Harnessing Ultrasound for Tumor Vascular Targeting: From Mechanistic Insights to Clinical Monitoring and Therapeutic Applications
1Key Laboratory of Medical Imaging Precision Theranostics and Radiation Protection, College of Hunan Province, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Changsha, China
2Department of Medical Imaging, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Changsha, China
3Institute of Medical Imaging, Hengyang Medical School, University of South China, Hengyang, China
4Warwick Medical School, The University of Warwick, Coventry, CV4 7AL, United Kingdom
aThese authors contributed equally to this work and share first authorship.
*Correspondence to: Meng Du, E-mail: dumeng_work@126.com; Youchao Chen, E-mail: Youchao.Chen@warwick.ac.uk
Received: June 17 2025; Revised: September 22 2025; Accepted: December 4 2025; Published Online: April 1 2026.
Cite this paper:
Lei L, Yang H, Du M et al. Harnessing Ultrasound for Tumor Vascular Targeting: From Mechanistic Insights to Clinical Monitoring and Therapeutic Applications. BIO Integration 2026; 7: 1–24.
DOI: 10.15212/bioi-2025-0117. Available at: https://bio-integration.org/
Download citation 
© 2026 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
The tumor vasculature, characterized by pathological angiogenesis and structural abnormalities, drives the progression of solid tumors by inducing hypoxia-acidosis microenvironments and therapeutic resistance. Targeting the tumor vasculature has emerged as a critical therapeutic strategy. Although conventional approaches such as anti-angiogenic drugs, vascular disrupting agents, and embolization have shown efficacy, their single-target focus hinders addressing tumor heterogeneity and evolving stage-specific needs. For example, rapid vascular disruption is effective for debulking advanced tumors, whereas vascular normalization enhances early- to mid-stage therapy by improving postoperative chemo-radiotherapy outcomes. Unlike single-mechanism interventions, ultrasound modulates acoustic parameters to achieve diverse effects including angiogenesis suppression, vessel disruption, and vasodilation, thus addressing multi-stage vascular needs. Ultrasound-based monitoring systems provide precise, dynamic vascular assessments to guide intervention strategies. Compared with traditional static imaging ultrasound offers real-time angiogenesis visualization and therapeutic response evaluation, thus enabling treatment optimization. This review synthesizes recent advances in ultrasound-based vascular targeting, emphasizing its dual role in spatiotemporally adaptive therapy and angiogenesis monitoring. We critically examine clinical translation challenges and future directions, highlighting how ultrasound-driven strategies, by bridging mechanistic precision with clinical scalability, might enable personalized, multi-effect therapeutic paradigms in oncology.
Keywords
Anti-angiogenesis, tumor microenvironment, tumor vasculature, ultrasound, vascular monitoring, vascular normalization.
Introduction
The tumor vasculature is critical in solid tumor progression, in which pathological angiogenesis is driven primarily by VEGF-mediated signaling cascades, to meet the high demand for oxygen and nutrients to fuel tumor cells’ rapid proliferation [1–3]. Unlike the physiological vasculature, tumor vessels exhibit extensive structural abnormalities including disorganized endothelial architecture, discontinuous basement membranes, and deficient pericyte coverage, thus resulting in hyperpermeability and hemodynamic dysfunction [4–6]. Functionally, these malformations impair convective transport, and consequently increase interstitial fluid pressure via plasma protein extravasation and aberrant extracellular matrix deposition [7–9]. The resultant hypoxia-acidosis microenvironment fosters therapeutic resistance while promoting immunosuppression and metastatic dissemination [10]. Consequently, vascular targeting has emerged as a foundational strategy in precision oncology [11].
Current anti-tumor vascular therapeutics are based on two mechanistic paradigms: (1) vascular deprivation through angiogenesis inhibition or vessel destruction to induce tumor ischemia and (2) vascular normalization to restore hemodynamic competence for enhanced therapeutic perfusion [12]. On the basis of these mechanisms, various tumor vascular targeting strategies have been developed, including anti-angiogenic therapy, vascular disruption therapy, and interventional embolic agents [13, 14]. However, these strategies often have single-purpose effects that cannot meet the dynamic demands of treating tumors at different stages under various scenarios. For patients with advanced-stage tumors who are unable to undergo surgery, vascular inhibition or destruction during active tumor angiogenesis, in which tumors rely on newly formed blood vessels, can rapidly decrease tumor burden and prolong survival [15, 16]. In contrast, during early to mid-stages of tumor development, when the treatment goal is enhancing local control rates through radiotherapy and chemotherapy, interventions that restore vascular function and increase perfusion to enhance drug delivery, optimize the tumor microenvironment, and decrease treatment resistance might be more beneficial [9, 12].
