, and incidence) and (B) illustrating the number of cases. (C) and (D) present the same indicators for AD with (C) showing age-standardized rates and (D) depicting the number of cases across different age groups.
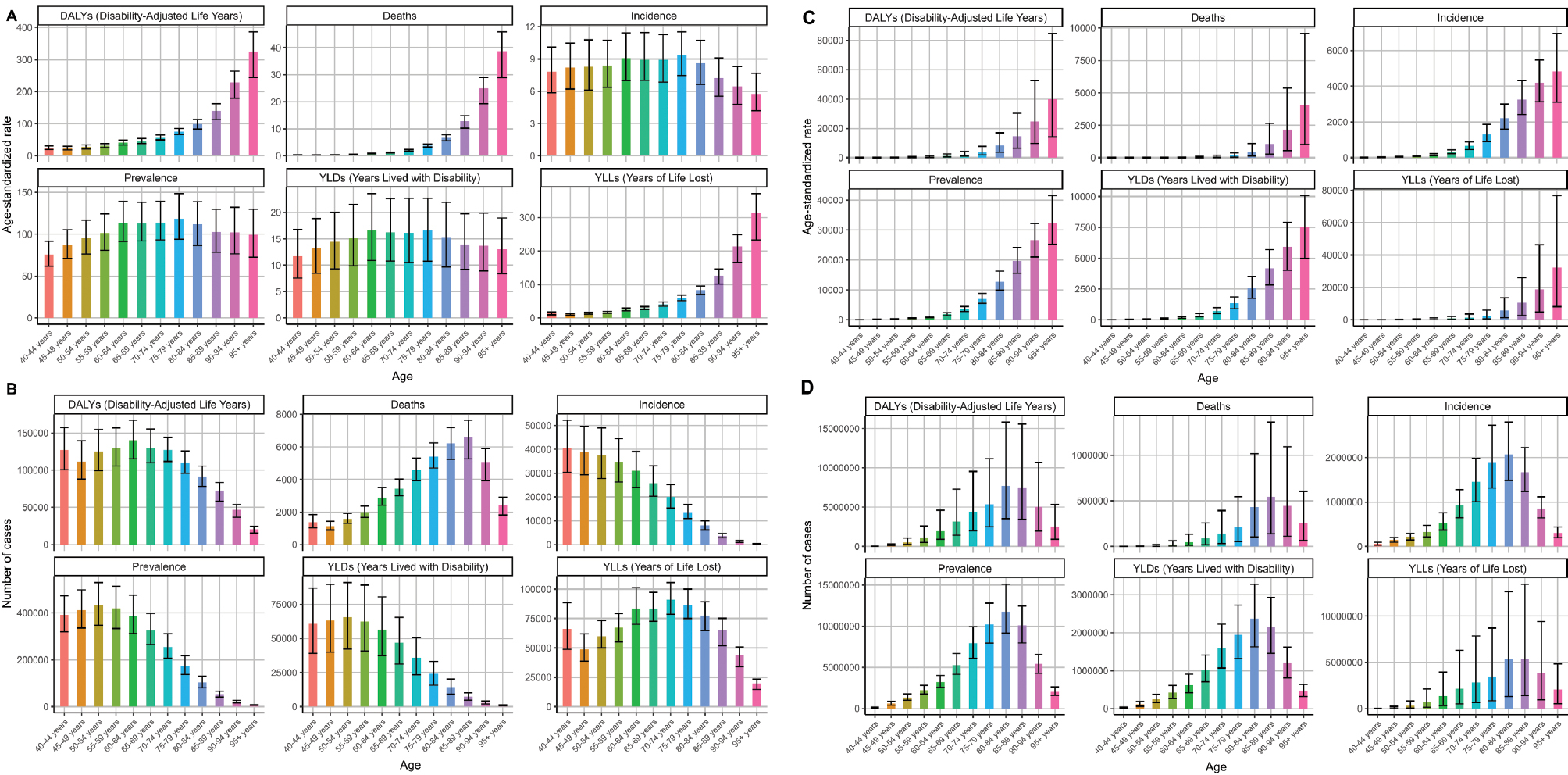
The 70–74-year age group had the highest number of DALYs cases for AD (1,631,927; 95% UI: 729,673–3,659,124) and the highest age-standardized DALYs rate at 1,931.01 per 100,000 (95% UI: 861.81–4,321.78) in 1990. This same age group had a substantial increase to 4,445,351 (95% UI: 2,003,614–9,542,641) cases in 2021 with a rate of 1,993.42 per 100,000 (95% UI: 898.48–4,279.19). Although the absolute number of cases and deaths in older populations has grown significantly, the age-standardized DALYs rate has shown a slight decline over time, notably in the 60–64-year age group (from 568.78 to 575.53 per 100,000; EAPC: 0.07). The death counts increased from 156,304 in 1990 to approximately 543,471 in 2021 with death rates rising from 1,009.95 to 1,057.08 per 100,000. The incidence and prevalence also peaked in the 70–74-year age group, increasing from 35,271 cases in 1990 to nearly 1,459,266 cases in 2021, and from 2.76 million to > 7.94 million, respectively. Overall, older age groups, particularly the > 70-year age group, continue to bear the highest burden of AD with substantial increases in the absolute number over time, while age-standardized rates remained relatively stable or slightly declined (Figure 2C, D).
Table 2 presents the overall burden of disease metrics stratified by gender for major conditions (IBD and AD) for1990 and 2021 with emphasis on trends in disease prevalence, mortality, and DALYs. Females and males exhibited comparable DALY counts for IBD in 1990 with approximately 306,241 and 303,892 cases, respectively, and age-standardized rates of 44 and 49 per 100,000, both of which slightly decreased over time (EAPC: females −0.33; males −0.39). The mortality rates were marginally higher in males with death counts of 8255 (females) and 8255 (males) in 1990 and increasing modestly by 2021, while the age-standardized death rates decreased slightly. The incidence and prevalence of IBD increased substantially, especially in older populations, with the prevalence increasing from 749,000 (females) and 685,000 (males) in 1990 to 1.54 and 1.43 million in 2021, respectively. The YLDs and YLLs mirrored these trends, indicating a rising disease burden but with modest declines in age-standardized rates. Conversely, AD displayed a markedly higher burden with females experiencing approximately 9.19 million DALYs in 1990, rising to > 26 million in 2021, and males with 4.29 million increasing to 13.6 million. Notably, the age-standardized DALYs rate increased slightly for females (EAPC: 0.08) and more substantially for males (0.21). The mortality data revealed a consistent decline in age-standardized death rates for both genders but the total deaths increased due to population growth and aging. The prevalence and incidence of AD also increased significantly with the prevalence increasing from 13.7 million (females) and 7.4 million (males) in 1990 to > 38 and 22 million, respectively, in 2021. Overall, these data highlight substantial increases in disease burden over the 3 decades that were driven by demographic shifts, although age-standardized rates suggested some improvement or stabilization in some metrics. These findings underscore the importance of targeted public health strategies to mitigate the growing impact of IBD and AD across genders.
