Trends in Gallbladder and Biliary Tract Cancer Global Burden (1990–2021): A Socioeconomic Gradient Analysis and Projections for 2040
1Shanghai Cancer Institute, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
2Second Clinical Medical College, Guangdong Medical University, Guangdong, China
3First Clinical Medical College, Guangdong Medical University, Guangdong, China
4Department of Biology, Science Faculty, Selcuk University, Konya, Turkey
5Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu, China
6Shanghai Key Laboratory of Cancer Systems Regulation and Clinical Translation, Shanghai Jiading District Central Hospital, Shanghai, China
aThese authors contributed equally to this work.
*Correspondence to: Gokhan Zengin, Department of Biology, Science Faculty, Selcuk University, 42130 Konya, Turkey, E-mail: gokhanzengin@selcuk.edu.tr; Shuai Ren, Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, No. 155 Hanzhong Road, Qinhuai District, Nanjing 210029, China, E-mail: shuairen@njucm.edu.cn; Mengyao Li, Shanghai Cancer Institute, Renji Hospital, Shanghai Jiao Tong University School of Medicine, No 1630 Dongfang Road, Pudong new area, Shanghai 200127, China, E-mail: limy@sioc.ac.cn
Received: October 5 2025; Revised: November 10 2025; Accepted: January 3 2026; Published Online: April 1 2026
Cite this paper:
Wu Y, Yang G, Zengin G et al. Trends in Gallbladder and Biliary Tract Cancer Global Burden (1990–2021): A Socioeconomic Gradient Analysis and Projections for 2040. BIO Integration 2026; 7: 1–17.
DOI: 10.15212/bioi-2025-0174. Available at: https://bio-integration.org/
Download citation 
© 2026 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Background: Gallbladder and biliary tract cancers (GBTCs) are highly lethal malignancies with a heterogeneous global burden. Most existing epidemiological studies have been regional and descriptive, and have lacked systematic analysis of worldwide spatiotemporal trends, socioeconomic associations, and future projections. Therefore, this study was aimed at comprehensively assessing global GBTCs burden from 1990 to 2021, analyzing its association with socioeconomic development, and projecting trends to 2040.
Methods: Using data from the Global Burden of Disease (GBD) 1990–2021 study, we evaluated global trends in GBTC incidence, mortality, prevalence, and disability adjusted life years (DALYs). Age standardization was applied for comparability. Analytical methods included joinpoint regression for temporal trends, correlation analysis with the Socio-demographic Index (SDI), frontier analysis to benchmark performance, and AIMA modeling to project age-standardized incidence and mortality rates to 2040.
Results: The analysis revealed a dual burden pattern characterized by global declining age-standardized mortality and DALY rates alongside rising absolute case counts attributable to population growth and aging. Age-standardized incidence rates positively correlated with SDI. Males consistently carried a higher burden than females across all metrics. Projections indicated a continuing increase in male age-standardized incidence rates through 2040, whereas female rates were predicted to remain stable.
Conclusions: The global GBTC burden is characterized by a dual challenge of decreasing severity but expanding scale, including sex and socioeconomic gradients. These findings support a need for differentiated public health strategies. High-SDI regions should target metabolic risk factors and survivorship care, whereas low- and moderate-SDI regions require enhanced efforts in early diagnosis and management of traditional risk factors. Tailored, context-specific interventions are essential for effective global cancer control.
Keywords
Burden projection, frontier analysis, GBTCs, GBD, SCI.
Introduction
In contrast to many other malignancies, GBTCs are highly aggressive malignancies with among the poorest prognoses across all oncologic entities [1]. Their deep-seated anatomical locations and absence of specific early symptoms lead to delayed diagnosis; consequently, most patients present with advanced, inoperable stages [2]. The mortality-to-incidence ratio remains persistently and alarmingly high, and 5-year survival rates rarely exceed 15% [3]. Although GBTCs are classified as rare globally, their absolute burden is substantial and shows a strikingly uneven geographical distribution, with major disease clusters in East Asia, South America, and parts of Eastern Europe [4]. The triad of lethality, diagnostic elusiveness, and focalized high incidence makes GBTCs a persistent and complex global public health challenge.
GBTC epidemiology is shaped by a dynamic range of risk factors and strongly correlates with social development stage [5]. In low-resource settings, infectious etiologies, such as chronic Opisthorchis viverrini or Clonorchis sinensis infestation, are classic predominant drivers. In contrast, in economically developed regions, metabolic disorders (including obesity, diabetes mellitus, and cholesterol gallstone disease) resulting from lifestyle changes are key risk factors [6]. This remarkable epidemiological transition underscores the intrinsic link between cancer burden and socioeconomic context, and suggests that targeting socioeconomic-related risk exposures might enhance the effectiveness of disease prevention and control. However, because the precise nature, magnitude, and temporal progression of this association remain to be adequately quantified, the pathways through which social development influences disease risk and outcomes remain unclear; moreover, this knowledge gap hinders the design of targeted prevention and control measures [7].
The epidemiological literature on GBTCs has revealed prominent deficiencies that prevent comprehensive understanding of the disease, and the promotion of practical prevention and control measures. The research scope of most studies has been confined to national or regional levels, whereas global-scale integrated analyses reflecting the global distribution patterns and overall evolutionary trends in disease burden are lacking. Moreover, existing studies have focused on the epidemiological characteristics of the disease itself, without systematically incorporating the socioeconomic dimension into the analytical framework. Consequently, the inherent link between social development and disease burden remains to be fully understood, and long-term longitudinal trend assessments are required to elucidate the dynamic changes in disease burden. The standardized analytical framework provided by the GBD Study, which integrated indicators such as incidence, mortality, and DALYs, together with the SDI, has enabled cross-population and cross-period analyses, thus providing an important tool to address the aforementioned limitations and to explore the associations between social development and GBTCs [8].
Despite the powerful utility of the GBD data, two critical and complementary analytical perspectives have been notably underexplored in GBTC research, thus resulting in core methodological and theoretical gaps in the current literature. First, the absence of frontier analyses based on the full spectrum of the SDI gradient has precluded accurate discrimination of variations in disease burden across regions with distinct development levels, as well as adequate understanding of the inequitable status quo of healthcare service performance [9]. Second, most prior studies have been restricted to descriptive assessments of past disease trends, whereas few have used predictive models to estimate future disease burden. However, such prospective analyses are essential for proactive planning of healthcare systems and rational distribution of resources. Notably, integrating in-depth evaluation of the socioeconomic gradient with long-term disease burden forecasting is critical to close theoretical knowledge gaps and increase research value.
To bridge the aforementioned theoretical and methodological gaps, we conducted a comprehensive, integrative analysis of global GBTC burden from 1990 to 2021. We aimed to systematically delineate the spatiotemporal evolution of age-standardized incidence, mortality, and DALYs; clarify the complex association between core disease burden indicators and the SDI through correlation analysis techniques and cutting-edge analyses; and predict age-standardized incidence and mortality rates until 2024 by using the ARIMA model [10]. By integrating socioeconomic gradient assessment with long-term predictive analysis, we provide a stratified and prospective evidence base to serve as a reference for public health interventions targeting GBTCs across global regions with diverse development backgrounds.
Methods
Data source and preprocessing
The core data analyzed in this study were obtained from the GBD 2021 database via the Global Health Data Exchange (GHDx, URL: https://vizhub.healthdata.org/gbd-results?params=gbd-api-2021-permalink/f77bf15b97f0bbdf030d43275d053f23). Key GBTC indicators from 1990 to 2021 were extracted from 232 countries and territories worldwide. These indicators, including incidence, mortality, and DALYs, were obtained in three numerical formats: absolute numbers, percentages, and age-standardized rates. To assess the influence of demographic factors, we acquired the data in three distinct stratified forms: all-age combined data for males and females; sex-specific data; and data grouped into 5-year age brackets ranging from 0–4 years to 95 years and above.
The SDI served as the core socioeconomic dimension indicator, and was calculated as the geometric mean of the total fertility rate among women <25 years of age, per capita income, and the average educational attainment of individuals ≥15 years of age (ranging from 0 to 1, with higher values indicating superior socioeconomic development, educational accessibility, and demographic structure). The SDI was used to link disease burden data for gradient analysis. Two correlation strategies were used. First, in annual matching, each country’s annual SDI was paired one-to-one with its corresponding disease data for the same period. Second, in stratification grouping, countries were divided into five tiers (high, high-moderate, moderate, low-moderate, or low) by SDI, to enable dual assessment of temporal trends and developmental gradients. The standard GBD classification was used for the geographical dimension, and the analysis focused on 232 countries and territories. All data were merged, cleaned, summarized, and visualized in R 4.4.2 software (primarily with packages including ggplot2, tidyr, dplyr, broom, reshape2, scales, RColorBrewer, circlize, ComplexHeatmap, stringr, ggmap, maps, ggrepel, forecast, and ggpubr), to provide a foundation for subsequent analyses.
Explanation of data limitations
The GBD data used in this study have both aggregated ecological data and summary data characteristics, and encompass only collective information at national or regional levels, without individual-level data on risk factor exposure (e.g., obesity or history of gallstones). Because this inherent attribute precluded individual-level multivariate adjustment analyses, this study focused only on macro-trend correlations at the population level. Moreover, both aggregated ecological data and summarized data are susceptible to the ecological fallacy, in which associations observed at the group level might not apply to individuals, and details regarding individual differences can be lost during the summarization process, thus further limiting the exploration of individual risk mechanisms. These limitations were integrated into the analysis design: individual risk factors were not included in the model, and all conclusions are based on trend inferences at the population level.
Core analytical methods
We integrated correlation analysis and time series modeling, and conducted analyses through a progressive trend quantification–correlation analysis–performance evaluation–future prediction framework. All statistical processes were performed in R 4.4.2 software. Importantly, the analytical methods were applied to pre-existing datasets, and no primary data collection was conducted. These methods are described in the following sections in the same order presented in the results.
Age standardization and trend quantification of GBTC disease burden
To eliminate interference due to differences in age structure among populations in the disease burden comparisons, we used the direct method for age standardization (age-standardized rates, ASR) of incidence, mortality, and DALYs. Calculations were based on GBD 2021 standard population weights to ensure cross-country and cross-temporal comparability, in line with the general methodological guidelines for age standardization in cancer epidemiology [11]. These weights were applied to calculate age-specific rate estimates by 5-year age category (for example, from 0–4 years, 5–9 years, and so forth, to 95 years or older). This method helped minimize potential bias arising from differences in age distribution.
For trend quantification, we used three complementary methods, which were selected to meet the need for a comprehensive assessment covering short-term fluctuations, long-term trends, and overall cumulative changes. First, joinpoint regression was used to identify inflection points in the temporal ASR trends. On the basis of a log-linear model (adapted to the Poisson or exponential distribution characteristics of epidemiological data) [12], the trend phases from 1990 to 2021 were divided with a grid search algorithm. Inflection points were determined through 4500 Monte Carlo permutation tests. The annual percentage change (APC) for each phase was calculated to reflect short-term fluctuations, whereas the average annual percentage change (AAPC) was used to summarize the overall trend across the entire study period [13]. Second, the estimated annual percentage change (EAPC) was calculated to summarize the average annual trend. A linear regression model was constructed with the natural logarithm of the ASR (y = ln[ASR]) as the dependent variable and calendar year (x) as the independent variable (y = α + βx + ε, where α is the intercept, β is the slope, and ε is the error term) [14]. Subsequently, EAPC was calculated as EAPC = (eβ−1) × 100%, and its 95% confidence interval was calculated from the regression model. If the EAPC was not statistically significant or fell within the GBD uncertainty interval, the trend was deemed stable; otherwise, it was considered unstable. Third, the percentage change (PC) was calculated to intuitively reflect the overall change magnitude over the entire study period. The PC from 1990 to 2021 was computed as (ASR2021−ASR1990)/ASR1990 × 100%.