Ultrasound enables dynamic and diverse tumor vascular interventions, and overcomes the limitations of existing single-mechanism therapies. This modality’s multiple effects include angiogenesis suppression, vessel disruption, and vasodilation [12, 17, 18]. For example, therapeutic ultrasound (mechanical index = 1.3/1.4) stimulates endothelial cells, upregulates endothelial nitric oxide synthase expression, and promotes nitric oxide (NO) release, thereby improving blood perfusion in the target tissue, lowering interstitial pressure, and fostering a favorable microenvironment for chemotherapy or radiotherapy [18, 19]. In contrast, high-intensity focused ultrasound induces mechanical stress through inertial cavitation, and results in endothelial cell damage, widespread vessel closure, and tumor ischemic necrosis [20]. Compared with conventional methods such as localized embolization, ultrasound-based vascular disruption offers advantages such as non-invasive and repeatable treatments.
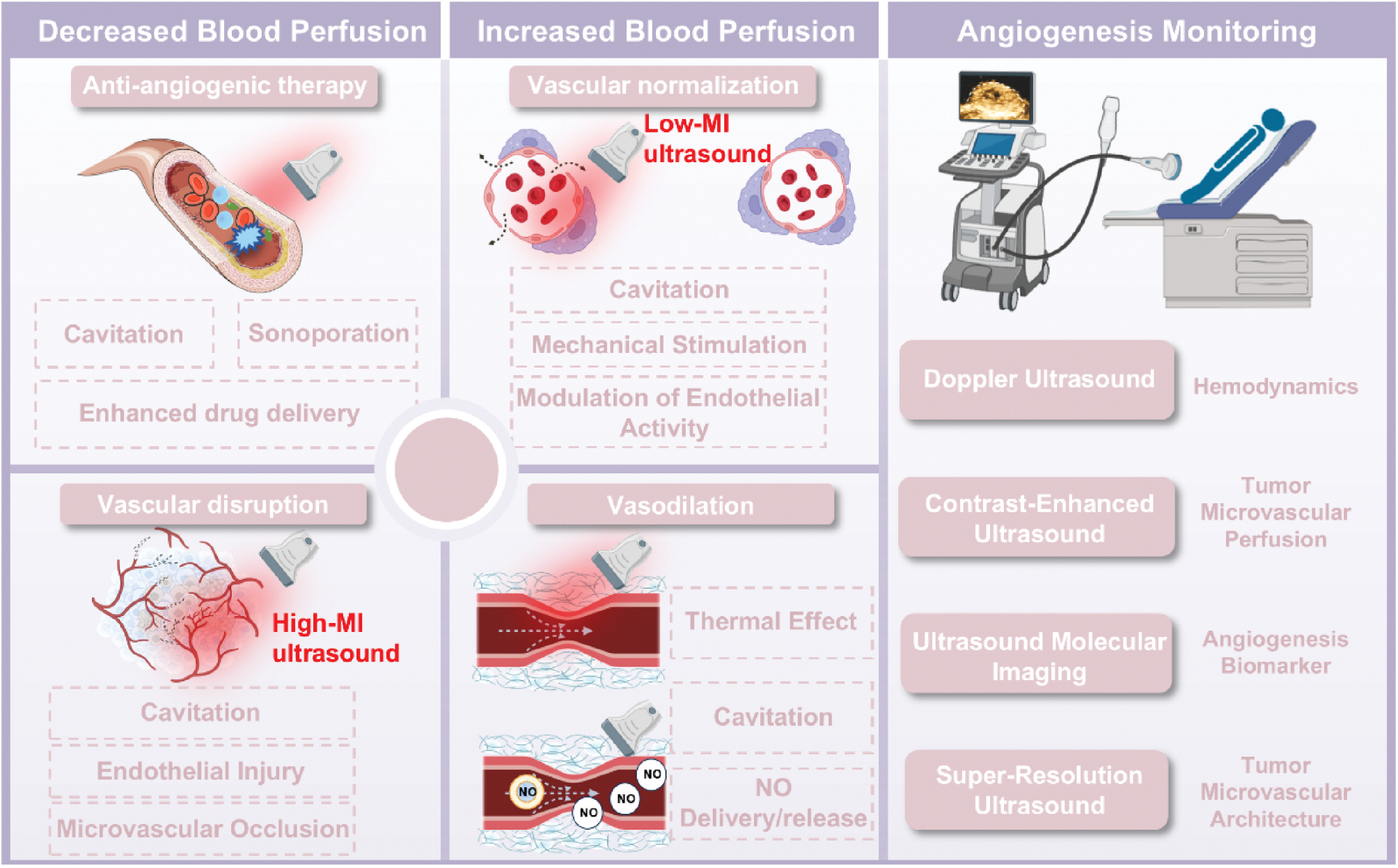
Moreover, the precise implementation of tumor vascular targeting requires dynamic monitoring of angiogenesis, focusing on real-time, detailed representation of tumor vascular structures, such as microvessel density (MVD), morphology, spatial distribution, function, and molecular signaling alterations [21–23]. Ultrasound-based angiogenesis monitoring integrates therapeutic functionality with real-time, multimodal imaging capabilities. Technologies such as contrast-enhanced ultrasound (CEUS), super-resolution ultrasound (SR-US), and ultrasound molecular imaging (UMI) enable simultaneous visualization of vascular structures, quantification of blood perfusion, and targeted identification of specific molecular markers [24, 25]. This review discusses current advancements in ultrasound-based therapies for efficient tumor treatment, and highlights ultrasound as a multi-effect diagnostic and therapeutic tool for targeting the tumor vasculature (Figure 1). The key mechanisms underlying vascular targeting in tumor treatment are explored, with a focus on ultrasound-based strategies. Additionally, current progress in ultrasound-based tumor vascular monitoring technologies is reviewed, and the challenges and future prospects for clinical translation are examined.