Table 2 Overall Burden of Global Disease Metrics for Females and Males
| Gender | Metric | Number of DALYs Cases (95% UI) in 1990 | Age-standardized DALYs Rate Per 100,000 (95% UI) in 1990 | Number of DALYs Cases (95% UI) in 2021 | Age-standardized DALYs Rate Per 100,000 (95% UI) in 2021 | EAPC [% Per Year] (95% CI) |
|---|---|---|---|---|---|---|
| IBD | ||||||
| Female | DALYs | 306240.54 (240001.71–388919.42) | 43.82 (34.34–55.58) | 626101.17 (500635.43–763837.92) | 38.83 (30.99–47.46) | −0.33 (−0.43–0.23) |
| Male | DALYs | 303891.82 (237475.8–380176.29) | 48.78 (38.26–60.67) | 605876.31 (492088.5–742228.06) | 42.57 (34.62–52.04) | −0.39 (−0.45–0.33) |
| Female | Deaths | 9895.51 (7459.79–13014.37) | 1.54 (1.16–2.01) | 23427.27 (18265.27–29217.39) | 1.38 (1.08–1.73) | −0.26 (−0.45–0.08) |
| Male | Deaths | 8255.04 (6156.27–10921.64) | 1.64 (1.25–2.13) | 19307.39 (15786.98–24303.62) | 1.49 (1.22−1.86) | −0.22 (−0.33–0.1) |
| Female | Incidence | 54736.04 (42053.62–69969.95) | 7.58 (5.83–9.7) | 128615.49 (98044.48–164058.19) | 8.26 (6.3–10.54) | 0.31 (0.26–0.36) |
| Male | Incidence | 54452.7 (41836.17–69056.64) | 7.99 (6.15–10.13) | 126812.42 (96315.02–161739.45) | 8.58 (6.52–10.94) | 0.25 (0.21–0.29) |
| Female | Prevalence | 748891.62 (611215.76–908282.1) | 104.07 (84.88–126.26) | 1540665.83 (1243367.26–1887141.58) | 98.26 (79.36–120.29) | −0.11 (−0.22–0) |
| Male | Prevalence | 684767.14 (561434.83–832092.76) | 101.94 (83.29–124.18) | 1436627.05 (1154500.93–1766039.15) | 97.27 (78.11–119.64) | −0.09 (−0.19–0.01) |
| Female | YLDs | 113611.4 (74995.42–161664.03) | 15.77 (10.41–22.43) | 230535.03 (149866.04–323872.59) | 14.75 (9.58–20.72) | −0.13 (−0.24–0.03) |
| Male | YLD | 100827.38 (65628.28–142789.55) | 14.92 (9.71–21.12) | 209649.92 (136703.92–298658.34) | 14.18 (9.24–20.2) | −0.1 (−0.2–0) |
| Female | YLLs | 192629.14 (142139.23–259151.26) | 28.05 (20.77–37.57) | 395566.14 (309709.05–507150.29) | 24.08 (18.81–31.05) | −0.44 (−0.55–0.33) |
| Male | YLLs | 203064.45 (148905.06–274623.85) | 33.86 (25.11–45.12) | 396226.39 (318788.22–513662.12) | 28.39 (22.87–36.63) | −0.53 (−0.58–0.47) |
| AD | ||||||
| Female | DALYs | 9190019.95 (4028552.1–19850346.92) | 1459.49 (632.99–3148.87) | 26015752.09 (11586941.09–53781723.99) | 1516.77 (677.49–3136.53) | 0.08 (0.05–0.1) |
| Male | DALYs | 4294423.07 (1895657.26–9674587.43) | 1027.2 (443.64–2305.27) | 13635201.11 (5898371.71–30314599.17) | 1100.66 (471.29–2453.14) | 0.21 (0.19–0.23) |
| Female | Deaths | 473779.43 (113734.53–1238999.09) | 81.61 (19.67–211.91) | 1492038.54 (380746.37–3658868.93) | 85.53 (21.81–210.01) | 0.11 (0.09–0.14) |
| Male | Deaths | 192362.13 (43878.44–528189.79) | 56.53 (13.01–152.46) | 705509.7 (160627.7–1892238.76) | 62.05 (14.17–165.86) | 0.3 (0.27–0.32) |
| Female | Incidence | 2433152.52 (1733627.57–3317426.15) | 369.52 (264.32–502.16) | 6567367.14 (4652680.73–8981567.22) | 387.68 (274.4–530.5) | 0.08 (0.05–0.11) |
| Male | Incidence | 1303998.62 (907301.64–1804192.42) | 289.07 (203.68–397.04) | 3919258.74 (2734929.05–5395495.8) | 303.89 (212.98–417.45) | 0.11 (0.09–0.13) |
| Female | Prevalence | 13744965.73 (10809963.06–17188290.29) | 2108.62 (1660.57–2631.05) | 38015085.94 (29768465.43–47630266.78) | 2238.08 (1751.45–2806.41) | 0.1 (0.07–0.13) |
| Male | Prevalence | 7373054.25 (5741891.98–9307711.92) | 1636.57 (1279.27–2057.76) | 22261989.12 (17282207.83–28114077.78) | 1729.11 (1343.34–2182.12) | 0.12 (0.1–0.14) |
| Female | YLDs | 2850155.99 (1919404.24–3997049.87) | 441.31 (297.34–615.85) | 7971459.49 (5359107.28–11144013.56) | 468.27 (314.67–655.66) | 0.1 (0.07–0.13) |
| Male | YLDs | 1376418.13 (899299.04–1942371.02) | 312.89 (205.2–437.1) | 4232529.11 (2764088.28–5935041.6) | 332.05 (217–464.17) | 0.13 (0.11–0.16) |
| Female | YLLs | 6339863.96 (1494887.62–16857526.71) | 1018.18 (241.45–2688.11) | 18044292.6 (4515498.83–45167292.32) | 1048.51 (261.95–2628.89) | 0.07 (0.05–0.09) |
| Male | YLL | 2918004.94 (654217.37–8225845.09) | 714.31 (162.5–1965.87) | 9402671.99 (2111904.52–25584468.51) | 768.61 (173.51–2078.79) | 0.24 (0.22–0.27) |
UI: uncertainty interval; EAPC: estimated annual percentage change; DALYs: disability-adjusted life years; YLDs: years lived with disability; YLLs: years of life lost; IBD: inflammatory bowel disease; AD: Alzheimer’s disease.
Differences in IBD and AD across SDI levels
The SDI data for IBD indicate distinct patterns in disease burden between 1990 and 2021. High SDI regions initially exhibited the highest absolute DALY counts and rates with 369,892 DALYs (95% UI: 308,026–442,380) and an age-standardized rate of 54.81 per 100,000 in 1990, which decreased slightly over time (EAPC: −0.02). In contrast, middle SDI regions experienced a substantial increase in total DALYs, increasing from 34,479 in 1990 to 73,910 in 2021 with a significant reduction in age-standardized rates (EAPC: −1.10). Low SDI regions had a lower absolute burden but also demonstrated a decline in rates (EAPC: −0.36). The high-middle SDI group had intermediate initial burden levels but had notable decreases in standardized rates (EAPC: −0.86). These trends suggested that high SDI countries initially bore the greatest burden but the relative burden decreased modestly over time, possibly reflecting improvements in healthcare and disease management. Conversely, middle and lower SDI regions have increasing total burdens, highlighting disparities in disease prevalence, detection, and healthcare access across socio-economic strata. Overall, these findings underscore the importance of tailored public health strategies to address the evolving landscape of IBD burden across different socioeconomic levels (Figure 3A, B). In addition to descriptive comparisons, whether temporal trends in age-standardized DALY rates differed across SDI strata was formally evaluated by fitting linear regression models of log-transformed rates on calendar year with an interaction term for SDI level. The global test for heterogeneity in EAPCs across SDI categories was statistically significant [p_global < 0.001], indicating that the modest decline that occurred in high-SDI regions differed significantly from the steeper declines in middle- and low-SDI regions.
Figure 3 Distribution of IBD- and AD-related indicators across SDI regions in GBD 2021 data. (A) and (B) show the variation in IBD burden across different SDI regions with (A) illustrating age-standardized rates (DALYs, deaths, and incidence) and (B) displaying the number of cases. (C) and (D) depict the corresponding distribution for AD with (C) presenting age-standardized rates and (D) showing the number of cases across SDI regions. These figures highlight how disease burden varies with sociodemographic development levels for IBD and AD.