DALY estimation was performed in accordance with the method established in the GBD study, by combining years of life lost as a result of premature death and years lived with disability [15]. Years of life lost were computed with GBTC-specific mortality rates and reference life expectancies, whereas years lived with disability were calculated by integration of disability weights and the duration of illness to measure non-fatal health losses [8]. These two indicators together enabled comprehensive assessment of GBTCs.
Correlation analysis methods
Pearson correlation analysis was conducted to assess the linear association between socioeconomic development and GBTC burden, with a model design aimed at clarifying the pathway through which macro socioeconomic factors affect population-level disease burden [16]. The independent variables included the SDI, comprehensively reflecting developmental levels, and the 2021 Human Development Index, indicating healthcare quality [17]. The dependent variables included the 1990 baseline ASRs (representing the baseline disease burden); the EAPC of incidence, mortality, and DALYs (quantifying trend magnitude); and the age-standardized incidence rate (ASIR, characterizing disease risk). The analysis was conducted in two steps: (1) visualizing bivariate associations through scatter plots and (2) calculating the Pearson correlation coefficient (r) and evaluating statistical significance with a two-tailed test (α = 0.05).
Frontier analysis methods
We used frontier analysis to construct a benchmark framework for assessing the performance of GBTC disease burden control, thus enabling comparisons between regions and top-performing counterparts with comparable socioeconomic characteristics [18]. This method was aimed at identifying gaps in disease burden management and screening regions that have effectively implemented optimal control strategies. Scatter plots were constructed with the SDI on the x-axis and the age-standardized DALY rate (DALY ASR, reflecting disease burden) on the y-axis. A color gradient was used to represent the temporal changes from 1990 to 2021. Frontier regions (benchmarks for optimal performance) were defined as those with the lowest DALY ASR at a given SDI level in a specific year. Through comparison against this benchmark, we determined whether the disease burden in other regions was higher than expected according to their developmental level, thereby identifying areas requiring enhanced interventions.
Future trend prediction (ARIMA model)
The ARIMA model was used to predict age-standardized rates of GBTC incidence and mortality from 2022 to 2040. The model was selected according to the need for stationarity of time series data and the goal of accurate trend prediction. ARIMA can address data temporal dependence through autoregressive (p), differencing (d), and moving average (q) components, and its effectiveness has been verified in similar disease burden prediction studies [19].
The model assumptions and parameter optimization process were as follows. First, the premise assumption was that the macro trends from 1990 to 2021 (e.g., the association pattern between socioeconomic development and disease burden) remained relatively stable during the prediction period, without interference from sudden major public health events (such as large-scale infectious diseases or disruptive medical technologies). Second, parameters were identified by minimizing the Akaike Information Criterion (where L is the maximum value of the likelihood function, and K is the total number of estimated parameters); subsequent visual inspection and the augmented Dickey-Fuller test confirmed that the original GBTC data series was non-stationary. Therefore, first-order differencing (d = 1) was applied to achieve data stationarity. The tailing phenomenon of the autocorrelation function indicated a moving average order (q) of 0–1, whereas the truncation of the partial autocorrelation function at lags 1–2 suggested an autoregressive order (p) of 1–2. The optimal parameters were determined by minimization of the Akaike Information Criterion (balancing model fit and complexity [20]) as follows: (2,1,1) for male ASIR, (1,1,0) for female ASIR, (1,1,1) for male age-standardized mortality rate (ASMR), and (2,1,0) for female ASMR. Finally, model validation was performed with residual diagnostics (Ljung-Box Q test), which confirmed that the residuals exhibited white noise characteristics. The model output included predicted values of age-standardized incidence and mortality rates from 2022 to 2040, along with their 95% confidence intervals (reflecting prediction uncertainty). The findings might provide a reference for future trends in GBTC disease burden and inform the formulation of long-term prevention strategies.
Results
Quantitative assessment of key metrics for GBTCs
The quantitative analysis results of four core disease burden indicators (mortality, DALYs, prevalence, and incidence) of the global burden of GBTCs from 1990 to 2021 are summarized in Table 1. The core trend characteristics and in-depth implications are described below.
Table 1 Mortality, DALYs, Prevalence, and Incidence of GBTCs by Sex, 1990–2021: Counts, Percentage Change (PC), and Average Annual Percentage Change (AAPC) with Uncertainty Intervals (UI)
| Sex | Value, 1990 | Value, 2021 | PC | AAPC UI |
|---|---|---|---|---|
| Male | 8081 (5345, 11612) | 19525 (11615, 27421) | 141.60 | 2.99 (2.89, 3.09) |
| Female | 9170 (6355, 12939) | 18309 (11423, 24764) | 99.70 | 2.16 (2.05, 2.26) |
| Both | 17251 (13213, 22143) | 37833 (26653, 49262) | 119.30 | 2.57 (2.49, 2.66) |
| Male | 221390 (145097, 311194) | 459793 (269773, 651240) | 107.70 | 2.52 (2.41, 2.63) |
| Female | 230959 (158402, 322844) | 397711 (248642, 540089) | 72.20 | 1.70 (1.60, 1.79) |
| Both | 452349 (341842, 581398) | 857504 (601927, 1121113) | 89.60 | 2.12 (2.03, 2.21) |
| Male | 8792 (5766, 12289) | 44801 (25705, 62876) | 409.60 | 5.83 (5.55, 6.10) |
| Female | 9188 (6276, 12800) | 34887 (21146, 47646) | 279.70 | 4.57 (4.35, 4.79) |
| Both | 17980 (13589, 22713) | 79688 (53151, 103929) | 343.20 | 5.23 (4.99, 5.48) |
| Male | 8138 (5378, 11476) | 27797 (16110, 38966) | 241.60 | 4.28 (4.12, 4.44) |
| Female | 8940 (6147, 12548) | 23923 (14698, 32562) | 167.60 | 3.24 (3.10, 3.38) |
| Both | 17077 (13003, 21744) | 51720 (35618, 66848) | 202.90 | 3.77 (3.63, 3.92) |
Over the past 30 years, GBTCs exhibited a dual burden globally, characterized by diminished severity but expanded effects. This concept refers to a contradictory trend in which lethality and damage to health decreased, but the scale of affected populations continued to expand, thus challenging global GBTC prevention and control measures. Specifically, indicators reflecting disease severity improved: the mortality rates for males, females, and the total population continued to decline, and male deaths decreased by 45.20%. DALYs showed a more pronounced improvement, including a 59.10% decrease in male DALYs (AAPC = −3.33%). These findings indicated that advances in global GBTC diagnosis and treatment have effectively decreased disease-related mortality risk. However, indicators reflecting the scope of the disease’s effects showed an opposite increasing trend: the male prevalence rate surged by 84.60%, and the overall prevalence showed an average annual growth rate of 2.01%; although the incidence rate generally decreased (by approximately 11.70% in new male cases), its rate of decline was far lower than the growth in prevalence and therefore did not offset the expansion of disease effects.
Further decomposition of indicator patterns revealed that, among count-based indicators (reflecting the total number of affected individuals), the prevalence count showed the most significant increase (total PC = 343.20%, AAPC = 5.23%) and was followed by the incidence count (PC = 202.90%, AAPC = 3.77%). Among rate-based indicators (reflecting population risk levels), the age-standardized prevalence rate increased by 89.60% (AAPC = 2.12%), and the ASIR rose by 119.30% (AAPC = 2.57%). These findings indicated that because the population risk of GBTCs has continued to increase, enhanced prevention and early screening efforts are necessary.
All indicators demonstrated consistent sex differences: males showed consistently higher PC and AAPC than females across the four core indicators (e.g., the PC was 141.6% for males versus 99.7% for females, and the incidence rate increased by 241.6% in males versus 167.6% in females). Therefore, males are the primary population driving the growth of GBTC disease burden, a finding potentially associated with higher risk factor exposure rates among males than females.
In summary, the global GBTC disease burden showed an overall increasing trend from 1990 to 2021, and its core characteristics included a dual burden and male-dominated growth.
Statistical analysis of key age-standardized rates for GBTCs
The age-standardized data (Table 2) eliminated the confounding effects of population aging and growth, thus further verifying the dual burden characteristics of GBTCs and providing a complementary interpretation to the trends in absolute counts (Table 1).
Table 2 Age-Standardized Rates (per 100,000 Population), Percentage Change (PC), and Average Annual Percentage Change (AAPC) with Uncertainty Intervals (UI) for Mortality, DALYs, Prevalence, and Incidence of GBTCs by Sex, 1990–2021
| Measure | Sex | Value, 1990 | Value, 2021 | PC | AAPC UI |
|---|---|---|---|---|---|
| Deaths | Male | 2.38 (1.55, 3.5) | 2.11 (1.26, 2.92) | −11.30 | −0.34 (−0.47, −0.22) |
| Deaths | Female | 2.32 (1.6, 3.24) | 1.67 (1.04, 2.25) | −28 | −1.17 (−1.29, −1.04) |
| Deaths | Both | 2.32 (1.78, 2.97) | 1.85 (1.29, 2.4) | −20.30 | −0.75 (−0.87, −0.64) |
| DALYs | Male | 52.86 (34.73, 75.75) | 45.57 (26.8, 63.82) | −13.80 | −0.41 (−0.51, −0.31) |
| DALYs | Female | 52.85 (36.17, 73.76) | 35.83 (22.37, 48.65) | −32.20 | −1.36 (−1.47, −1.25) |
| DALYs | Both | 52.61 (39.99, 67.15) | 40.38 (28.21, 52.61) | −23.20 | −0.87 (−0.96, −0.77) |
| Prevalence | Male | 2.22 (1.45, 3.16) | 4.47 (2.58, 6.19) | 101.40 | 2.62 (2.44, 2.83) |
| Prevalence | Female | 2.16 (1.48, 3) | 3.15 (1.91, 4.3) | 45.80 | 1.35 (1.2, 1.51) |
| Prevalence | Both | 2.18 (1.66, 2.74) | 3.77 (2.51, 4.91) | 72.90 | 2.04 (1.85, 2.22) |
| Incidence | Male | 2.21 (1.46, 3.23) | 2.89 (1.69, 4) | 29 | 1 (0.88, 1.11) |
| Incidence | Female | 2.19 (1.51, 3.05) | 2.17 (1.33, 2.95) | −0.90 | −0.04 (−0.14, 0.06) |
| Incidence | Both | 2.19 (1.68, 2.79) | 2.49 (1.71, 3.21) | 13.70 | 0.5 (0.4, 0.6) |
Globally, both the age-standardized mortality rate (a 20.3% decrease) and the age-standardized DALY rate (a 23.2% decrease) showed statistically significant declines. Therefore, after adjustment for population structure, the risk of disease-induced death and the level of health damage at the population level showed improvements. In contrast, the global age-standardized prevalence rate rose substantially (72.9% overall increase), a finding further confirming that the expanding scope of disease was not due to changes in population structure and provided a true reflection of elevated population disease risk. This result reinforced our primary conclusion regarding the existence of a dual burden, i.e., that GBTC prevention and control must simultaneously address two goals of decreasing mortality risk and controlling the scale of prevalent cases.