Figure 1 Ultrasound-based strategies for tumor vascular theranostics.
Targeting the vasculature for enhanced therapeutic efficacy
Given the central role of angiogenesis in sustaining tumor growth and progression, targeting the tumor vasculature has emerged as a compelling therapeutic strategy [26]. Tumor-vasculature-targeted therapies have markedly evolved in recent decades. Early strategies focused on inhibiting angiogenesis or disrupting existing vascular networks to induce “starvation therapy.” These approaches have since expanded to correcting vascular abnormalities (e.g., hyperpermeability or tortuosity) and promoting vasodilation, thereby improving perfusion, decreasing hypoxia, and enhancing the efficacy of concurrent treatments such as chemotherapy and radiotherapy.
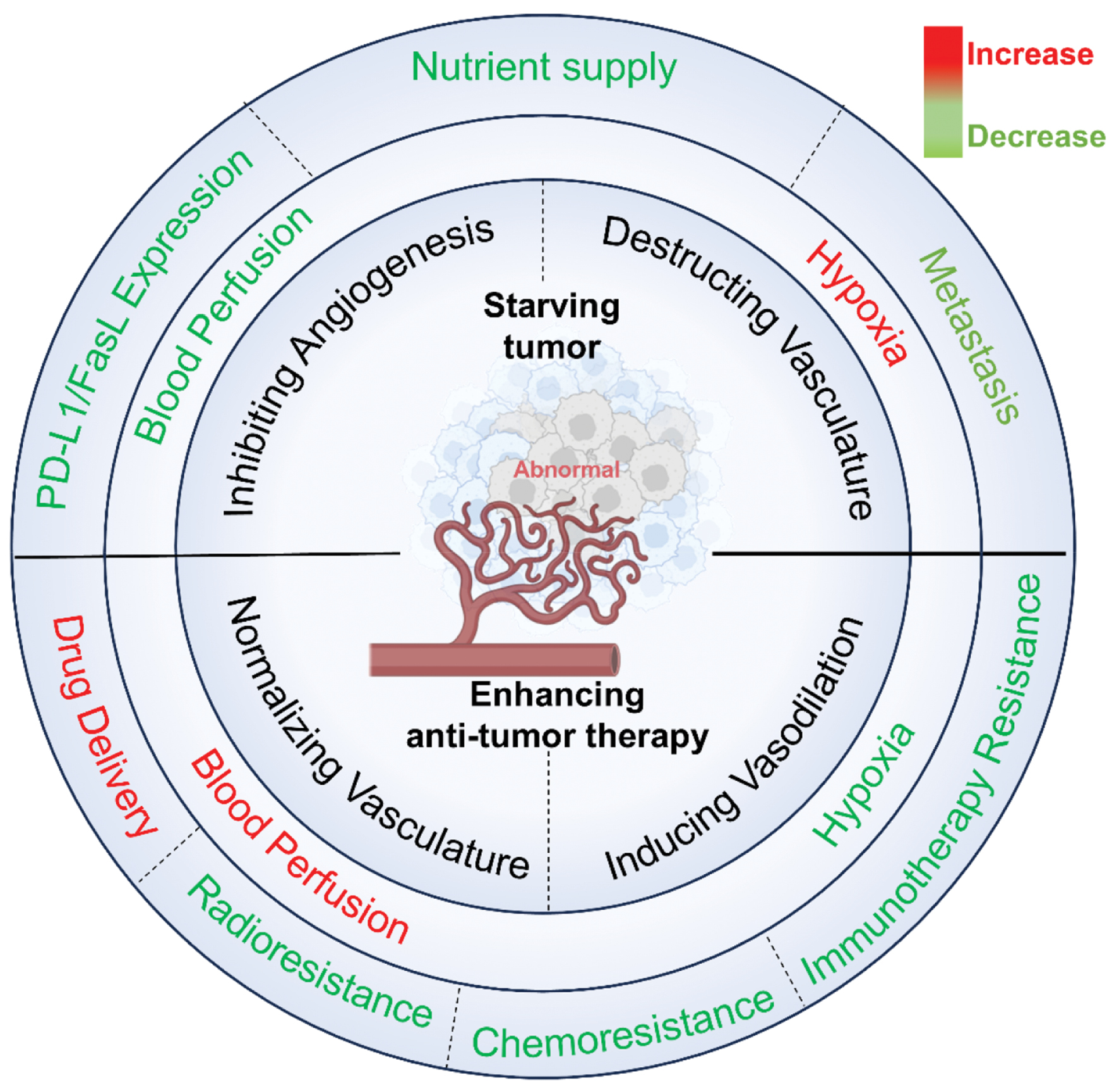
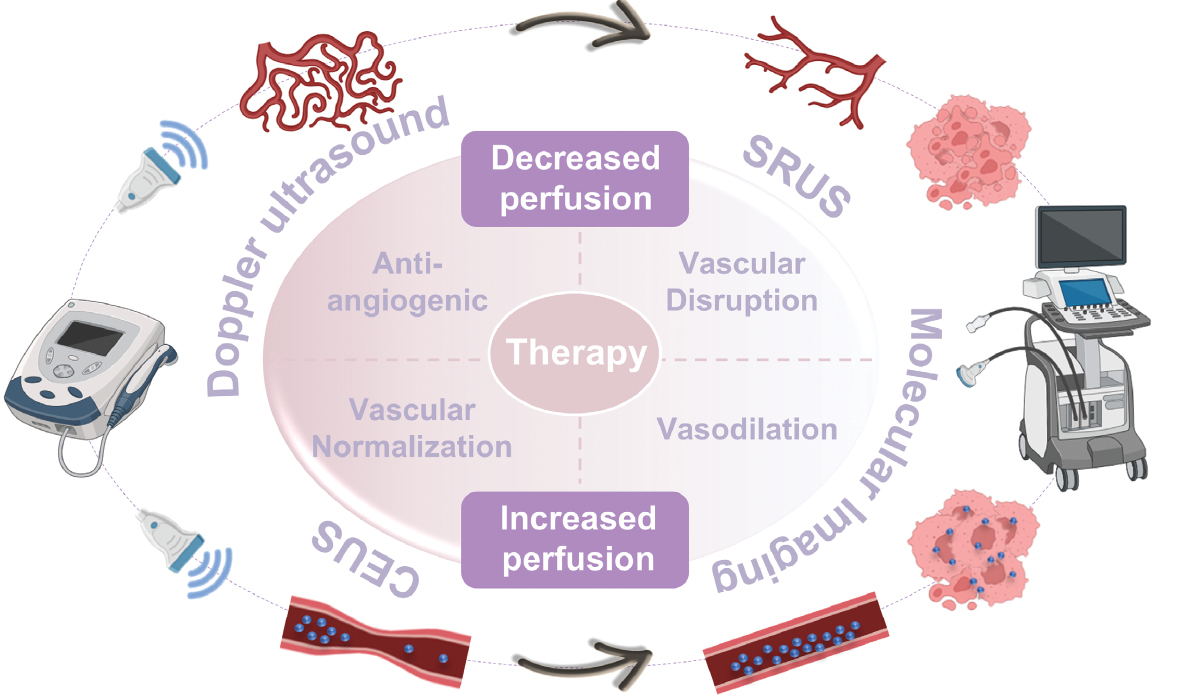
The success of these strategies critically depends on the dynamic functional state of the vasculature. A thorough understanding of how vasculature targeting influences tumor progression is essential for designing personalized vascular-targeted therapies. Figure 2 illustrates the mechanistic interactions between vasculature targeting and tumor therapy.
Figure 2 Mechanistic interactions between vasculature targeting and tumor therapy.
Targeting the tumor vasculature to impair tumor perfusion: starving the tumor
Tumors exhibit dysregulated metabolic activity and elevated proliferation and metastasis ability. Because the tumor vasculature is a critical conduit for nutrient and oxygen delivery, its disruption is a logical therapeutic target [27]. “Starving” tumors is aimed at inducing