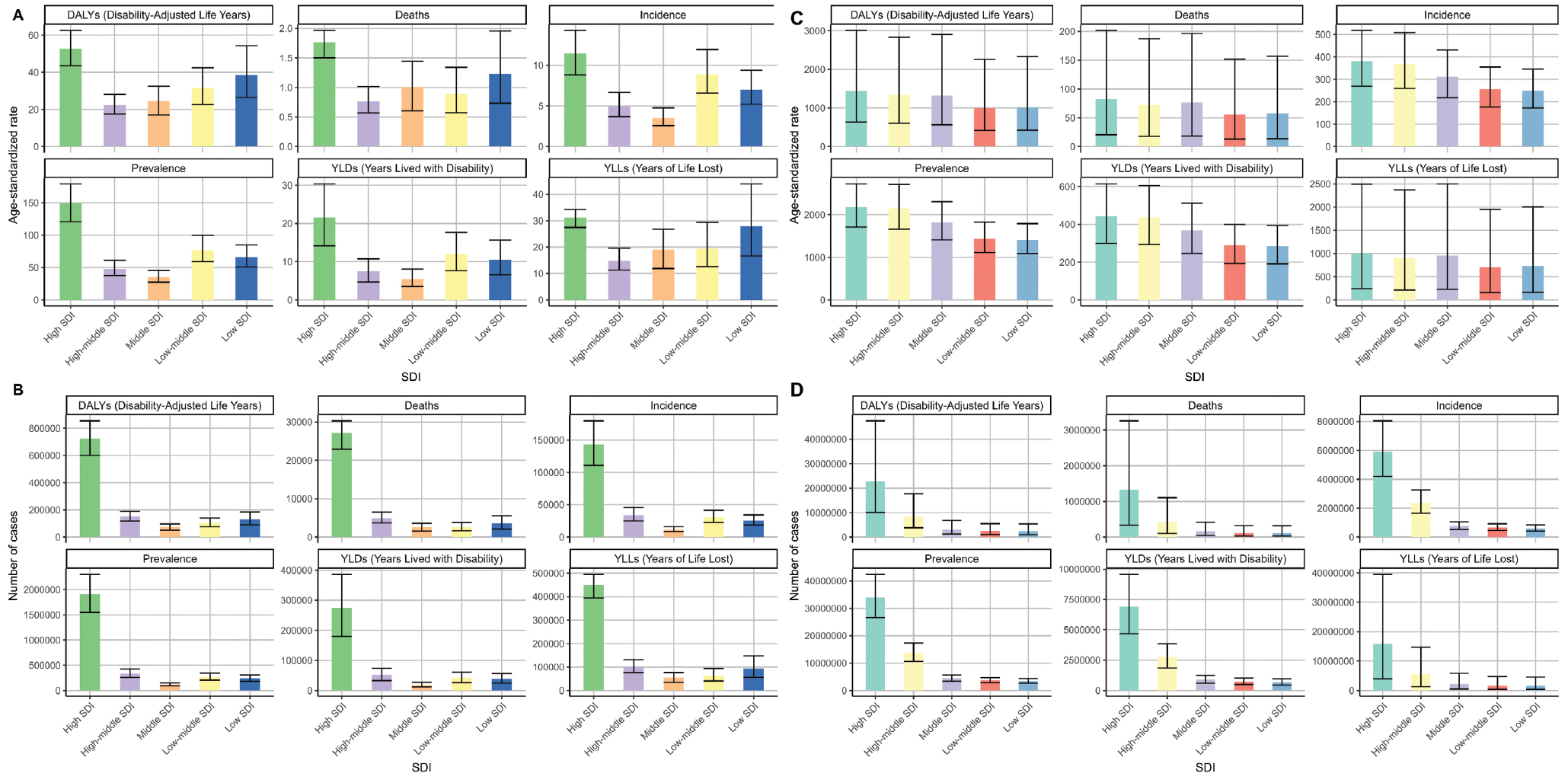
The SDI level and burden of AD data from 1990–2021 showed that high SDI countries initially had the highest absolute DALYs (approximately 8.55 million in 1990) with a rate of 1,402.56 per 100,000, increasing to > 22.75 million cases by 2021 with a slight rate increase (EAPC: 0.04). High-middle SDI regions also experienced substantial growth with DALYs rising from 2.06 million to > 8.36 million and a modest rate increase (EAPC: 0.05). Conversely, lower SDI regions started with smaller burdens but had significant proportional increases with DALYs increasing from 769,000 to 2.41 million and higher rates (EAPC: 0.45), indicating a faster relative increase in disease burden. Middle SDI regions followed similar trends with DALYs increasing from 881,569 to > 3 million and a steady rate increase (EAPC: 0.46). Overall, while high SDI countries maintain the highest absolute burden, lower SDI regions are experiencing more rapid growth in AD burden, reflecting disparities in disease prevalence, detection, and healthcare resources (Figure 3C, D). Similarly, the global heterogeneity test for EAPCs across SDI categories was statistically significant [p_global < 0.001], driven by faster increases in age-standardized DALY rates in low- and middle-SDI regions compared to the relatively stable trends in high-SDI regions. These findings support the presence of genuine regional heterogeneity in the temporal evolution of AD burden.
Forecasted risk factors for IBD and AD
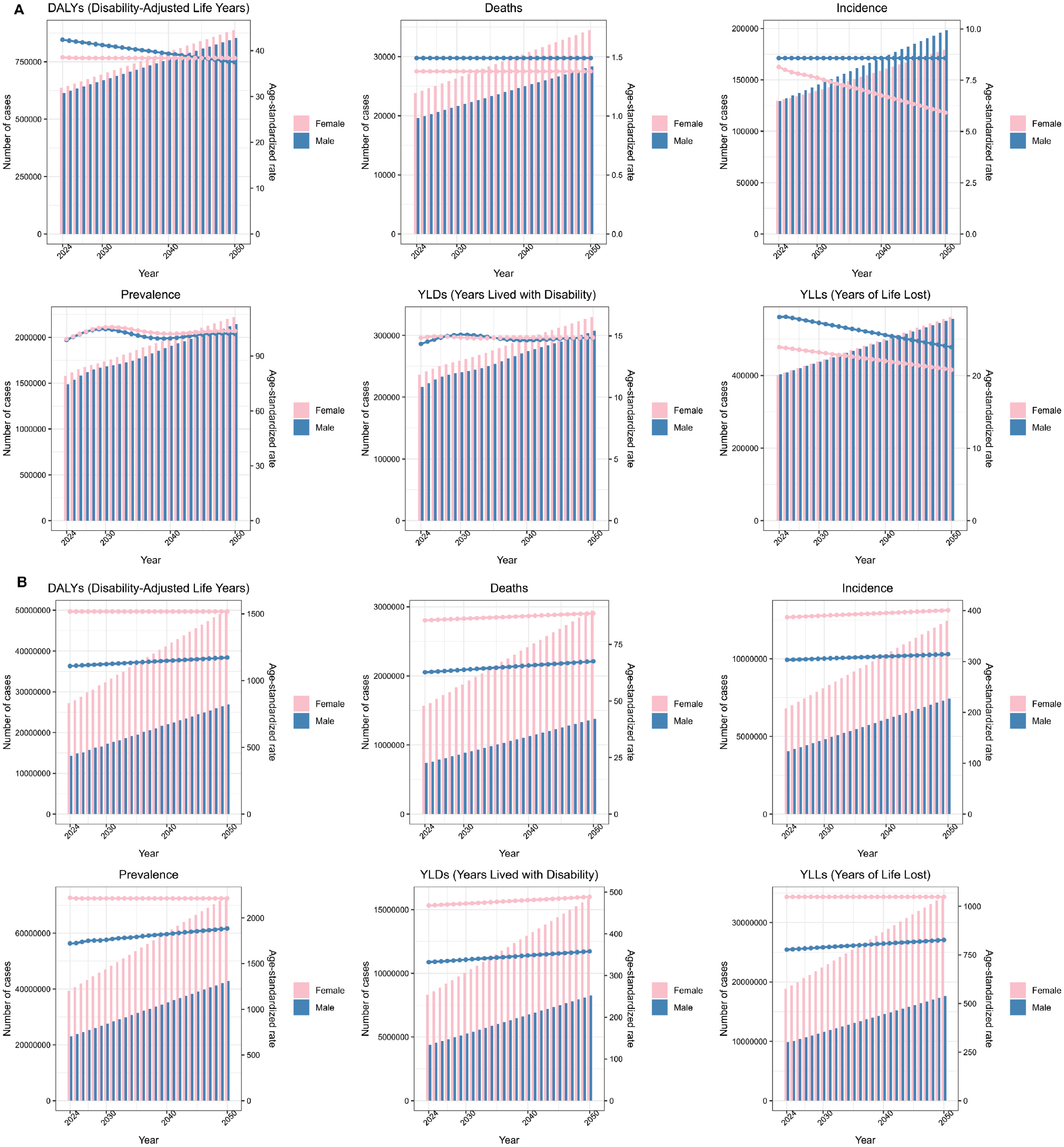
The ARIMA forecasts for IBD risk factors from 2024–2050 indicate a steady increase in disease burden across both genders. Female DALYs are projected to rise from approximately 635,794 in 2024 to > 887,806 in 2050 with similar upward trends occurring in males, increasing from 615,027 to > 852,955 during the same period. The forecasted incidence rates for females are expected to grow from 129,737 cases in 2024 to nearly 222,381 cases by 2050, while males are projected to increase from approximately 129,465 to > 214,351 cases. Similarly, the prevalence of IBD is forecasted to increase significantly with females increasing from 1.58 million to > 3.3 million cases and males from approximately 1.49 million to > 3.1 million cases between 2024 and 2050. The YLLs also had an upward trend with females increasing from 402,000 to > 561,000 and males from 403,000 to > 556,000 over the forecast period (Figure 4A). The YLLs forecasts for AD from 2024–2050 project a continuous increase in disease burden across both genders. Female DALYs are expected to grow from approximately 27.2 million in 2024 to > 34.3 million in 2050 with a corresponding increase in incidence from 6.8 million to nearly 14 million cases. Male DALYs are forecasted to increase from 14.3 million to > 17.6 million with the incidence increasing from 4.0 million to > 7.6 million cases. The total YLLs for females are projected to rise from 18.9 million to > 26.5 million, while for males the total YLLs are projected to increase from 9.87 million to > 13.8 million during the same period. Prevalence estimates indicated that the number of individuals affected will grow substantially with females increasing from 39.4 million to > 43.3 million and males from 23.1 million to > 27.6 million by 2050. These forecasts highlight a significant and ongoing increase in AD burden globally, underscoring the need for enhanced healthcare preparedness and resource allocation to manage the increasing impact of the disease over the coming decades (Figure 4B).