Sex- and age-stratified distribution of GBTC burden indicators
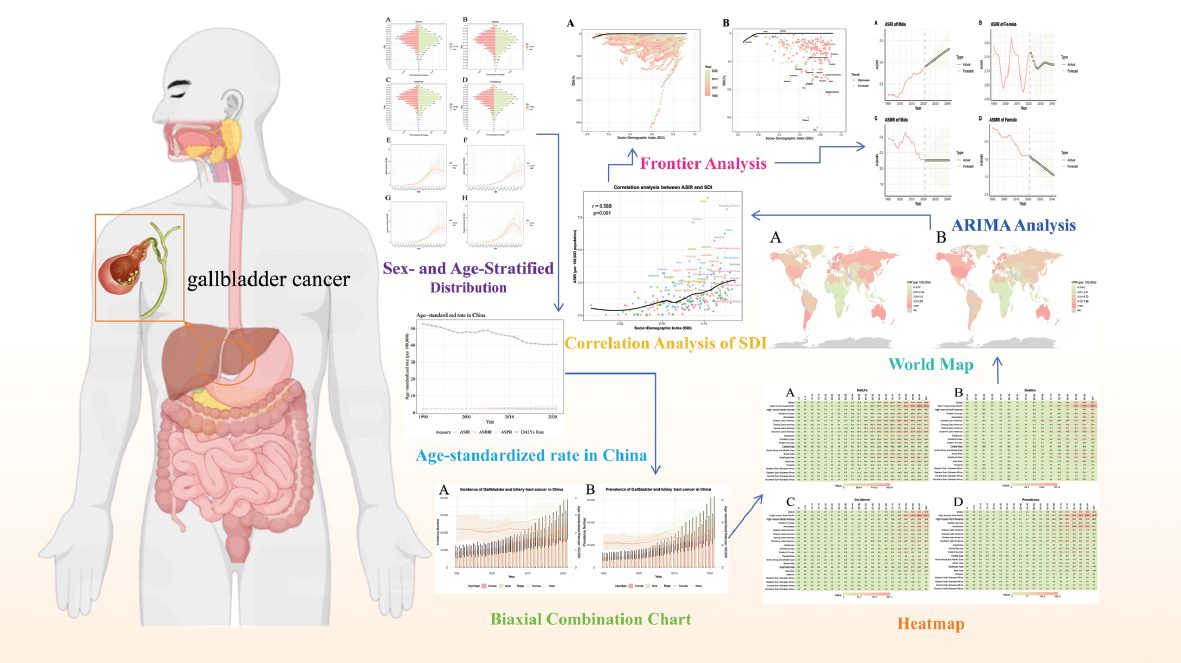
We used a unified visualization framework (a dual-panel structure with a consistent color scheme of pink indicating females and green indicating males) to systematically analyze the age and sex distribution characteristics of GBTC burden (Figure 1A–H). The core patterns are summarized as follows.
Figure 1 Comprehensive presentation of gallbladder and biliary tract cancer burden metrics: sex- and age-stratified distributions and global age-specific patterns in DALYs, mortality, incidence, and prevalence, 1990–2021.
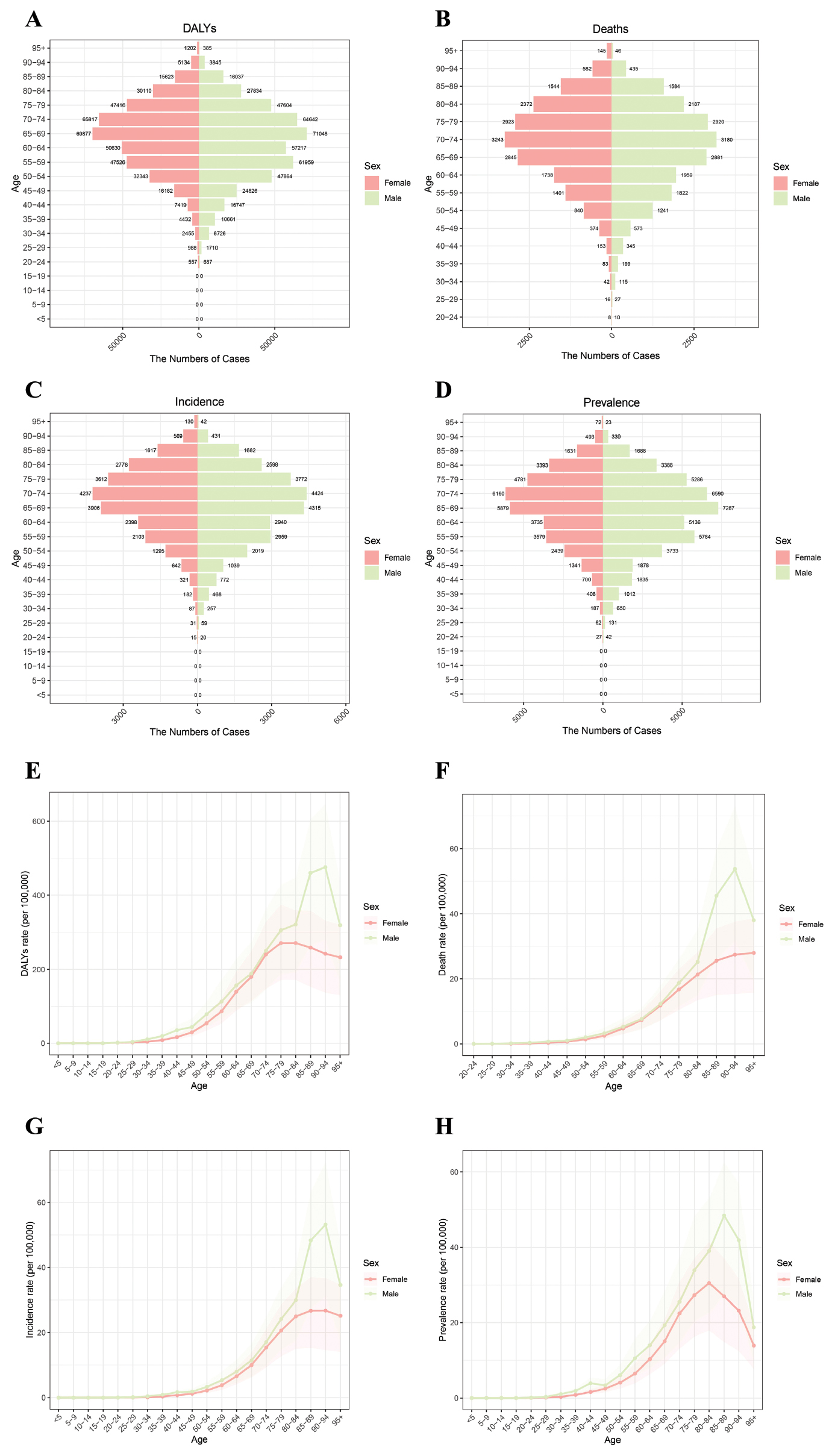
Regarding age-associated characteristics, all burden indicators (DALYs, mortality, incidence, and prevalence) showed an increasing trend with advancing age, and a marked acceleration in the growth rate was observed after middle age (≥50 years). The burden peaks for males appeared primarily between 65 and 84 years old (e.g., DALY peak at 65–69 years and mortality peak at 70–74 years), whereas the peaks for females emerged later and were milder in magnitude (e.g., mortality peak at 65–74 years). Moreover, the male peaks were significantly higher than the female peaks in the advanced age group (≥80 years).
Analysis of the characteristics of the sex difference indicated that the burden indicators (case counts and standardized rates) for males remained consistently higher than those for females across all age groups. The most prominent differences were observed in the middle-aged and older population (50–69 years). Males showed systematically higher values than females in all aspects: DALYs reflecting health loss, mortality indicating fatal risk, incidence representing disease occurrence, and prevalence measuring the scale of prevalent cases. Additionally, these sex differences widened with increasing age. This pattern was consistent with the conclusions in Section 3.1, in which males (particularly those middle-aged or older) were found to be the key population that should be targeted to decrease GBTC burden.
In summary, GBTC burden presented a stable distribution pattern characterized by age-dependent growth and persistent male predominance, thus providing precise targets for formulating stratified prevention and control strategies.
Age-standardized incidence, mortality, prevalence, and DALYs
Figure 2 presents trends in the core age-standardized indicators of GBTCs in China from 1990 to 2021. The results demonstrated remarkable effectiveness of prevention and control measures.
Figure 2 Age-standardized incidence, mortality, prevalence, and disability-adjusted life year rates of GBTCs in China, 1990–2021.
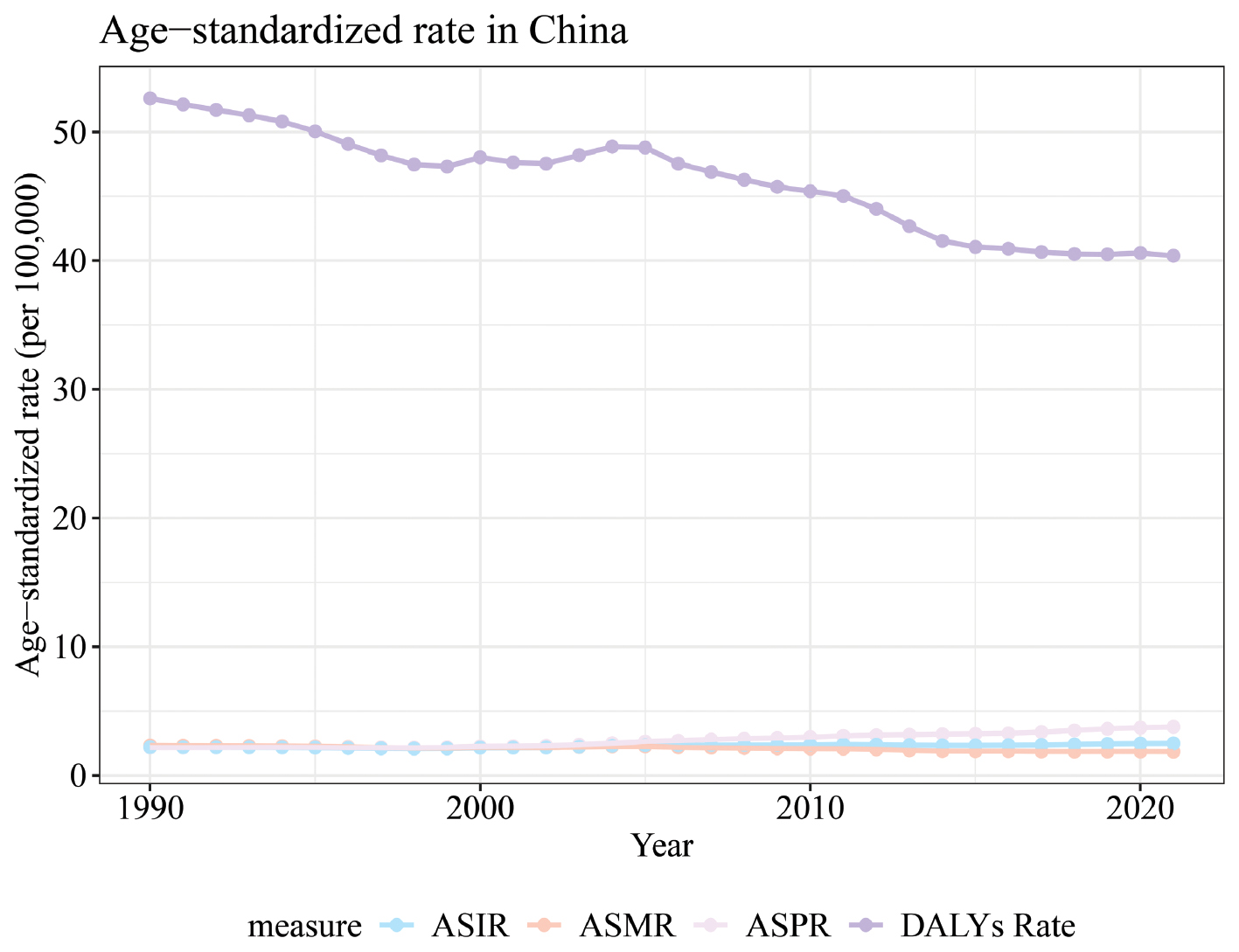
The age-standardized DALY rate (purple line) had the highest value among the four indicators but showed a consistent decrease, from approximately 5.3 million in 1990 to approximately 4.0 million in 2020, thus reflecting a substantial decline in GBTC-related health loss in China. The age-standardized incidence and mortality rates (light blue and light orange lines, respectively) remained consistently low (approximately 0.2 million), with mild fluctuations. Although the age-standardized prevalence rate (light pink line) exhibited a moderate increasing trend (reaching approximately 3.5 million in 2020), it remained generally low overall.