ischemia and nutrient deprivation within tumors by either preventing neovascularization (anti-angiogenic therapy) or destroying existing tumor vessels (vascular disruption therapy). Both strategies can lead to rapid cessation of blood flow and central tumor necrosis [28]. However, these approaches often have limited efficacy against peripheral tumor regions, where more mature and resilient vessels can persist [29]. Therefore, combinatorial strategies integrating starvation therapies with conventional treatments are under active investigation to enhance therapeutic outcomes [30].
Beyond nutrient and oxygen supply, structurally abnormal vasculature contributes to tumor progression and metastasis. For example, the overexpression of matrix metalloproteinases during angiogenesis facilitates extracellular matrix degradation and consequently enhances local invasion [31]. Irregular vessel walls also provide accessible routes for tumor cells to intravasate and disseminate systemically [32]. Recent studies have highlighted a close interplay between angiogenesis and immune suppression within the TME. Endothelial cells in aberrant tumor vasculature frequently upregulate immunosuppressive molecules such as programmed death-ligand 1 (PD-L1) and Fas ligand (FasL), which inhibit cytotoxic T-cell infiltration and activation [33]. By targeting these abnormal vessels, starving tumors might not only deprive tumors of essential resources but also reverse immune exclusion, thereby amplifying anti-tumor immune responses. These multifaceted mechanisms underscore the therapeutic potential of vascular-targeted strategies in achieving sustained tumor control.