Figure 4 Predicted number of cases for IBD- and AD-related indicators in GBD 2021 data. (A) displays the forecasted values of six indicators (DALYs, deaths, incidence, prevalence, YLDs, and YLLs) for IBD separated by gender (female and male) using the ARIMA method. (B) shows the corresponding predicted values for AD with the same six indicators and gender-specific data, which were also generated via ARIMA. These projections provide insights into future trends of disease burden across different health metrics and genders for IBD and AD.
Influence of risk factors on the IBD and AD burden
MR analyses were performed to assess the causal effects of multiple risk factors on IBD and AD, using the IVW (fixed effects) method as the primary analytic strategy. From this comprehensive assessment, three overlapping factors (beef intake, coffee consumption, and educational attainment) were shown to be significantly associated with the risk of both diseases, as summarized in Table 3.
Table 3 MR Estimates (IVW and Fixed Effects) for Overlapping Risk Factors
| Exposure | Outcome | Beta | Standard Error | P-value | Odds Ratio | 95% CI (Lower) | 95% CI (Upper) |
|---|---|---|---|---|---|---|---|
| Beef intake | IBD | −0.72 | 0.31 | 0.018 | 0.48 | 0.27 | 0.88 |
| Beef intake | AD | −6.73 | 0.38 | 8.02 × 10−72 | 0.0012 | 0.0006 | 0.0025 |
| Coffee consumption | IBD | 0.18 | 0.05 | 0.0003 | 1.20 | 1.09 | 1.33 |
| Coffee consumption | AD | 0.18 | 0.06 | 0.005 | 1.19 | 1.05 | 1.35 |
| Educational attainment | IBD | −0.14 | 0.04 | 0.0008 | 0.87 | 0.80 | 0.94 |
| Educational attainment | AD | −0.20 | 0.05 | 1.79 × 10−4 | 0.82 | 0.74 | 0.91 |
MR: Mendelian randomization; IVW: inverse variance weighted; IBD: inflammatory bowel disease; AD: Alzheimer’s disease.
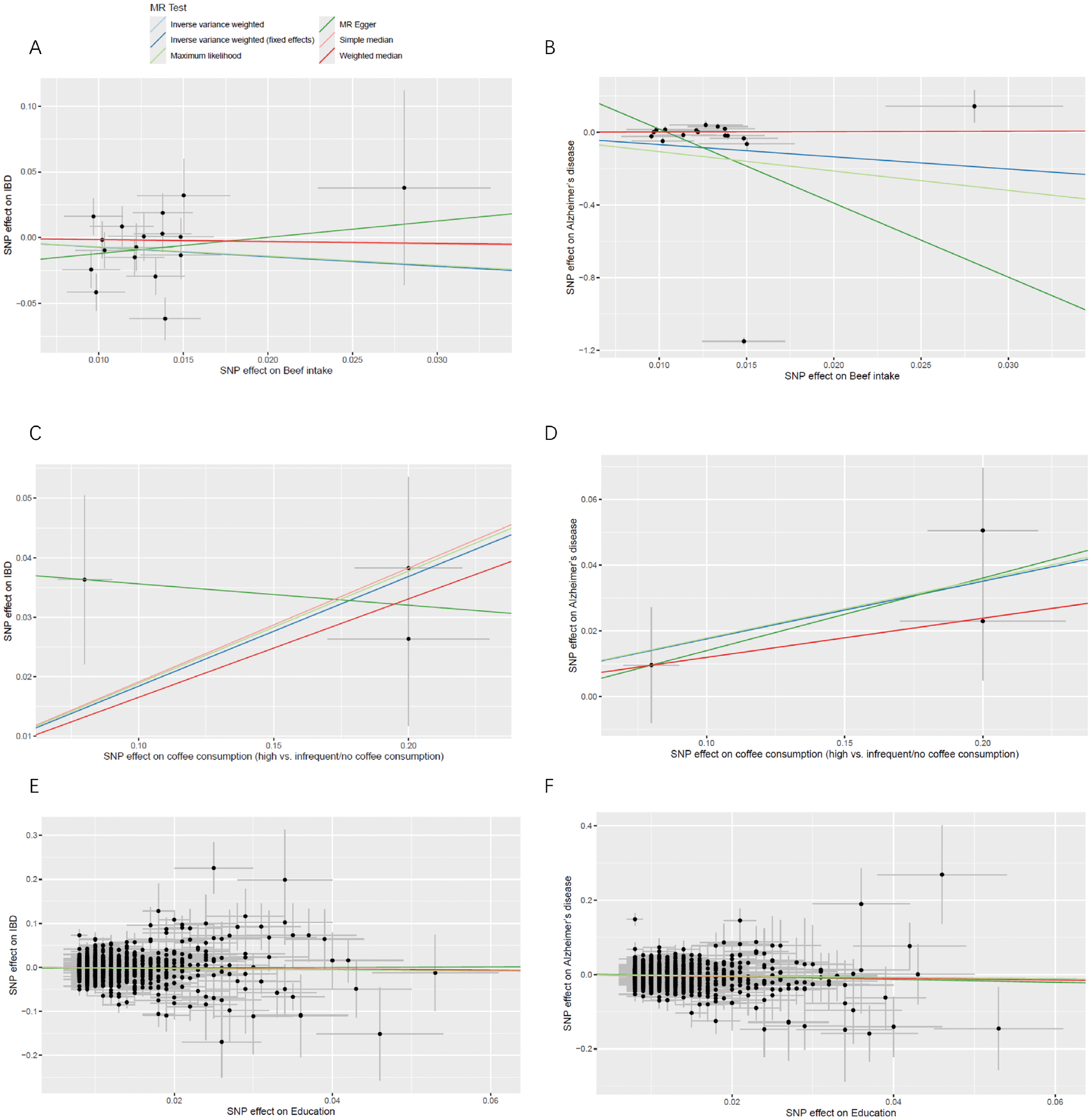
Specifically, higher genetically predicted beef intake was associated with a significantly reduced risk of IBD (β = −0.72, SE = 0.31, P = 0.018; OR = 0.48, 95% CI: 0.27–0.88) and AD (β = −6.73, SE = 0.38, P < 0.0001; OR = 0.0012, 95% CI: 0.0006–0.0025; Figure 5A, B), indicating a potential protective effect. In contrast, higher genetically predicted coffee consumption (high vs. infrequent/no consumption) was significantly associated with increased risk for IBD (β = 0.18, SE = 0.05, P = 0.0003; OR = 1.20, 95% CI: 1.09–1.33) and AD (β = 0.18, SE = 0.06, P = 0.005; OR = 1.19, 95% CI: 1.05–1.35; Figure 5C, D), suggesting that elevated coffee intake may be a risk factor for both disorders. Moreover, higher genetically predicted educational attainment demonstrated a protective association and was linked to lower risks of IBD (β = −0.14, SE = 0.04, P = 0.0008; OR = 0.87, 95% CI: 0.80–0.94) and AD (β = −0.20, SE = 0.05, P = 1.79 × 10−4; OR = 0.82, 95% CI: 0.74–0.91; Figure 5E, F).