The above trends indicated that China’s GBTC prevention and control measures have achieved favorable outcomes characterized by decreased health loss and stabilized fatal and incidence risks, without the dual burden contradiction observed at the global level. This finding reflects the remarkable effectiveness of the management of this disease in China.
Biaxial combination chart (sex-time distribution in China)
Figure 3 uses a dual-axis combination of bar charts (case counts) and line charts (rate values) to illustrate the temporal and sex-specific distribution of GBTC incidence and prevalence in China (Figure 3A, B). The key findings are elaborated upon from the perspectives of temporal trends and sex-specific patterns as follows.
Figure 3 Incidence and age-standardized incidence rates of GBTCs in China, 1990–2021.
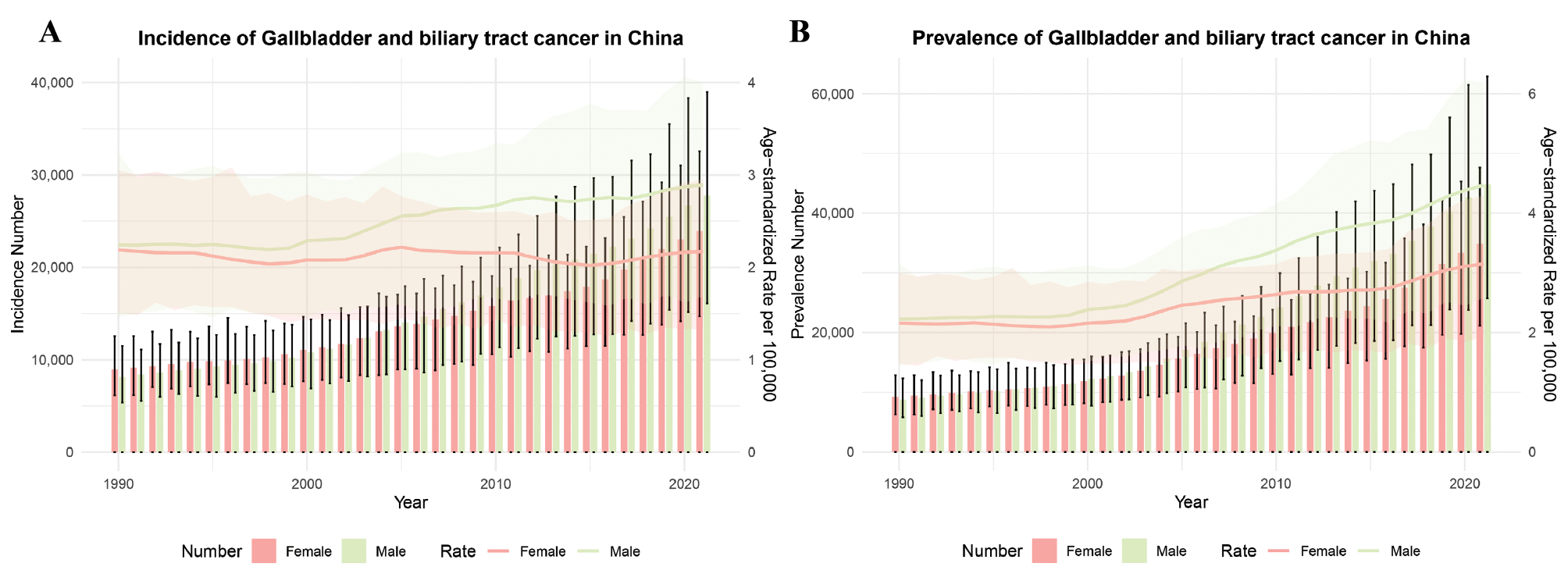
First, analysis of temporal trends indicated marked increases in incidence and prevalence over time, and the growth rate of incidence accelerated after 2010, thus demonstrating a gradually increasing disease burden of GBTCs in China.
Second, analysis of sex-specific patterns revealed systematically higher case counts, incidence rates, and prevalence rates in males than females. These differences persisted throughout the entire study period. Regarding incidence, both male case counts and rates showed a continual rise; moreover, the number of prevalent male cases increased monotonically, and the age-standardized rate remained consistently higher than that of females. This result was consistent with the global sex difference pattern, thus further confirming that males in China are the key population for GBTC prevention and control.
Heatmap analysis (global regional disparities and spatiotemporal trends)
Figure 4 illustrates the global distribution and spatiotemporal trends of disease burden associated with GBTCs across various regions from 1990 to 2021. In this figure, darker shading represents higher values. The core features are further described below, from the perspectives of regional differences and temporal trends.
Figure 4 Global heat map of GBTCs burden: case counts and incidence rates, 1990–2021.
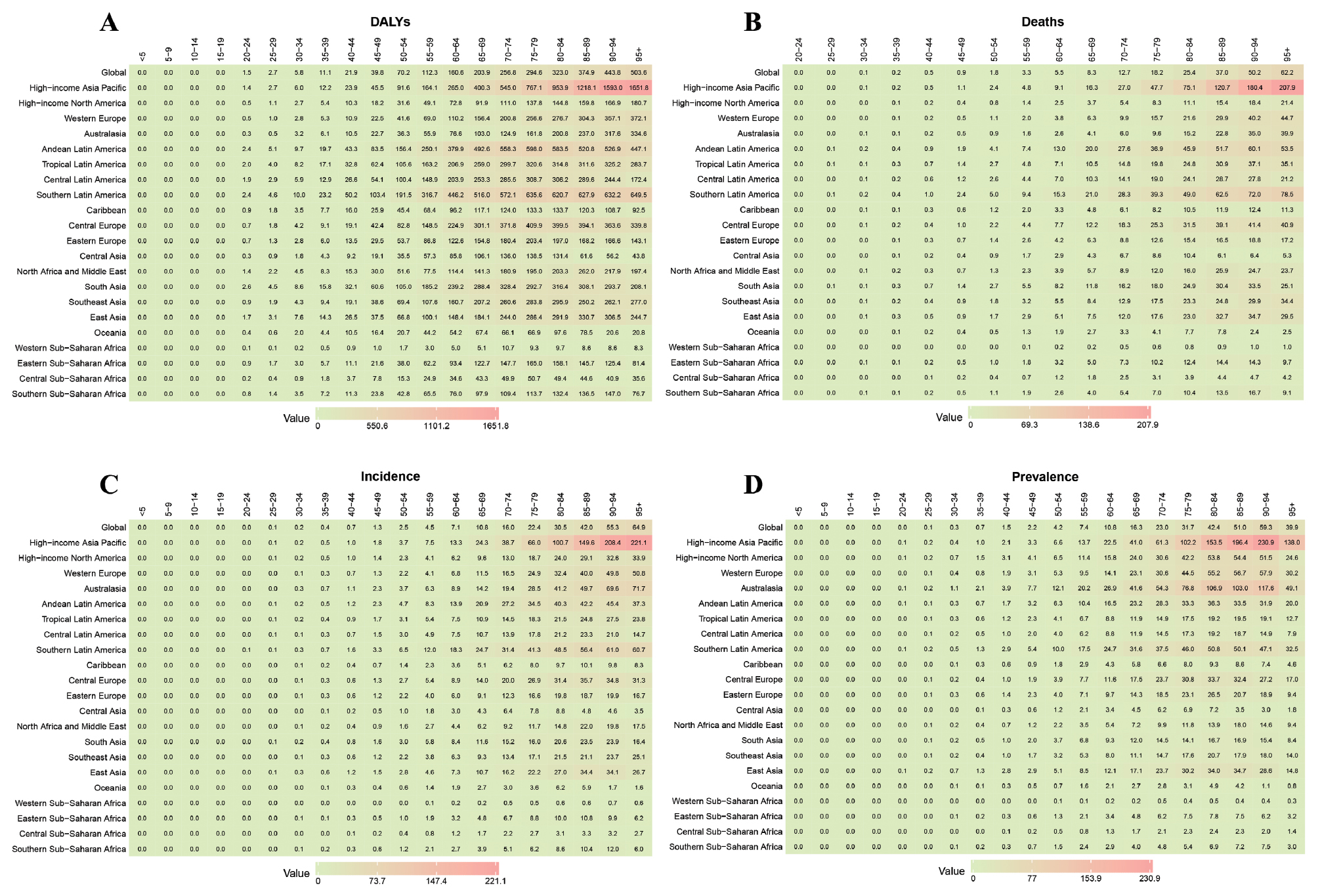
In the analysis of regional differences, the colors corresponding to the four indicators (DALYs, number of deaths, incidence, and prevalence) in regions such as East Asia and South America were significantly darker than those in regions such as high-income North America. Therefore, these areas were high-burden clusters of global GBTCs, whereas high-income North America consistently showed lighter colors reflecting a relatively low disease burden.
In the analysis of temporal trends, the colors of the global overall data, as well as those of high-burden clusters including East Asia and South America, gradually deepened over time. This finding indicated continually increasing trends in health loss, number of deaths, new cases, and prevalence scale in these regions, and suggested that the dual burden feature was relatively more prominent in high-incidence areas. In contrast, the trend in high-income North America remained relatively stable and showed no clear signs of exacerbation.
In conclusion, the GBTC disease burden in countries with low socioeconomic development levels was higher than that in countries with high socioeconomic development levels, and showed an increasing trend.
World map
Figure 5 depicts the global geographical variation in the incidence and prevalence of GBTCs according to data sourced from the GBD database. Panels A (cancer incidence rate) and B (cancer prevalence rate) show global distribution maps, in which the shading intensity is proportional to rates per 100,000 population, and darker shades represent higher values.
Figure 5 Global distribution of cancer incidence rates (CIR) and cancer prevalence rates (CPR).