Restoring vessels to enhance tumor perfusion: improving treatment efficacy
Because angiogenesis is a critical requirement for tumor growth and progression, anti-angiogenic therapy was initially conceived as a promising strategy for cancer treatment. However, clinical trials combining anti-angiogenic agents with chemotherapy have consistently not increased overall survival rates in multiple malignancies, including breast, pancreatic, and prostate cancers [34]. Notably, a preclinical study challenged this conventional paradigm by integrating low-dose cilengitide (a pro-angiogenic agent) with verapamil (a vasodilator) and the chemotherapeutic agent gemcitabine. This counterintuitive strategy, antipodal to traditional anti-angiogenic approaches, paradoxically enhanced tumor vascular density and blood perfusion while effectively suppressing tumor growth and metastasis in mouse models of pancreatic ductal adenocarcinoma and non-small cell lung cancer [35, 36]. These paradoxical findings illuminated an alternative vascular-targeting approach: rather than inducing vascular starvation, targeting the tumor vasculature to enhance blood perfusion might provide a new perspective for treating tumors.
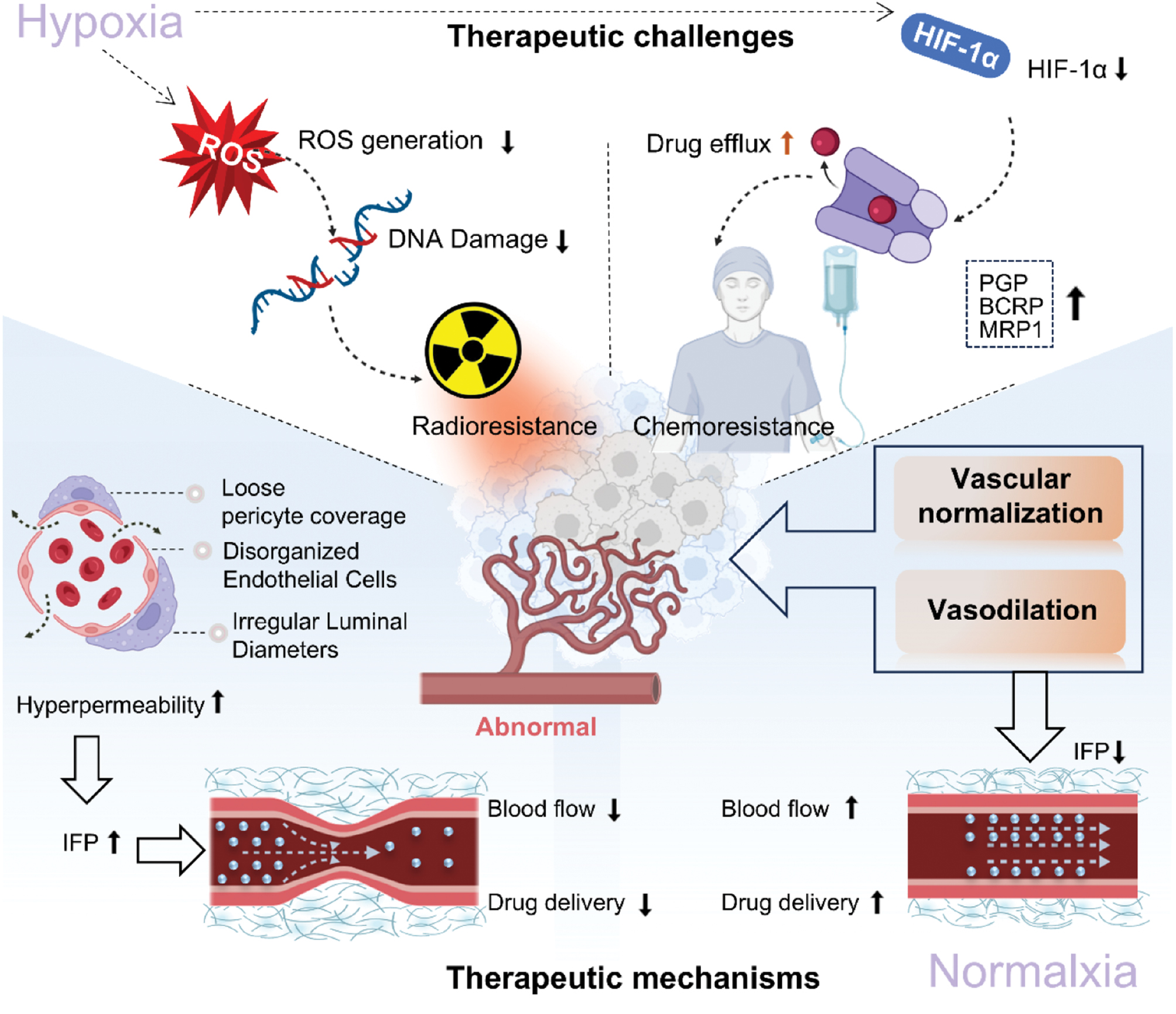
Strategies such as vascular normalization or vasodilation are aimed at restoring vascular function and improving blood flow, thereby improving the hypoxic tumor microenvironment and enhancing drug delivery efficiency [14] (Figure 3). The hypoxic microenvironment plays a crucial role in tumor resistance. Hypoxic tumor cells exhibit three times greater resistance to radiation than normoxic cells [37]. This phenomenon, known as the “oxygen effect,” first described by Gray et al. [38], occurs because radiotherapy relies on oxygen to produce reactive oxygen species, which induce DNA damage and cell death [39, 40]. Moreover, hypoxia can activate HIF-1α and consequently upregulate drug efflux pumps such as P-glycoprotein, breast cancer resistance protein, and multidrug resistance protein 1, which together contribute to chemoresistance in solid tumors including breast and colorectal cancers, thus posing treatment challenges [41, 42]. Therefore, enhancing blood flow and alleviating the hypoxic microenvironment are essential for increasing the efficacy of anti-tumor therapy.