Figure 5 Mendelian randomization analysis examining the associations of lifestyle and educational factors with IBD and AD risk. (A) and (B) display scatter plots illustrating the inverse association between genetically predicted beef intake and the risk of IBD and AD. (C) and (D) show the positive association between genetically predicted coffee consumption (comparing high versus infrequent/no consumption) and the risks of IBD and AD, respectively. (E) and (F) depict the inverse relationship between genetically predicted educational attainment and the risks of IBD and AD, respectively.
Shared inflammatory transcriptomic signatures between IBD and AD
In the colonic mucosa dataset 1247 DEGs associated with IBD were identified compared to non-IBD controls (713 upregulated and 534 downregulated; FDR < 0.05, |log2FC| ≥ 1). In the temporal cortex dataset 1038 DEGs were associated with AD compared to cognitively normal controls (612 up-and 426 down-regulated). Intersection analysis revealed 146 genes that were significantly dysregulated in IBD and AD, of which 112 (76.7%) had a concordant direction of change (i.e., up-or down-regulated in IBD and AD).
Pathway enrichment analysis of these 146 shared DEGs demonstrated significant over-representation of innate and adaptive immune pathways, including the TNF signaling pathway (KEGG; FDR = 2.1 × 10−4), NF-κB signaling pathway (FDR = 4.6 × 10−4), cytokine–cytokine receptor interaction (FDR = 7.8 × 10−4), and regulation of leukocyte activation (GO; FDR = 1.3 × 10−3). Consistent with these findings, the shared DEG set was significantly enriched for curated immune-related gene sets, particularly the DEGs involved in innate immune responses and cytokine signaling (all FDR < 0.05). Notably, several key inflammatory mediators (e.g., TNFRSF1A, IL1B, CCL2, and CXCL8) and regulators of microglial/monocytic activation (e.g., TREM2 and TYROBP) were consistently upregulated across both tissues, suggesting convergent activation of myeloid-driven inflammatory programs. Conversely, a subset of shared downregulated genes was enriched for synaptic function and neuronal signaling pathways (e.g., synaptic vesicle cycle [FDR = 3.4 × 10−3]), indicating that chronic inflammatory signaling may be mechanistically linked to neuronal dysfunction.
Taken together, these transcriptomic findings provided orthogonal biological support for the epidemiologic observations, indicating that IBD and AD share overlapping inflammatory and immune-related molecular signatures despite involving distinct primary organs. This convergence on TNF/NF-κB–centered pathways may help explain the parallel increases in disease burden and highlights potentially shared therapeutic targets that warrant further mechanistic investigation.
Discussion
This study provides a multifaceted examination of the global burden, epidemiologic trends, and potential causal risk factors associated with IBD and AD, two major health conditions with increasing prevalence worldwide. Leveraging data from the GBD 2021, both diseases experienced notable increases in absolute burden over the past 3 decades with AD showing a more pronounced rise in total DALYs and age-standardized rates, particularly among older populations and high SDI regions. These findings highlight the growing public health challenge posed by neurodegenerative diseases in aging societies and underscore the importance of targeted prevention strategies.
Our analysis demonstrated notable heterogeneity in the burden of IBD and AD across different demographic groups, emphasizing the importance of tailored public health strategies. The higher burden of AD observed in females and older age groups aligns with well-established demographic patterns, reflecting biological, social, and healthcare access factors [15, 16]. Women generally have longer life expectancy, which increases the cumulative risk of age-related neurodegenerative diseases, such as AD [17]. In addition, hormonal differences and genetic predispositions may contribute to the observed gender disparities [18]. The pronounced increase in AD burden among the elderly underscores the critical impact of aging populations globally, highlighting the necessity for age-specific interventions and healthcare planning [19].
In contrast, IBD displayed a relatively stable but slightly declining age-standardized rate over the study period, which may reflect improvements in disease management, early diagnosis, and increased availability of effective therapies that reduce the progression and disability associated with the condition [20, 21]. Stabilization of the IBD burden suggests that advances in medical care could be mitigating the overall impact on populations, despite an increase in the prevalence [22, 23]. However, regional disparities persist and the burden remains significant, especially in low- and middle-income countries where healthcare resources and awareness may be limited.
Furthermore, the results revealed that the burden of both diseases increases markedly with age, particularly beyond 40 years of age, with the highest rates occurring in the oldest age groups (85+ years). The steep age-related increase in DALYs and rates emphasizes the profound influence of aging on disease susceptibility and severity [24]. This trend for AD is expected due to neurodegenerative processes that accelerate with age, but the rising burden of IBD in the elderly also warrants attention [25]. Age-related immune dysregulation, co-morbidities, and polypharmacy may exacerbate disease progression and complicate management in older adults.
Sociodemographic factors further modulate disease burden. High SDI regions, characterized by higher healthcare access and longer life expectancy, exhibit higher absolute DALYs for AD, partly due to demographic shifts toward older populations [26, 27]. Conversely, lower SDI regions, although currently showing lower absolute burdens, are experiencing faster increases in disease rates that are likely driven by demographic transitions, urbanization, and lifestyle changes [28, 29]. Higher SDI countries have higher absolute IBD DALYs and rates, which is consistent with the observed global epidemiologic pattern, in which urbanized and economically developed regions report a higher IBD prevalence, possibly due to environmental and dietary factors [30].
Importantly, the epidemiologic evidence and biological plausibility support a close link between IBD and AD. Population-based studies and meta-analyses indicate that individuals with IBD are at a higher risk of developing AD and other neurodegenerative conditions, potentially driven by shared inflammatory pathways and gut microbiome dysbiosis [9, 25]. The role of systemic inflammation and alterations in gut microbiota in contributing to neuroinflammation and neurodegeneration is increasingly recognized, suggesting common pathogenic mechanisms [31]. Recent MR analyses further support a bidirectional causal relationship, implying that systemic inflammation and gut-derived metabolites may influence neurodegenerative processes, while neuroinflammation may impact gastrointestinal health [32, 33]. These insights underscore the interconnected nature of gut-brain axis pathways and highlight the potential for integrated therapeutic approaches.