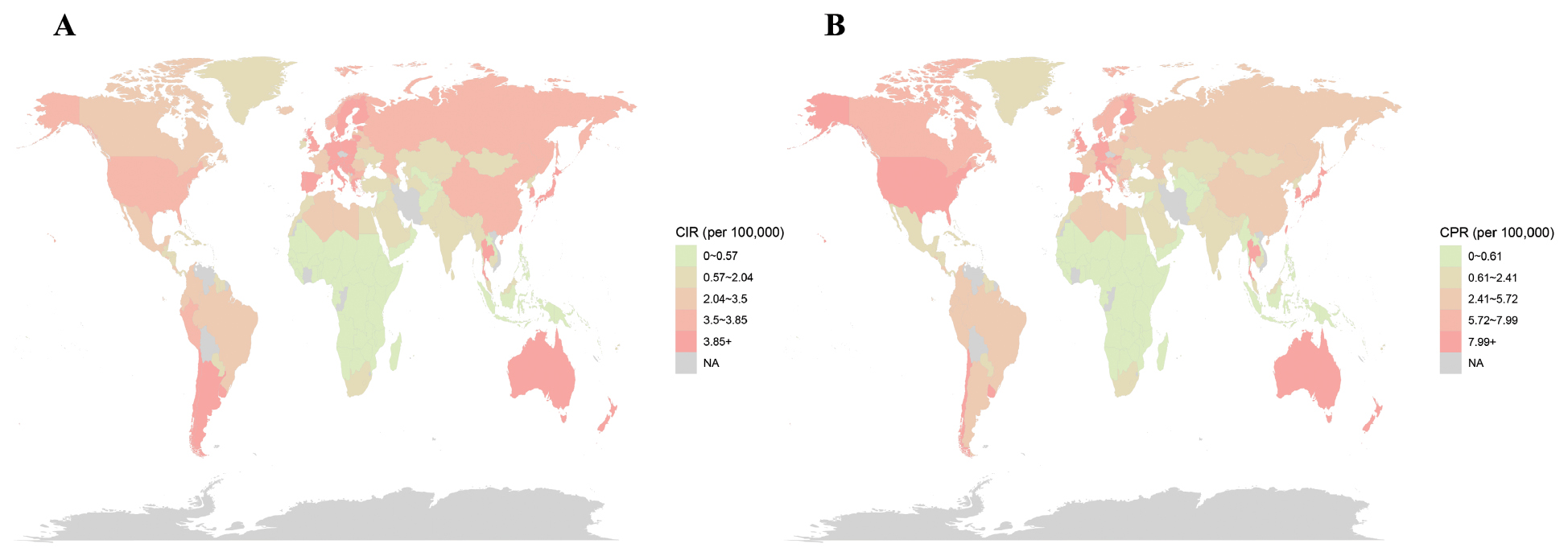
The incidence distribution (Figure 5A) indicated significant geographical variation in GBTC incidence rates worldwide. Areas in East Asia, Europe, and parts of South America were darker in color, thus suggesting relatively elevated risk of new cases. In contrast, the central-southern part of Africa and parts of the Middle East were relatively lighter in color.
The prevalence distribution (Figure 5B) showed several similarities to the incidence pattern in terms of spatial concentration, as well as clear differences in value ranges. The difference in shading patterns, for example in Australia and North America, was likely to have represented regional differences in patient survival times and case accumulation, because prevalence is a joint effect of both disease incidence and survival time.
SDI correlation analysis
Figure 6 analyzes the relationship between the ASIR of GBTCs and the SDI across 204 countries and territories from 1990 to 2021. The key findings were as follows.
Figure 6 Correlation analysis between SDI and age-standardized incidence rates (ASIR, new cases per 100,000 population) of GBTCs worldwide, 1990–2021. Inflection points in the male ASIR trend (around 2010) and regions deviating from the SDI frontier (e.g., Niger with increasing DALYs and South Sudan with decreasing DALYs in low-SDI countries) are highlighted to facilitate interpretation.
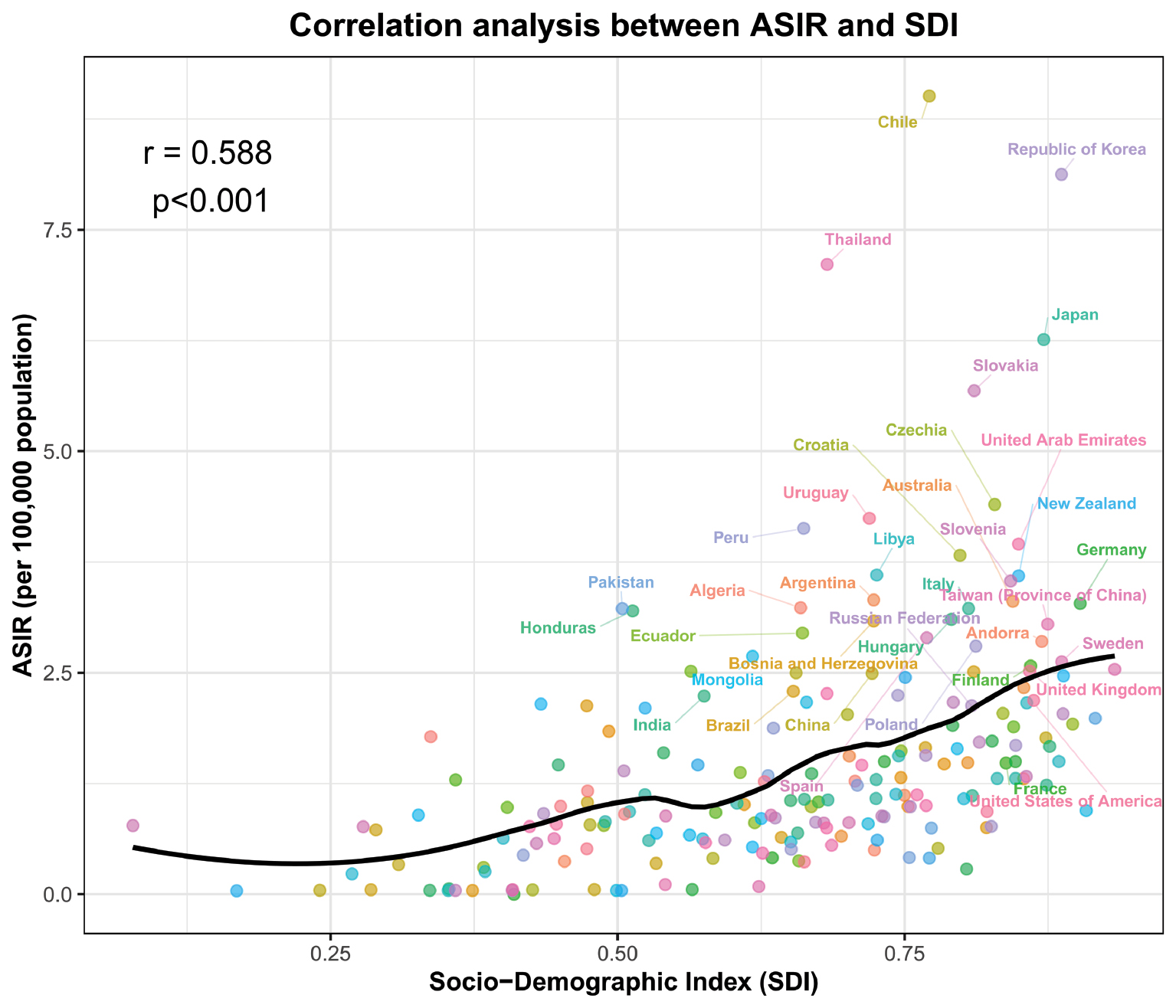
The findings indicated a statistically positive correlation between SDI and GBTCs ASIR (correlation coefficient r = 0.588, P < 0.001). Therefore, regions with higher socioeconomic development, educational attainment, and life expectancy had higher GBTC incidence rates. The scatter plot distribution demonstrated that regions with high SDI, such as Chile, South Korea, and Japan, generally displayed relatively elevated ASIR values, whereas most low-SDI regions showed lower ASIR rates. The overlaid curve visually validated this positive correlation and highlighted a trend in which the incidence rate of GBTCs rose with increasing sociodemographic development.
Frontier analysis
Figure 7 shows a frontier analysis using the global surveillance function of the GBD database, with the minimum DALYs recorded at each SDI level serving as the performance benchmark, to illustrate the spatiotemporal correlation between DALYs of GBTCs and the SDI from 1990 to 2021.
Figure 7 Spatiotemporal correlation between GBTC DALYs and SDI (1990–2021). (A) Global distribution (left: red = 1990; green = 2020) and temporal trends by SDI tier (right, black frontier curve indicates minimum achievable DALY level). (B) Heterogeneity in national trends (green: increasing; red: decreasing), with fitted curve showing SDI-DALY association.
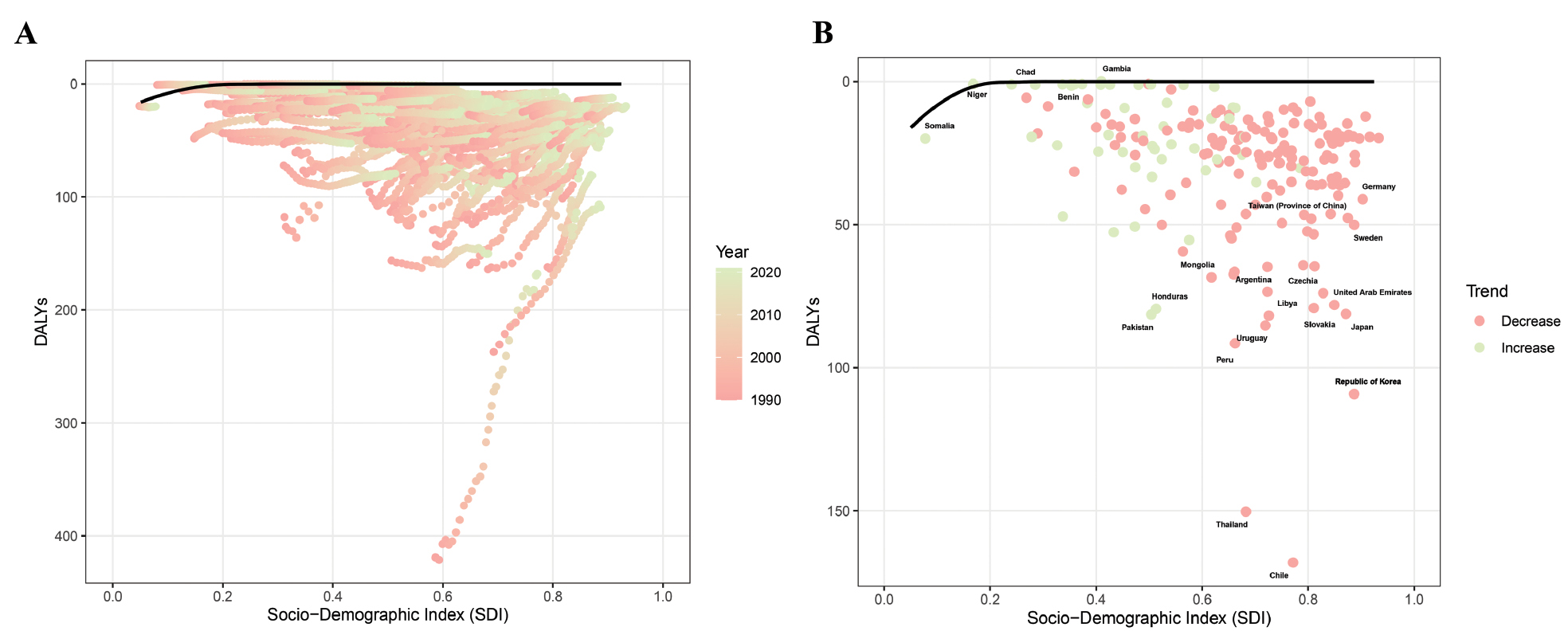
Figure 7A presents two subpanels: the global distribution of GBTCs DALYs by SDI from 1990 to 2021 (color-coded by year, with red representing 1990 and green representing 2020), and the temporal changes in DALY trends across regions, stratified by SDI. Low-SDI regions had high DALY values (red color in the 1990s) and showed varied temporal trends, whereas high-SDI regions generally maintained low DALYs over time. The frontier line, the black line representing the minimum achievable DALY level at each SDI level, revealed that, with increasing SDI, the growth trajectory of the DALY frontier gradually decelerated and eventually stabilized or even showed signs of improvement in high-SDI regions.