Figure 3 Therapeutic challenges of abnormal tumor vessels and therapeutic mechanisms of vessel restoration.
In chemotherapy and radiotherapy, the distribution of drugs or radiosensitizers within tumors is another critical factor influencing treatment outcomes. Vascular normalization has been shown to improve drug distribution and increase bioavailability in preclinical models [43, 44]. For example, enhancing pericyte coverage and stabilizing the tumor vasculature have successfully inhibited the progression of Lewis lung cancer in preclinical models [45]. Furthermore, emerging evidence highlights the interaction between abnormal tumor vasculature and anti-tumor immunity. Restoring normal vascular structure and function enhances immune cell infiltration, promotes dendritic cell maturation, and improves antigen presentation. Simultaneously, decreased recruitment of immunosuppressive cells (such as regulatory T cells and myeloid-derived suppressor cells) alleviates immunosuppression [46–49]. These findings underscore the substantial potential of targeting the tumor vasculature to enhance the efficacy of anti-tumor therapies by improving blood flow perfusion and restoring vascular function.
Ultrasound-based tumor vasculature targeting strategies
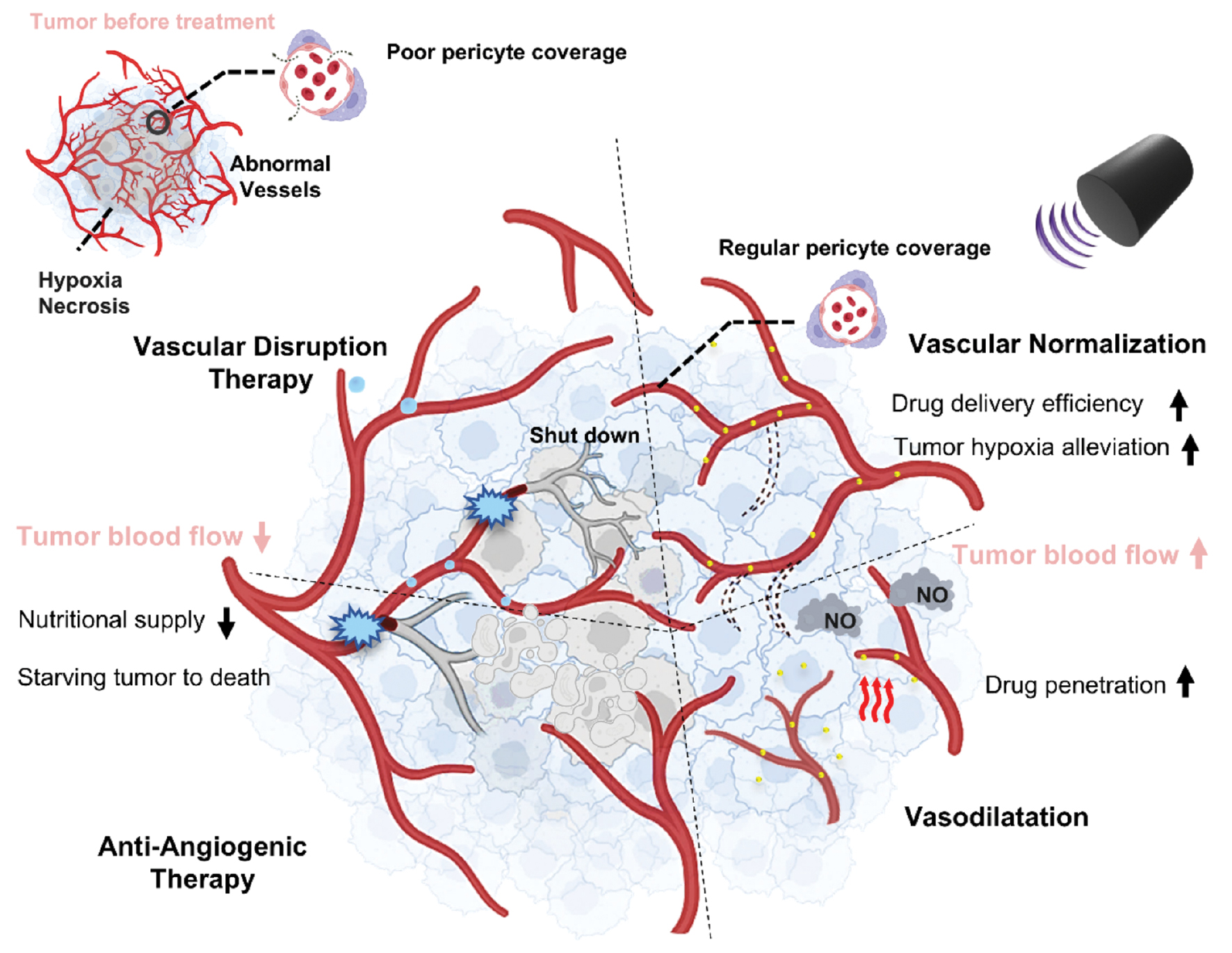
Ultrasound, a non-invasive physical regulatory tool, is emerging as a promising method to overcome tumor resistance. Its mechanisms extend beyond the thermal ablation effects of traditional high-intensity focused ultrasound (HIFU) on tumor tissues, by including multimodal effects such as mechanical stress and cavitation. These mechanisms enable targeted treatment of blood vessels to enhance tumor therapy efficiency. Ultrasound-based targeted vascular strategies have been successfully applied in areas such as anti-angiogenesis, vascular disruption, vascular normalization, and vasodilation, and have yielded favorable therapeutic results (Figure 4).