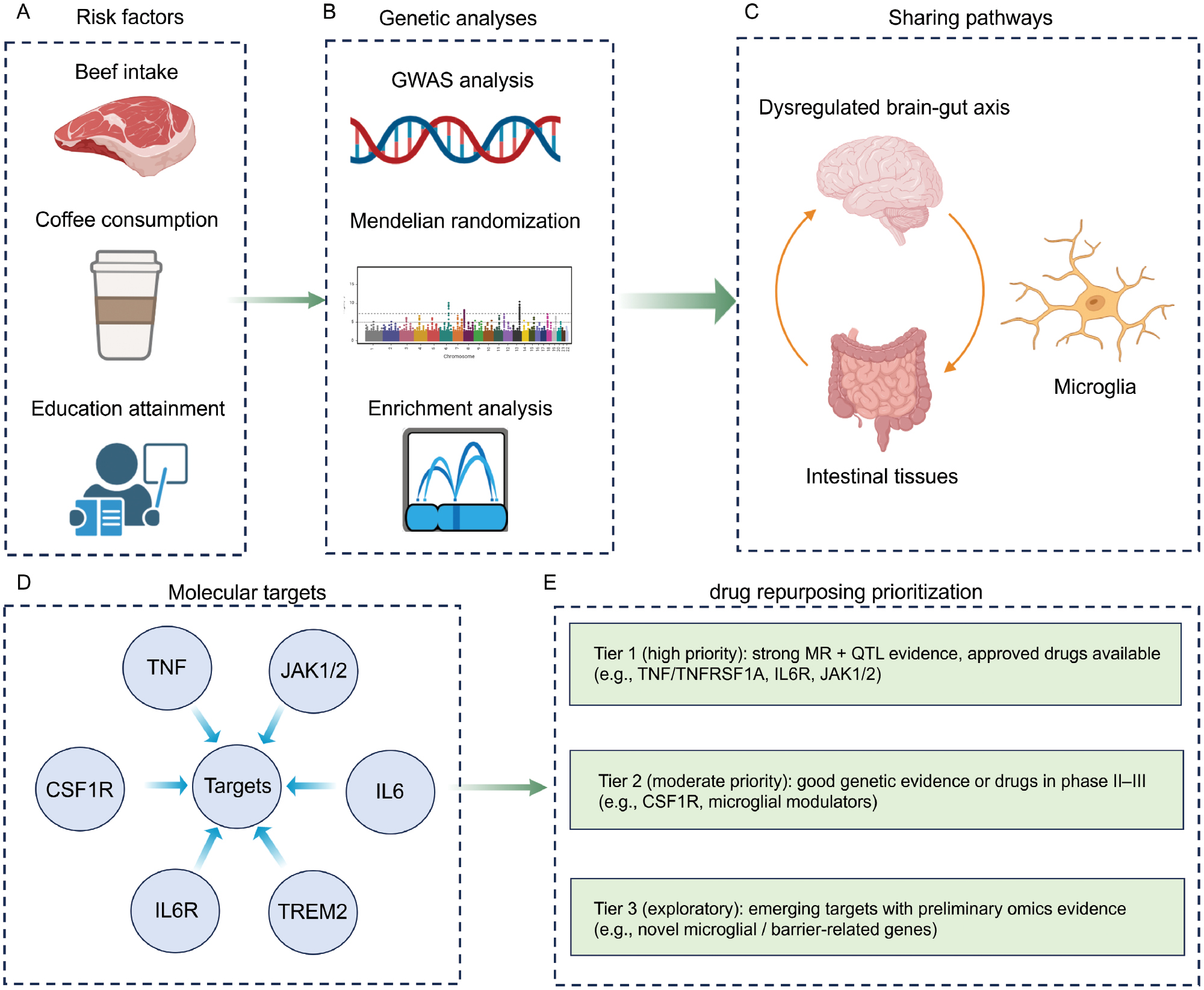
The MR findings suggested that higher genetically predicted beef intake may have a protective effect against IBD and AD, potentially due to the rich content of high-quality protein, micronutrients, and amino acids that support immune and neurologic health, although the exact mechanisms warrant further investigation [34–36]. Conversely, increased genetically predicted coffee consumption was associated with higher risks of both diseases, which may reflect genetic influences on caffeine metabolism, individual responses, or the potential irritant effects of caffeine on the gut and impact on neuroinflammation [37, 38]. In addition, higher educational attainment demonstrated a protective effect, aligning with literature linking cognitive reserve and health literacy to disease risk reduction [39, 40]. These results highlighted the complex and nuanced relationship between diet, lifestyle, and disease, emphasizing that while some dietary factors may be beneficial, other factors could pose risks depending on individual genetics and consumption patterns. Further research is needed to clarify these pathways and inform personalized dietary recommendations for disease prevention. Based on MR and following genetic analyses, we propose a conceptual roadmap for druggable targets and drug repurposing opportunities across IBD and AD (Figure 6), mapping causal pathways to existing pharmacologic modulators and prioritizing targets for subsequent experimental and clinical validation.
Figure 6 Roadmap from genetic informed pathways to druggable targets and repurposing priorities. (A) Risk factors, (B) Genetic analyses, (C) Sharing pathways, (D) Molecular targets, (E) Drug repurposing prioritization.
Although broadly increasing burdens of IBD and AD were noted at the global level, the incidence patterns in China were not entirely concordant, suggesting that contextual factors may modulate these trends. Differences in diagnostic capacity, health-care access, population aging, urbanization, and environmental exposures may differentially affect IBD and AD incidence in China compared to other regions [41–43]. Moreover, changes in awareness and screening practices, particularly for dementia, could lead to apparent increases in AD diagnoses that are not solely driven by true changes in disease risk. These discrepancies highlight that our ecologic findings at the global level cannot be directly extrapolated to all countries and underscore the need for country-specific studies that incorporate local health-system and environmental determinants when interpreting temporal trends in IBD and AD.
The observed negative association between beef intake and the risk of IBD and AD should be interpreted with caution. Although MR reduces confounding by many measured and unmeasured factors at the individual level, residual confounding cannot be fully excluded. Higher beef consumption may cluster with specific dietary patterns (e.g., higher overall protein and calorie intake, different fat quality, or concomitant intake of other protective nutrients) and lifestyle characteristics, as well as higher socioeconomic status and better access to medical care, which may independently influence IBD and AD risk. In addition, cultural and regional differences in beef preparation methods and co-consumed foods could modify any true causal effect [44, 45]. Therefore, the inverse association that was detected may partly reflect broader patterns of diet and living conditions rather than a direct protective effect of beef. Therefore, future mechanistic and interventional studies are required to disentangle these pathways.
Our projection model extrapolated historical temporal trends in disease burden under the assumption that the underlying drivers of IBD and AD incidence and mortality would remain broadly similar over the projection horizon. Indeed, the predicted future burden represents a continuation of past patterns in the absence of major structural changes in risk-factor exposure, diagnostic practices, or the implementation of highly effective new preventive or therapeutic strategies. Consequently, the forecasts should be interpreted as scenario-based projections rather than precise predictions of what will occur. Any substantial public-health interventions, shifts in lifestyle and environmental exposures, or breakthroughs in IBD and AD treatment could lead to future trajectories that deviate markedly from our estimates. This limitation underscores the need to regularly update projections as new data and interventions emerge, and to view our results primarily as a baseline against which the potential impact of future policies and therapies can be evaluated.