Figure 7B further displays the heterogeneity in the trends within these regions, with green and red dots representing increasing and decreasing trends, respectively. Some low-SDI countries (e.g., Niger) showed increasing trends in DALYs over time, whereas other low-SDI countries (e.g., South Sudan and Afghanistan) showed declining trends. Similarly, in high-SDI countries, heterogeneous trends in DALYs were observed over time.
These results indicated that socioeconomic development, accompanied by improved healthcare accessibility and refined disease control systems, helps curb the growth of DALYs but cannot fully offset disease burden; consequently, high-SDI regions still must optimize prevention and control strategies to maintain low DALY levels, whereas low-SDI regions must take targeted measures to address the burden differences caused by unbalanced development.
ARIMA analysis
Figure 8A–D illustrates the trends and predicted results of ASIR and ASMR of global GBTCs from 1990 to 2040, on the basis of the ARIMA model. The core sex-specific predictions are detailed below.
Figure 8 ARIMA of age-standardized incidence and mortality rates for GBTCs in males and females worldwide, 1990–2040.
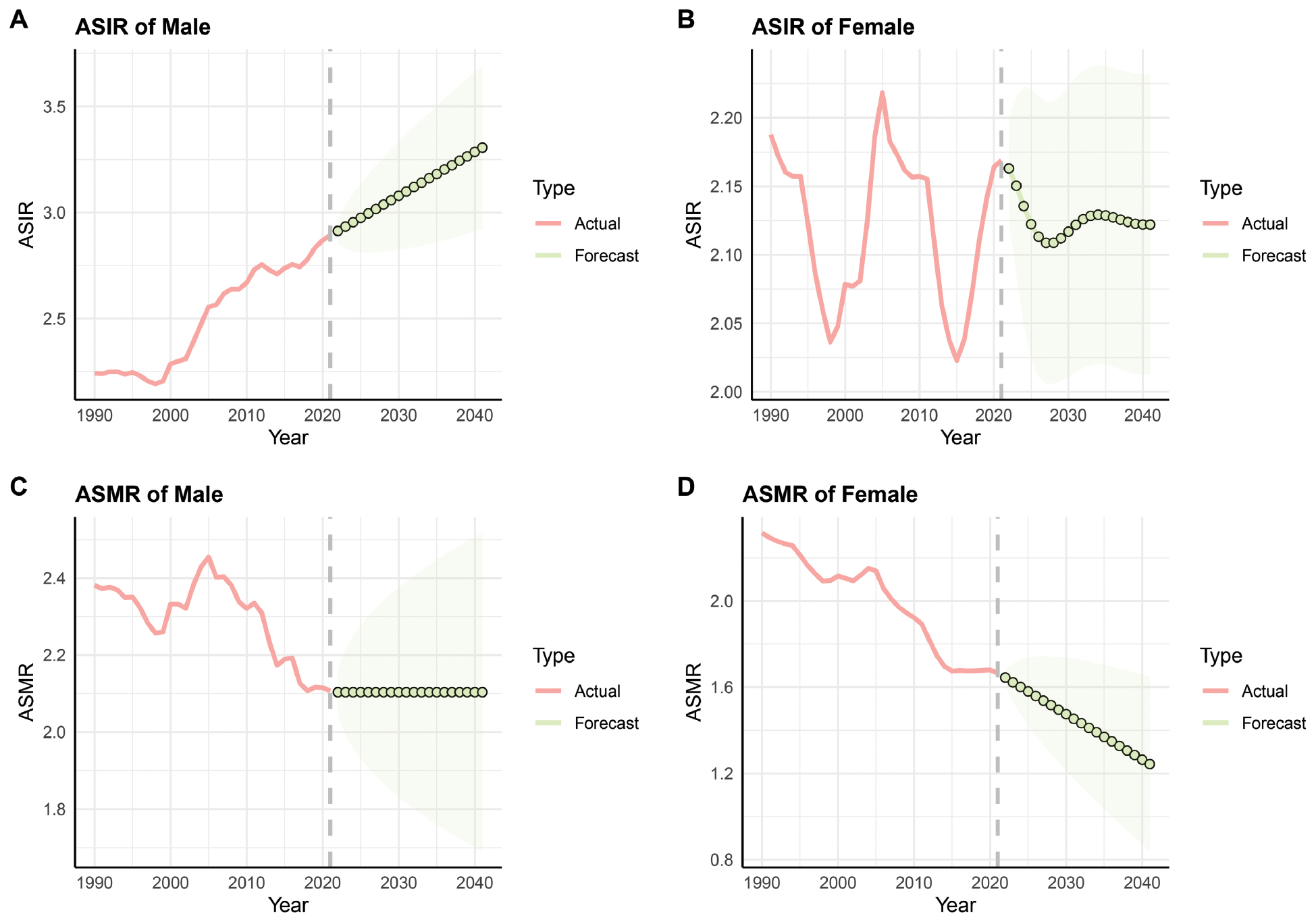
Among males, the actual ASIR showed a continually increasing trend from 1990 to 2020 and was predicted to grow steadily after 2020. The actual ASMR stabilized after fluctuations and showed an overall decreasing trend, and is expected to remain stable after 2020.
Among females, the actual ASIR from 1990 to 2020 fluctuated but showed an overall decreasing trend. Predictions indicated relative stability after 2020. The actual ASMR exhibited a significant decreasing trend and was projected to decline further beyond 2020.
In summary, the global GBTC burden is expected to present a sex-specific pattern characterized by rising incidence in males and continuing improvement in female mortality in the future. The sustained increase in male ASIR may exacerbate the global disease burden, whereas the steady decline in female mortality reflects the potential effectiveness of targeted prevention and control strategies, thus providing a clear direction for the priority allocation of prevention and control resources in the future.
Discussion
Core findings
The global epidemiology of GBTCs revealed a complex interplay among socioeconomic development, demographic transitions, and healthcare advancements extending far beyond simple descriptive statistics. Our analysis uncovered three fundamental mechanisms driving the observed patterns: a paradoxical relationship between economic development and cancer risk, potential inequalities reflected by the performance frontier of disease control, and predicted trends in future shifts in disease burden. Together, these mechanisms explain why GBTCs pose a unique challenge in global cancer control and provide a new perspective for re-examining the relationship between development and disease burden.
The most important discovery in this study was that the global disease burden of GBTCs showed a dual burden pattern. First, the data clearly indicated significant decreasing trends in both age-standardized mortality and DALYs rates, while the absolute values such as the number of deaths, DALYs, new cases, and prevalent cases all increased substantially. Notably, the age-standardized prevalence rate surged by 72.9%, whereas the age-standardized incidence rate showed a relatively modest increase of 13.7%. Reasonable inferences drawn from the data indicated that the decline in age-standardized mortality and DALY rates reflected a genuine decrease in population-level risks of death and health loss after controlling for demographic factors; the difference between the growth of age-standardized prevalence and incidence rates suggested that increased survival rates were the primary reason for the increase in patients with prevalent disease. We speculate that the decrease in mortality risk might have been associated with advancements in diagnostic technologies and improvements in surgical and systemic therapies in the past three decades, and the increase in absolute disease burden might have stemmed from global population growth, population aging, and prolonged survival time after diagnosis. That is, medical progress, combined with demographic changes, might have led to many survivors and ultimately to a continual rise in the total disease burden borne by society.
Our findings also indicated striking heterogeneity in GBTC burden by sex and geographical distribution. Males had systematically higher values than females for all absolute and age-standardized disease burden indicators. Moreover, the male ASIR increased over time, whereas the female rates were more stable or decreased. The geographical distribution showed a positive correlation between GBTC burden and SDI: higher age-standardized GBTC incidence rates were observed in high-SDI countries, a finding in sharp contrast to those for diseases such as cervical cancer or certain infectious diseases, which are more prevalent in low-SDI regions. Although this positive correlation between SDI and incidence rate is intriguing, it can be interpreted through biological and health system mechanisms supported by the previous literature. This phenomenon is consistent with the general pattern of modern cancer control summarized in the review Cancer Treatment: Past, Present, and Future [21], which has noted that contemporary cancer control measures often result in concurrent rising incidence rates and declining mortality rates. The increased incidence in high-SDI regions was attributed primarily to enhanced diagnostic capabilities and lifestyle transitions, whereas the decrease in DALYs reflected advancements in innovative treatment protocols and comprehensive cancer care systems. This finding was further corroborated by the observations in the study Global, Regional, and National Burden of Gallbladder Cancer, 1990–2019: socioeconomic development drives a shift in risk factor profiles, wherein dietary fat intake and gallstone prevalence, both of which are key risk factors for GBTCs, increase with rising SDI, while traditional infectious risks (e.g., Clonorchis sinensis infection) decline with improved sanitation. This transition explains why high-SDI regions such as East Asia and high-income Europe have maintained high incidence rates despite decreased parasitic exposure. In addition, the study Socioeconomic Disparities in Hepatobiliary Cancers: A Global Epidemiologic Perspective has indicated that advanced diagnostic infrastructure in high-SDI countries improves the detection of early-stage GBTCs and might potentially lead to higher estimated incidence rates than those for low-SDI regions, where underdiagnosis remains prevalent. Reasonable inferences regarding the causes of the sex differences can be made according to existing evidence: these differences might be associated with differences in gallstone prevalence, metabolic differences, and exposure to behavioral risk factors (e.g., smoking and alcohol consumption) between males and females. These sex-specific differences might also reflect differences in access to healthcare and screening, as well as biological mechanisms such as estrogen-mediated bile duct protection, all of which warrant further research to inform the development of sex-tailored intervention strategies [22].