Figure 4 Ultrasound-based targeting strategies for the tumor vasculature. Tumors exhibit abnormal vessels with poor pericyte coverage, thus leading to hypoxia necrosis and compromised nutritional supply, a microenvironment that fosters resistance to conventional therapies. Ultrasound-based targeted vascular strategies can decrease blood flow through anti-angiogenesis and vascular disruption to starve tumors; alternatively, they can improve tumor treatment efficacy by enhancing drug delivery efficiency, alleviating hypoxia, and enabling deeper drug penetration through vascular normalization and vasodilation.
Starving the tumor: ultrasound-based anti-angiogenic therapy
Judah Folkman’s concept of “starving a tumor to death” by targeting its vasculature laid the foundation for anti-angiogenic therapy more than 55 years ago [16]. In the past two decades, phase II and III trials have shown that anti-angiogenic therapy moderately improves survival in patients with solid tumors [50]. Drugs including bevacizumab (Avastin), sunitinib, axitinib, vandetanib, and ramucirumab are now clinically or preclinically approved [51]. However, these therapies face challenges including resistance, toxicity, and the absence of effective biomarkers. Tumor vessels, which are irregular and highly permeable, lead to elevated interstitial pressure and decreased blood perfusion, thus limiting the efficacy of anti-angiogenic drugs and contributing to tumor resistance [52, 53].
Ultrasound-based anti-angiogenic strategies are aimed at enhancing drug delivery and improving the tumor microenvironment. Ultrasound, when combined with microbubbles (MBs), induces oscillations and collapse of the MBs, thus generating mechanical forces that create transient openings in vascular walls; this process, known as sonoporation or acoustic cavitation, enhances penetration of therapeutic agents into tumors [54, 55]. MB-based drug delivery has potential in overcoming the biological barriers, such as dense extracellular matrix and high interstitial pressure, that limit traditional chemotherapy [56].
Targeted MBs functionalized with ligands specific to tumor biomarkers (e.g., VEGFR2 or integrin αvβ3) have been found to increase drug accumulation at tumor sites. VEGFR2-targeted microbubbles significantly enhanced the therapeutic effect of doxorubicin in a hepatocellular carcinoma model, as demonstrated by reduced tumor volume, inhibited angiogenesis, and increased apoptosis [57]. In addition, pH-sensitive polymer MBs that selectively release doxorubicin in the acidic tumor microenvironment, created by Liu et al., have decreased tumor volume by 60% while minimizing cardiotoxicity [58]. Barmin et al. have enhanced MB stability and drug loading by incorporating cross-linked shell structures enabling sustained drug release over multiple ultrasound sessions [59]. Additionally, Ingram et al. have designed a hybrid system encapsulating SN38 (a topoisomerase inhibitor) in liposomes attached to MBs, which has been found to improve systemic stability [60]. Ultrasound-induced cavitation transiently increases vascular permeability through sonoporation, wherein oscillating MBs disrupt endothelial tight junctions. Additionally, ultrasound-responsive nanoswitches, such as those developed by Huo et al., can release approximately 70% of their encapsulated doxorubicin payload upon ultrasound exposure, thus enhancing cancer cell inhibitory effects [61]. The spatio-temporal control of drug activity can be fine-tuned by adjusting ultrasound exposure times [62].