The strengths of the current study include the comprehensive use of large-scale global data, advanced statistical modeling for future projections, and the application of MR to infer causality between risk factors and disease outcomes. Nevertheless, the limitations should be acknowledged. The reliance on GWAS data predominantly from European populations may limit generalizability to other ethnicities. MR assumptions, such as no horizontal pleiotropy, although tested, cannot be entirely excluded. In addition, observational data from GBD cannot capture all nuances of exposures and behaviors at the level of the individual.
Conclusion
Our findings reinforce the importance of considering IBD and AD within a shared pathogenic framework, emphasizing the role of systemic inflammation and gut microbiota. The identification of modifiable risk factors through MR offers promising avenues for preventive interventions. Future prospective studies should explore the biological mechanisms linking these diseases and evaluate targeted strategies to mitigate the rising global burden. An integrated approach addressing lifestyle, dietary, and socio-economic factors holds potential for reducing the impact of these complex conditions on individuals and healthcare systems worldwide.
Data availability statement
The data used in this study were obtained from the Global Burden of Disease (GBD) 2021 study. The GBD 2021 dataset is publicly accessible and can be downloaded from the Institute for Health Metrics and Evaluation (IHME) website (https://ghdx.healthdata.org/gbd-2021). Specific data queries and analyses can be performed using the GBD Results Tool, which provides comprehensive information on incidence, prevalence, mortality, and disability-adjusted life years (DALYs) for various diseases and conditions across different regions and demographics.
Ethics statement
This study was approved by Wenzhou Medical University with approval number 2024-SCYJ-007. The University Ethics Board granted a waiver for informed consent because the research only involved data analysis and did not contain any identifiable personal information.
Author contributions
Zhongpeng Dai, Sisi Wang: Conceptualization, methodology, data analysis, and manuscript writing; Qiang Li: Conceptualization, methodology, data analysis, and manuscript writing; Wenyuan Wang, Ping Wu, Xun Chen, Jiping Wei, Yuqing Li, Wenjie Hu: Data collection, statistical analysis, and manuscript editing; Wen-Jia Wang: Data visualization; Chen Gao: Project administration and coordination; Quan Zhang: Supervision and critical review of the manuscript; Zun-Yong Feng, Xiao-Kun Li, and Zhou-Guang Wang: Manuscript writing and overall project oversight; Liuxi Chu: Conceptual guidance, manuscript writing, overall project oversight, and funding acquisition.
Funding
This study was supported by the Ningbo Natural Science Foundation (2024J313) and the National Natural Science Foundation of China (82401829).
Acknowledgments
The Graphical abstract and figure 6 were created by BioRender. https://BioRender.com.
Conflict of interest
The authors declare that there are no conflicts of interest.
Consent to publish declaration
Not applicable.
Supplementary materials
Supplementary Material can be downloaded from https://bio-integration.org/wp-content/uploads/2026/05/bioi20260023_Supplemental.pdf.
Graphical abstract
Highlights
- GBD 2021 shows parallel increases in IBD and AD burden globally.
- MR identifies education, coffee, and beef as shared causal factors.
- Shared TNF/NF-κB transcriptomic signatures in the gut and brain.
In brief
This study integrated global burden of disease data, Mendelian randomization, and transcriptomic cross-validation to show that inflammatory bowel disease and Alzheimer’s disease share convergent epidemiology and causal risk factors. Parallel increases in burden from 1990–2021, protective effects of higher education and beef intake, and detrimental effects of coffee consumption were observed for both diseases. Shared dysregulation of TNF/NF-κB pathways in gut and brain tissues provided biological plausibility, suggesting that coordinated prevention strategies targeting chronic inflammation along the gut–brain axis may mitigate both conditions.
References
- Meyer A, Agrawal M, Savin-Shalom E, Wong ECL, Levinson C, et al. Impact of diet on inflammatory bowel disease risk: systematic review, meta-analyses and implications for prevention. EClinicalMedicine 2025;86:103353. [PMID: 40697960 DOI: 10.1016/j.eclinm.2025.103353]
- Ryan NS. Alzheimer’s disease in Down syndrome: progress and promise. Lancet Neurol 2025;24(9):717-8. [PMID: 40818465 DOI: 10.1016/S1474-4422(25)00276-5]
- Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol 2021;18(1):56-66. [PMID: 33033392 DOI: 10.1038/s41575-020-00360-x]
- Rafii MS, Schlachetzki Z, Barroeta I, Head E, Fortea J, et al. Down syndrome and Alzheimer’s disease: insights into biomarkers, clinical symptoms, and pathology. Lancet Neurol 2025;24(9):753-62. [PMID: 40818475 DOI: 10.1016/s1474-4422(25)00237-6]
- Dolinger M, Torres J, Vermeire S. Crohn’s disease. Lancet 2024;403(10432):1177-91. [PMID: 38437854 DOI: 10.1016/S0140-6736(23)02586-2]
- GBD 2016 Dementia Collaborators. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019;18(1):88-106. [PMID: 30497964 DOI: 10.1016/S1474-4422(18)30403-4]
- Pradeepkiran JA, Reddy PH. Defective mitophagy in Alzheimer’s disease. Ageing Res Rev 2020;64:101191. [PMID: 33022416 DOI: 10.1016/j.arr.2020.101191]
- Aggarwal M, Alkhayyat M, Abou Saleh M, Sarmini MT, Singh A, et al. Alzheimer disease occurs more frequently in patients with inflammatory bowel disease: insight from a nationwide study. J Clin Gastroenterol 2023;57(5):501-7. [PMID: 35470286 DOI: 10.1097/MCG.0000000000001714]
- Szandruk-Bender M, Wiatrak B, Szeląg A. The risk of developing Alzheimer’s disease and Parkinson’s disease in patients with inflammatory bowel disease: a meta-analysis. J Clin Med 2022;11(13):3704. [PMID: 35806985 DOI: 10.3390/jcm11133704]
- Burgess S, Thompson SG. Mendelian randomization: methods for causal inference using genetic variants. 2nd ed. Boca Raton, FL: CRC Press; 2021. pp. 240. [DOI: 10.1201/9780429324352]
- Gupta V, Walia GK, Sachdeva MP. ‘Mendelian randomization’: an approach for exploring causal relations in epidemiology. Public Health 2017;145:113-9. [PMID: 28359378 DOI: 10.1016/j.puhe.2016.12.033]
- Jiang L, Li JC, Shen L, Tang BS, Guo JF. Association between inflammatory bowel disease and Alzheimer’s disease: multivariable and bidirectional Mendelian randomisation analyses. Gut 2023;72(9):1797-9 [PMID: 37549984 DOI: 10.1136/gutjnl-2022-327860]
- Wang D, Zhang X, Du H. Inflammatory bowel disease: a potential pathogenic factor of Alzheimer’s disease. Prog Neuropsychopharmacol Biol Psychiatry 2022;119:110610. [PMID: 35908596 DOI: 10.1016/j.pnpbp.2022.110610]
- Xu L, Wang Z, Li Q. Global trends and projections of Parkinson’s disease incidence: a 30-year analysis using GBD 2021 data. J Neurol 2025;272(4):286 [PMID: 40131471 DOI: 10.1007/s00415-025-13030-2]
- Mielke MM, Aggarwal NT, Vila-Castelar C, Agarwal P, Arenaza-Urquijo EM, et al. Consideration of sex and gender in Alzheimer’s disease and related disorders from a global perspective. Alzheimers Dement 2022;18(12):2707-24. [PMID: 35394117 DOI: 10.1002/alz.12662]