The positive correlation between SDI and GBTC incidence rate requires particularly cautious interpretation. This association is merely an ecological correlation directly presented by the data but cannot be directly inferred as a causal relationship. Multiple reasons might explain the phenomena and fit the existing data. First, under the detection effect, advanced diagnostic infrastructures in high-SDI countries might increase the detection rate of early-stage GBTCs, whereas widespread underdiagnosis in low-SDI regions might lead to overestimated incidence rates. Second, differences in coding standards, including variations in diagnostic coding criteria for GBTCs across regions with different SDI levels, might affect the statistical results of incidence rates. Third, according to survival bias, longer survival times among patients in high-SDI regions might indirectly influence the statistical classification of disease burden indicators. On the basis of the previous literature, this correlation might reasonably be speculated to be associated with the shift in risk factors driven by socioeconomic development; i.e., a westernized lifestyle in high-SDI regions might lead to a high prevalence of obesity and metabolic syndrome (key risk factors for GBTCs), whereas traditional infectious risks (e.g., Clonorchis sinensis infection) might persist in low-SDI regions. However, this speculation requires verification on the basis of individual-level data, and the effects of the above alternative explanations cannot currently be ruled out.
SDI gradient, frontier gap, and 2040 trajectory: a practical perspective on GBTC prevention and control
Transition in risk factors along the SDI gradient
The positive correlation between SDI and GBTC incidence underscores the complex association between socioeconomic development and risk factor exposure. On the basis of existing evidence, risk profiles in high-SDI countries might reasonably be inferred to be dominated by lifestyle-related risks such as obesity and metabolic syndrome, whereas low-SDI regions might remain affected primarily by traditional infectious risks such as liver fluke infection. However, this gradient of differences describes only correlations at the population level and cannot be directly generalized to the individual level. Individuals with different socioeconomic statuses within the same country can exhibit heterogeneous GBTC risks, and the association between SDI and incidence rate might be confounded by factors such as detection effects and coding discrepancies. Future research should include individual-level cohort studies to further clarify the causal pathway between SDI and GBTC risk.
Guiding value of frontier analysis for interventions in lagging regions
Frontier analysis revealed that the DALY frontier in low- and moderate-SDI regions has declined slowly. We therefore infer that these regions are lagging in translating the achievements of socioeconomic development into GBTC control effectiveness, possibly because of inadequate healthcare infrastructure, limited prevention programs, and persistent exposure to modifiable risk factors. From a practical application perspective, this finding provides clear targets for formulating intervention priorities: for lagging regions such as sub-Saharan Africa and Central Asia, priority should be given to supplementing basic medical resources (e.g., increasing the accessibility of ultrasound diagnosis) and preventing traditional infectious risks (e.g., liver fluke deworming programs), rather than directly copying the screening models of high-SDI regions. These efforts would ensure the compatibility of intervention measures with the local development level.
Implications of 2040 projections for prevention priorities
Predictions from the ARIMA model suggested that the male age-standardized incidence rate will continue to rise after 2020, whereas the female incidence rate is expected to remain relatively stable, and the mortality rate is expected to continue to decline. From a practical application perspective, policymakers and clinicians could use these prediction results in three aspects. First, in priority planning for resource allocation, resource investment in screening for high-risk factors of GBTCs (such as gallstones and obesity) should be strengthened and should target males, particularly in middle age, and incorporate male-specific prevention into regional cancer prevention and control programs. Second, for dynamic monitoring and adjustment, with the predicted trends serving as a benchmark, prevention and control strategies should be updated every 3–5 years in combination with actual incidence data to ensure timely correction of deviations. Third, a stratified intervention design should be adopted, focusing on preventing and controlling metabolism-related risk factors to slow the rise in male incidence rates in high-SDI regions, and on improving basic diagnosis and treatment capabilities to decrease female mortality rates in low-SDI regions. For females, the effectiveness of existing intervention measures requires further verification, and early detection and treatment protocols should be continually optimized in clinical practice to demonstrate a consistent downward trend in mortality rates.
Importantly, we caution that this prediction was based on historical trends from 1990 to 2021 and has clear limitations. This study did not include potential future intervention measures, such as widespread implementation of ultrasound screening in low-SDI regions, strengthened prevention and control of metabolic risk factors in high-SDI regions, and vaccination in liver fluke-endemic areas. In addition, it did not consider uncertain factors such as sudden public health events and disruptive medical technologies. Therefore, our predictions serve only as a baseline scenario reference rather than a deterministic result, and cannot directly provide an absolute basis for policy planning.
Theoretical and practical significance
Our findings provide a targeted direction for public health policy design, by clarifying that the control strategy for GBTCs should shift from solely focusing on decreasing mortality to comprehensive whole-chain management including prevention, diagnosis, treatment, and rehabilitation [23], with full consideration of the actual medical resource conditions in different regions. At the level of etiological prevention, differentiated measures must be formulated according to the risk characteristics of regions with varying SDI levels. High-SDI regions should prioritize the prevention and control of lifestyle-related risks, such as obesity and metabolic syndrome, and should promote weight management and healthful diet interventions through public health education and community health management initiatives [24–26]. Low-SDI regions, in contrast, should prioritize controlling traditional risks such as Clonorchis sinensis infection, strengthening the construction of sanitation facilities, and implementing targeted deworming programs. Special attention should be paid to the limitations of early detection: although advanced endoscopic equipment (e.g., choledochoscopes) used in high-SDI regions can improve the detection rate, they are expensive and difficult to popularize in low-SDI regions. Therefore, a low-cost detection method that can also ensure high detection efficiency must be developed.
Regarding survivor management, as the numbers of GBTC survivors increase, health systems should plan to build comprehensive systems for long-term follow-up, rehabilitation, and supportive care for chronic cancer management. The development of these systems must be aligned with regional medical system capacity: high-SDI regions might leverage existing cancer centers to build standardized follow-up networks incorporating services such as nutritional support and psychological intervention; in contrast, low-SDI regions might integrate primary healthcare resources and use a centralized diagnosis and treatment plus primary care follow-up model to decrease management costs. For low- and moderate-SDI countries, although socioeconomic development should be promoted, early diagnostic capacity for GBTCs should be expanded, so that surveillance and control outcomes can be improved to decrease the gap with high-SDI countries. The feasibility of expanding early diagnosis in low-SDI countries must be contextualized according to current healthcare resource capacity. Most low-SDI regions face constraints including limited access to endoscopic equipment (e.g., the choledochoscopes essential for biliary tract lesion detection), insufficient pathological testing infrastructure (e.g., a lack of specialized laboratories for GBTC histopathological confirmation), and financial barriers to screening programs, particularly for high-risk populations that might not be able to afford the out-of-pocket costs of diagnostic procedures. These resource gaps highlight the need for tailored, resource-appropriate strategies rather than direct use of high-SDI countries’ screening models. To address this aspect, we propose context-specific early detection strategies for low-SDI countries, First, high-risk populations should be defined according to locally prevalent risk factors, including individuals with a history of gallstones (confirmed via abdominal ultrasound, a more accessible tool than endoscopy), chronic liver fluke infection (endemic in regions such as Southeast Asia), or a family history of GBTCs; Second, the screening frequency should be set at 2–3 years for high-risk groups, to balance detection efficacy with resource constraints. Third, priority should be given to low-cost and easily accessible screening technologies, such as abdominal ultrasound (for initial detection of gallstones/lesions) and serum tumor markers (e.g., CA19-9 for auxiliary screening), to avoid reliance on high-cost endoscopic equipment. These strategies not only align with the actual medical resource conditions in low-SDI regions but also focus on core prevention and control targets, and therefore have potential to increase intervention efficiency and equity.
Limitations and future directions
This study has several limitations. First, all analyses were based on estimated data from the GBD database. The accuracy of these estimates depends on the quality and completeness of original data from each country and territory. Regions with relatively underdeveloped medical systems were more likely to have underestimates, whereas for regions with missing data, the spatiotemporal modeling imputation method used by the GBD might have introduced uncertainty, particularly for rare cancers such as GBTCs [27]. Second, the relationship between the SDI and GBTC burden is an ecological correlation, which therefore carries a risk of ecological fallacy, wherein the association observed at the population level might not hold at the individual level, and potential influences of confounding factors such as detection effects and differences in coding standards cannot be excluded. For example, although we observed a positive correlation between national SDI and GBTC incidence, this finding does not imply that individuals with higher socioeconomic status within a country necessarily have elevated GBTC risk; individual-level factors (e.g., personal dietary habits, access to healthcare, or genetic susceptibility) might interact with societal SDI in ways not captured by aggregated data. Third, the GBD database provided limited information regarding GBTC subtypes (gallbladder cancer or intra/extrahepatic cholangiocarcinoma). Because subtypes have varying risk factors and prognosis, this limitation might affect the accuracy of the results, and future studies should analyze these subtypes individually [28]. Fourth, this study did not systematically evaluate individual risk factors such as obesity and gallstones. Because of the lack of detailed individual-level data in the GBD database, we were unable to quantify their independent associations or distinguish the boundary of their effects from those of socioeconomic and demographic factors. In summary, these limitations should be considered in interpreting regional differences in the findings, because such variations might reflect genuine epidemiological differences and underlying differences in data quality.
Future research should focus on three key areas. First, individual-level cohort studies should be conducted to link individual socioeconomic status and lifestyle factors with clinical outcomes, verify whether the ecological association might be applicable to individuals, and clarify the specific causal pathways through which the SDI affects GBTC burden. Second, molecular epidemiological studies should be strengthened to explore the biological mechanisms underlying the sex differences in GBTCs [29]. Third, efforts should focus on developing and validating low-cost, high-efficiency screening technologies suitable for different resource environments, conducting cost-benefit analyses to provide actionable intervention tools for low-SDI regions, and formulating evidence-based, cost-effective long-term management strategies. These efforts will be crucial to address the global burden of GBTCs.
Comparison with recent literature
GBTC epidemiology has been a focus of several recent global and regional studies. Compared with the previous literature, this study substantially differed in analytical scope, integration of socioeconomic factors, and practical applications of our predictions [30–32]. Regarding the analytical scope, studies such as those by Cui et al. [31] and Jiang et al. [23] focused on BRICS countries, whereas our analysis covered 204 countries or territories to capture global differences, thus enabling more comprehensive capture of global heterogeneity. Regarding integration of socioeconomic factors, Dai et al. [30] focused on exploring demographic or healthcare workforce correlates, whereas this study used the SDI and clearly distinguished ecological associations between SDI and incidence rate (data results) from inference due to risk factor transition, and further provided alternative explanations, such as detection effects, thereby enhancing the rigor of the conclusions. Regarding predictions, Liu et al. [32] and Zhan et al. [28] have forecasted to 2045 and 2030, respectively, whereas this study provided predictions until 2040. More importantly, we provided key warnings regarding the limitations of predictions and practical application guidelines rather than merely presenting trends, to align the findings with policy needs. Whereas Zhao et al. [11] focused on specific risk factors (e.g., high BMI) or global trends but did not integrate frontier analysis to identify performance gaps in disease control, our study clarified the intervention lag in low- and moderate-SDI regions through frontier analysis, thus providing a unique reference for setting priorities.
Beyond these methodological distinctions, the robustness and policy relevance of our findings were further strengthened by several key features of our study design. First, this study’s use of data from the 2021 GBD database ensured comprehensive geographical and temporal representativeness, by covering GBTC burden data from 204 countries and regions in 1990–2021. Second, our integration of multiple methods, such as joinpoint regression, frontier analysis, and ARIMA modeling, enabled a multi-dimensional and systematic investigation of epidemiological trends, socioeconomic drivers, and future trajectories. Third, this study’s sex-specific and SDI-stratified analyses addressed limitations of previous studies by providing detailed insights required for the formulation of customized prevention strategies.
Conclusion
This study demonstrated that the global burden of GBTCs between 1990 and 2021 presented a dual burden scenario comprising decreased age-standardized rates at the individual level due to advancements in medical care but a continual rise in absolute burden due to population growth and aging. Our analysis confirmed the significant sex-based heterogeneity and distinct socioeconomic gradient in the distribution of disease burden. The increase in male incidence rates and their positive correlation with the SDI underscored the effects of sex-specific risk factors and socioeconomic development levels. Predictions from ARIMA modeling suggested that, without enhanced interventions, the burden of male incidence will continue to rise through 2040. Consequently, tailored strategies are necessary: high-SDI regions should concentrate on controlling risk factors and improving long-term care systems, whereas low- and moderate-SDI regions must strengthen their early diagnostic capabilities. These strategies should be informed by regional context. For example, low-SDI countries might benefit from task-shifting diagnostic training to primary care providers, whereas high-SDI nations could integrate GBTC risk assessment into routine metabolic disorder screening. Additionally, cross-country knowledge sharing between frontier and lagging regions might accelerate a decrease in global burden. Future research should explore the mechanisms of SDI’s influence and the biological basis of sex differences to provide evidence for precision prevention and control.
Data availability statement
Not applicable.
Ethics statement
No direct interactions with human or animal subjects were involved. Therefore, ethical approval and informed consent were not required.
Author contributions
Yimao Wu and Guanyu Yang collected the data, performed the analyses, drafted the manuscript, and prepared the figures. Gokhan Zengin, Shuai Ren, and Mengyao Li conceptualized and designed the study, supervised the project, guided the process, and revised the manuscript. All authors have read and approved the final version of the manuscript.
Funding
This research was funded by the Young Elite Scientists Sponsorship Program of the China Association of Chinese Medicine (2024-QNRC2-B16), a project funded by the China Postdoctoral Science Foundation (2023M741808), the Young Elite Scientists Sponsorship Program of the Jiangsu Association for Science and Technology (JSTJ-2023-WJ027), the Natural Science Foundation of Nanjing University of Chinese Medicine (XZR2023036), and the Foundation of Excellent Young Doctor of Jiangsu Province Hospital of Chinese Medicine (2023QB0112).
Conflict of interest
The authors declare that there are no conflicts of interest.
Graphical abstract
Highlights
- Global trends revealed a critical dual burden in GBTCs, with declining age-standardized mortality and DALYs but rising absolute case counts.
- A distinct positive correlation was identified between age-standardized incidence rates and socioeconomic development (SDI), alongside a persistent male predominance in disease burden.
- Model projections indicated a continuing rise in age-standardized incidence rates among males through 2040, thus underscoring the need for sex-specific and development-stratified interventions.
In brief
The global burden of GBTCs poses a critical dual burden wherein decreasing age-standardized mortality contrasts with rising absolute cases. Analyses linked higher incidence to greater socioeconomic development and identified a persistent male predominance. Projections indicated a continuing rise in male incidence necessitating prevention strategies that are both sex-specific and tailored to different resource settings.
References
- Li JT, Gu A, Tang NN, Sun ZY, Zhang G, et al. Exploring anti-tumor potential of food and medicine homology substances: an in-silico evaluation of Citri Grandis Exocarpium against gallbladder cancer. Food Med Homol 2026;3(2):9420084. [DOI: 10.26599/FMH.2026.9420084]
- Tang N, Li J, Gu A, Li M, Liu Y. Single-cell multi-omics in biliary tract cancers: decoding heterogeneity, microenvironment, and treatment strategies. Mol Biomed 2025;6(1):82. [PMID: 41091402 DOI: 10.1186/s43556-025-00330-2]
- Zhang W, Wang YJ, Liu JM, Sun XH, Jiang Y, et al. Burden of biliary tract carcinoma in China (1990-2021): findings from the 2021 Global Burden of Disease Study. Sci Bull 2024;69(22):3547-57. [PMID: 39366826 DOI: 10.1016/j.scib.2k024.09.026]
- Zheng JX, Liu Y, Guan SY, Guo ZY, Duan L, et al. Global, regional, and national burden of neglected tropical diseases and malaria in the general population, 1990-2021: systematic analysis of the global burden of disease study 2021. J Adv Res 2026;79:769-81. [PMID: 40194698 DOI: 10.1016/j.jare.2025.04.004]
- Kamble S, Desai K, Joo S, Pandey P, Swami S, et al. Epidemiology, treatment patterns, and humanistic and economic burden of biliary tract carcinoma: a systematic and targeted literature review. J Clin Oncol 2024;42(3 suppl):443. [DOI: 10.1200/JCO.2024.42.3_suppl.443]
- Lin XL, Zhang QW, Chen GF, Yang SJ, Li XB, et al. Global, regional, and national trends in metabolic risk factor-associated mortality among the working-age population from 1990-2019: an age-period-cohort analysis of the Global Burden of Disease 2019 study. Metabolism 2024;157:155954. [PMID: 38878856 DOI: 10.1016/j.metabol.2024.155954]
- Zhao ZY, Li JJ, Ouyang HQ, Li WH, Huang SK, et al. Enhancing regional disease burden estimates: insights from the comparison of Global Burden of Disease and China’s notifiable infectious diseases data with policy implications (2010-2020). Infect Dis Poverty 2025;14(1):81. [PMID: 40770780 DOI: 10.1186/s40249-025-01351-3]
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024;403(10440):2133-61. [PMID: 38642570 DOI: 10.1016/S0140-6736(24)00757-8]
- Loia V, Orciuoli F, Pedrycz W. Towards a granular computing approach based on formal concept analysis for discovering periodicities in data. Knowl Based Syst 2018;146:1-11. [DOI: 10.1016/j.knosys.2018.01.032]
- Salman AG, Kanigoro B. Visibility forecasting using autoregressive integrated moving average (ARIMA) models. Procedia Comput Sci 2021;179:252-9. [DOI: 10.1016/j.procs.2021.01.004]
- Zhao M, Zhai H, Li H, Wei F, Ma H, et al. Age-standardized incidence, prevalence, and mortality rates of autoimmune diseases in adolescents and young adults (15-39 years): an analysis based on the global burden of disease study 2021. BMC Public Health 2024;24(1):1800. [PMID: 38970015 DOI: 10.1186/s12889-024-19290-3]
- Kim HJ, Luo J, Kim J, Chen HS, Feuer EJ. Clustering of trend data using joinpoint regression models. Stat Med 2014;33(23):4087-103. [PMID: 24895073 DOI: 10.1002/sim.6221]
- Kinnamon DD, Martin ER. Valid Monte Carlo permutation tests for genetic case-control studies with missing genotypes. Genet Epidemiol 2014;38(4):325-44. [PMID: 24723341 DOI: 10.1002/gepi.21805]
- Yu SC, Wang QQ, Long XJ, Hu YH, Li JQ, et al. [Multiple linear regression models with natural logarithmic transformations of variables]. Zhonghua Yu Fang Yi Xue Za Zhi 2020;54(4):451-6 (in Chinese). [PMID: 32268656 DOI: 10.3760/cma.j.cn112150-20191030-00824]
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2197-223. [PMID: 23245608 DOI: 10.1016/S0140-6736(12)61689-4]
- Wisniewski SJ, Brannan GD. Correlation (coefficient, partial, and spearman rank) and regression analysis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025.
- Downs SM, Ahmed S, Warne T, Fanzo J, Loucks K. The global food environment transition based on the socio-demographic index. Glob Food Secur 2022;33:100632. [DOI: 10.1016/j.gfs.2022.100632]
- Chen J, Lin A, Luo P. Advancing pharmaceutical research: a comprehensive review of cutting-edge tools and technologies. Curr Pharm Anal 2024;21(1):1-19. [DOI: 10.1016/j.cpan.2024.11.001]
- Zhao Y. R and data mining: examples and case studies. Cambridge, Massachusetts, USA. Academic Press; 2012.
- Schaffer AL, Dobbins TA, Pearson SA. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. BMC Med Res Methodol 2021;21(1):58. [PMID: 33752604 DOI: 10.1186/s12874-021-01235-8]
- Sonkin D, Thomas A, Teicher BA. Cancer treatments: past, present, and future. Cancer Genet 2024;286-287:18-24. [PMID: 38909530 DOI: 10.1016/j.cancergen.2024.06.002]
- Xiao Y, Hong X, Neelagar R, Mo H. Age-standardized incidence, prevalence, mortality rates and future projections of autoimmune diseases in China: a systematic analysis based on GBD 2021. Immunol Res 2025;73(1):26. [PMID: 39762576 DOI: 10.1007/s12026-024-09591-5]
- Jiang Z, Jiang Q, Wang P, Zhong L. Gallbladder and biliary tract cancer burdens in China from 1990 to 2021 and projection to 2044: findings from the 2021 Global Burden of Disease study. Front Med 2025;12:1592621. [PMID: 40417698 DOI: 10.3389/fmed.2025.1592621]
- Li MY, Zhang Q, Li J, Zengin G. Food and medicine homology in cancer treatment: traditional thoughts collide with scientific evidence. Food Med Homol 2025;2(3):9420120. [DOI: 10.26599/FMH.2025.9420120]
- Li MY, Zhang H, Li J, Chen YS, Ren S, et al. Reshaping the future of cancer therapy: taming toxicity and side effects. Biomed Eng Commun 2026;5(2):11. [DOI: 10.53388/BMEC2026011]
- Li MY, Gu A, Li J, Tang N, Matin M, et al. Exploring food and medicine homology: potential implications for cancer treatment innovations. Acta Mater Medica 2025;4(2):200-6. [DOI: 10.15212/AMM-2025-0003]
- GBD 2023 Cancer Collaborators. The global, regional, and national burden of cancer, 1990-2023, with forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2023. Lancet 2025;406(10512):1565-86. [PMID: 41015051 DOI: 10.1016/S0140-6736(25)01635-6]
- Zhan Z, Chen B, Teng W, Huang R, Zheng H, et al. Trends and projections of gallbladder and biliary tract cancer in China: a comprehensive analysis from 1990 to 2030 based on the Global Burden of Disease Study 2021. BMC Public Health 2025;25(1):2409. [PMID: 40629282 DOI: 10.1186/s12889-025-23601-7]
- Li J, Gu A, Tang N, Zengin G, Li MY, et al. Patient-derived xenograft models in pan-cancer: from bench to clinic. Interdiscip Med 2025;3(5):e20250016. [DOI: 10.1002/INMD.20250016]
- Dai F, Cai Y, Yang S, Zhang J, Dai Y. Global burden of gallbladder and biliary diseases (1990-2021) with healthcare workforce analysis and projections to 2035. BMC Gastroenterol 2025;25(1):249. [PMID: 40221715 DOI: 10.1186/s12876-025-03842-x]
- Cui YL, Bao X, Liu DM, Mu H, Yu G. Gallbladder and biliary tract cancer burden trends in Brazil, Russian Federation, India, China, and South Africa in 1990-2021. World J Gastrointest Oncol 2025;17(8):109245. [PMID: 40837750 DOI: 10.4251/wjgo.v17.i8.109245]
- Liu C, Du S, Liu X, Niu W, Song K, et al. Global, regional, and national burden of gallbladder and biliary tract cancer, 1990 to 2021 and predictions to 2045: an analysis of the Global Burden of Disease study 2021. J Gastrointest Surg 2025;29(3):101968. [PMID: 39848314 DOI: 10.1016/j.gassur.2025.101968]