- Wiese LAK, Gibson A, Guest MA, Nelson AR, Weaver R, et al. Global rural health disparities in Alzheimer’s disease and related dementias: state of the science. Alzheimers Dement 2023;19(9):4204-25. [PMID: 37218539 DOI: 10.1002/alz.13104]
- Hou Y, Dan X, Babbar M, Wei Y, Hasselbalch SG, et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019;15(10):565-81. [PMID: 31501588 DOI: 10.1038/s41582-019-0244-7]
- Bianco A, Antonacci Y, Liguori M. Sex and gender differences in neurodegenerative diseases: challenges for therapeutic opportunities. Int J Mol Sci 2023;24:6354. [PMID: 37047320 DOI: 10.3390/ijms24076354]
- Deng Y, Wang H, Gu K, Song P. Alzheimer’s disease with frailty: prevalence, screening, assessment, intervention strategies and challenges. Biosci Trends 2023;17(4):283-92. [PMID: 37612122 DOI: 10.5582/bst.2023.01211]
- Zhou JL, Bao JC, Liao XY, Chen YJ, Wang LW, et al. Trends and projections of inflammatory bowel disease at the global, regional and national levels, 1990–2050: a Bayesian age-period-cohort modeling study. BMC Public Health 2023;23(1):2507. [PMID: 38097968 DOI: 10.1186/s12889-023-17431-8]
- Liu Y, Li J, Yang G, Meng D, Long X, et al. Global burden of inflammatory bowel disease in the elderly: trends from 1990 to 2021 and projections to 2051. Front Aging 2024;5:1479928. [PMID: 39512627 DOI: 10.3389/fragi.2024.1479928]
- Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol 2015;12(12):720-7. [PMID: 26323879 DOI: 10.1038/nrgastro.2015.150]
- Kaplan GG. The global burden of inflammatory bowel disease: from 2025 to 2045. Nat Rev Gastroenterol Hepatol 2025;22(10):708-20. [PMID: 40681759 DOI: 10.1038/s41575-025-01097-1]
- Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL. Measuring population ageing: an analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019;4(3):e159-67. [PMID: 30851869 DOI: 10.1016/S2468-2667(19)30019-2]
- Zong J, Yang Y, Wang H, Zhang H, Yang X, et al. The two-directional prospective association between inflammatory bowel disease and neurodegenerative disorders: a systematic review and meta-analysis based on longitudinal studies. Front Immunol 2024;15:1325908. [PMID: 38720896 DOI: 10.3389/fimmu.2024.1325908]
- Liu W, Deng W, Gong X, Ou J, Yu S, et al. Global burden of Alzheimer’s disease and other dementias in adults aged 65 years and over, and health inequality related to SDI, 1990–2021: analysis of data from GBD 2021. BMC Public Health 2025;25(1):1256. [PMID: 40181335 DOI: 10.1186/s12889-025-22378-z]
- Yuan M, Jin L, Fang Y. Disease burden, temporal trends, and cross-country inequality associated with sociodemographic indicators in Alzheimer’s disease and other dementias. Am J Prev Med 2025;68(4):682-94. [DOI: 10.1016/j.amepre.2024.12.011]
- Bai J, Cui J, Shi F, Yu C. Global epidemiological patterns in the burden of main non-communicable diseases, 1990–2019: relationships with socio-demographic index. Int J Public Health 2023;68:1605502. [PMID: 36726528 DOI: 10.3389/ijph.2023.1605502]
- Zhang Y, Zhang XB, Ding YW, Kong Y, Zhu XF, et al. Distinct time trends in colorectal cancer incidence in countries with SDI levels from 1990 to 2019: an age–period–cohort analysis for the Global Burden of Disease 2019 study. Front Public Health 2024;12:1370282. [PMID: 38841678 DOI: 10.3389/fpubh.2024.1370282]
- Dou Z, Zheng H, Shi Y, Li Y, Jia J. Analysis of global prevalence, DALY and trends of inflammatory bowel disease and their correlations with sociodemographic index: data from 1990 to 2019. Autoimmun Rev 2024;23(11):103655. [PMID: 39366514 DOI: 10.1016/j.autrev.2024.103655]
- Mou Y, Du Y, Zhou L, Yue J, Hu X, et al. Gut microbiota interact with the brain through systemic chronic inflammation: implications on neuroinflammation, neurodegeneration, and aging. Front Immunol 2022;13:796288. [PMID: 35464431 DOI: 10.3389/fimmu.2022.796288]
- Maia JM, Solon IG, Soriano RN, Branco LGS. Exploring the links between pro-inflammatory diets, gut dysbiosis, serotonin, and their implications for psychiatric and neurodegenerative disorders. Brain Behav Immun Integr 2024;8:100097. [DOI: 10.1016/j.bbii.2024.100097]
- Batagianni M, Papazoglou A, Galiatsatos P, Linos D. Assessing the relationship of gut microbiota with neurological, psychiatric, and neurodegenerative disorders: a narrative review. World J Biol Psychiatry 2025;26(8):409-21. [PMID: 40673654 DOI: 10.1080/15622975.2025.2530750]
- Li C. The role of beef in human nutrition and health. Cambridge, UK: Burleigh Dodds Science Publishing; 2017.
- Lau CS, Fulgoni VL III, Van Elswyk ME, McNeill SH. Trends in beef intake in the United States: analysis of the National Health and Nutrition Examination Survey, 2001–2018. Nutrients 2023;15(11):2475. [PMID: 37299438 DOI: 10.3390/nu15112475]
- Scollan N, Hocquette JF, Nuernberg K, Dannenberger D, Richardson I, et al. Innovations in beef production systems that enhance the nutritional and health value of beef lipids and their relationship with meat quality. Meat Sci 2006;74(1):17-33. [PMID: 22062713 DOI: 10.1016/j.meatsci.2006.05.002]
- Coffee and Caffeine Genetics Consortium; Cornelis MC, Byrne EM, Esko T, Nalls MA, Ganna A, et al. Genome-wide meta-analysis identifies six novel loci associated with habitual coffee consumption. Mol Psychiatry 2015;20(5):647-56. [PMID: 25288136 DOI: 10.1038/mp.2014.107]
- Gökcen BB, Şanlier N. Coffee consumption and disease correlations. Crit Rev Food Sci Nutr 2019;59(2):336-48. [PMID: 28853910 DOI: 10.1080/10408398.2017.1369391]
- Wang HX, MacDonald SW, Dekhtyar S, Fratiglioni L. Association of lifelong exposure to cognitive reserve-enhancing factors with dementia risk: a community-based cohort study. PLoS Med 2017;14(3):e1002251. [PMID: 28291786 DOI: 10.1371/journal.pmed.1002251]
- Clouston SAP, Manganello JA, Richards M. A life course approach to health literacy: the role of gender, educational attainment and lifetime cognitive capability. Age Ageing 2017;46(3):493-9. [PMID: 27940567 DOI: 10.1093/ageing/afw229]
- Li X, Song P, Li J, Tao Y, Li G, et al. The disease burden and clinical characteristics of inflammatory bowel disease in the Chinese population: a systematic review and meta-analysis. Int J Environ Res Public Health 2017;14(3):238. [PMID: 28264519 DOI: 10.3390/ijerph14030238]
- Zhang Y, Wang L, Yang H. Varying patterns of risk factors for inflammatory bowel disease in the East and the West: insights from the global burden of disease study 2021. BMC Public Health 2025;25(1):2252. [PMID: 40604809 DOI: 10.1186/s12889-025-23099-z]
- Ji Q, Chen J, Li Y, Tao E, Zhan Y. Incidence and prevalence of Alzheimer’s disease in China: a systematic review and meta-analysis. Eur J Epidemiol 2024;39(7):701-14. [PMID: 39088069 DOI: 10.1007/s10654-024-01144-2]
- Nam KC, Jo C, Lee M. Meat products and consumption culture in the East. Meat Sci 2010;86(1):95-102. [PMID: 20510536 DOI: 10.1016/j.meatsci.2010.04.026]
- Santich BJ. Beef consumption: historical overview, recent trends and contemporary attitudes. In: Cottle D, Kahn L, editors. Beef cattle production and trade. Clayton South, VIC: CSIRO Publishing; 2014;1-16.