Starving the tumor: ultrasound-based vascular disruption therapy
Targeting the tumor vasculature to starve tumors has promise in decreasing tumor burden and extending survival. However, anti-angiogenic therapy primarily affects newly formed blood vessels, whereas pre-existing blood vessels are strengthened because of increased coverage by pericytes, thus leading to treatment resistance [12]. In clinical studies, anti-angiogenic drugs have shown low sensitivity in advanced tumors and have failed to achieve long-term control of cancer [63]. Additionally, alternative vascularization patterns in tumors, which are not dependent on angiogenesis, such as vasculogenic mimicry and vessel co-option, are not targeted by anti-angiogenic therapies and therefore do not respond to them [12]. Given the limitations of anti-angiogenic therapy, another strategy has emerged to starve tumors by directly damaging blood vessels and selectively inducing thrombosis to block the tumor vasculature [64]. Transarterial embolization, a regional treatment designed to control local disease by occluding the principal arterial supply to tumors, exhibits limitations in completely blocking blood flow in patients with multifocal HCC [65]. Vascular disrupting agents (VDAs), which selectively target the established tumor vasculature and decrease tumor burden, provide a promising alternative. This novel class of drugs specifically disrupts aberrant tumor vessels by either targeting the cytoskeleton or delivering pro-apoptotic factors, thereby inducing thrombosis, vascular occlusion, and subsequent extensive ischemic tumor necrosis [66]. The selectivity of VDAs toward the tumor vasculature arises from tumor endothelial cells’ frequent deficiency in pericyte and smooth muscle coverage, and their reliance on microtubulin for structural integrity [67]. Inhibition of microtubulin function by VDAs triggers morphological contraction and rounding of endothelial cells, and results in vascular lumen obstruction, vessel collapse, and ultimately interruption of blood flow [68]. In contrast, normal blood vessels, which are stabilized by intact pericytes and smooth muscle, display greater endothelial stability and resistance to VDA-induced effects [66]. Combretastatin, a representative VDA, induces hemorrhagic necrosis in tumors, decreases blood flow, and impairs oxygen and nutrient delivery, thereby inhibiting tumor growth [69]. Combretastatin A4 (CA4), a prototype VDA, and its phosphate prodrug, CA4 phosphate (CA4P), have entered phase III clinical trials [70].
Multiple clinical studies have demonstrated that the combination of VDAs with chemotherapy significantly improves the treatment of various advanced and metastatic solid tumors, such as prostate cancer, breast cancer, and ovarian cancer, and also significantly extends survival [71–73]. Despite promising clinical efficacy, concerns regarding VDA toxicity persist. VDAs currently in clinical trials, such as cemadotin, TZT-1027, and ASA404, have been shown to have dose-limiting toxicities, most commonly neutropenia [74]. Therefore, the selection of drug doses, monitoring of drug clearance, and identification of sensitive patients for combination therapy pose major challenges in the development of personalized treatment strategies.
Anti-vascular ultrasound has been shown to act as a physical equivalent of small-molecule vascular disrupting agents in achieving vascular disruption and controlling tumor growth [75]. This method, which uses high-pressure focused ultrasound to induce microvascular blood flow occlusion and subsequent ischemic tissue necrosis, is referred to as mechanical ablation, vascular disruption therapy, or more commonly anti-vascular ultrasound (AVUS) [17]. Ultrasound-induced MB destruction directly damages tumor endothelial cells via physical forces (shear stress and shockwaves), thus triggering apoptosis and increasing tumor sensitivity to radiotherapy [76]. Clinical trials have further demonstrated the feasibility and early safety of ultrasound combined with transarterial radioembolization in HCC treatment [77]. As of 2020, the combination of AVUS and radiation therapy had advanced into clinical trials for head and neck cancer, chest wall cancer, and locally advanced breast cancer [78]. The mechanism involves the cavitation effect of ultrasound-induced MBs, which mechanically disrupt the endothelial cell membrane and activate phospholipid-based biomechanical pathways, thereby enhancing the radiosensitivity of endothelial cells [79]. Endothelial apoptosis disrupts vascular integrity, thereby decreasing blood flow to tumors, depleting cellular energy, and inhibiting DNA repair enzyme activity. Restricted supply of DNA repair substrates further weakens repair capacity and enhances radiotherapy efficacy [80]. Unlike VDAs, ultrasound MB destruction decreases vascular density by as much as 67%, without worsening tumor hypoxia within 3 hours post-treatment [81]. This strategy avoids activation of hypoxia-related pathways (e.g., HIF-1α) and consequently preserves tumor radiosensitivity.
Moreover, the efficacy of ultrasound-mediated vascular disruption is influenced by ultrasound exposure conditions, MB behaviors, and vascular heterogeneity (vessel diameter, pericyte coverage, and endothelial integrity) [82]. Adjusting ultrasound parameters enables targeted disruption of blood vessels in tissues of varying sizes and maturity. Mature vasculature, with intact neuro-muscular structures, activates endothelial nitric oxide synthase in response to cavitation-induced shear stress, thereby promoting NO generation and vasodilation. In contrast, immature vasculature, which lacks this protective mechanism, is preferentially targeted. In mouse dorsal window tumor models, ultrasound pressures of 1–3 MPa cause vascular closure, primarily in smaller vessels (<20 μm), which is characterized by deformation and mild leakage. At 2 MPa, cavitation extends to moderately mature vessels (20–50 μm), with local thrombus formation. At 3 MPa, inertial cavitation significantly increases, thus disrupting endothelial barriers in vessels >50 μm and resulting in blood flow stagnation (80.6%) [79]. Tumor vascular heterogeneity affects treatment outcomes: lower energy attenuation in the tumor center requires longer pulse durations to effectively target mature vessels in the periphery.
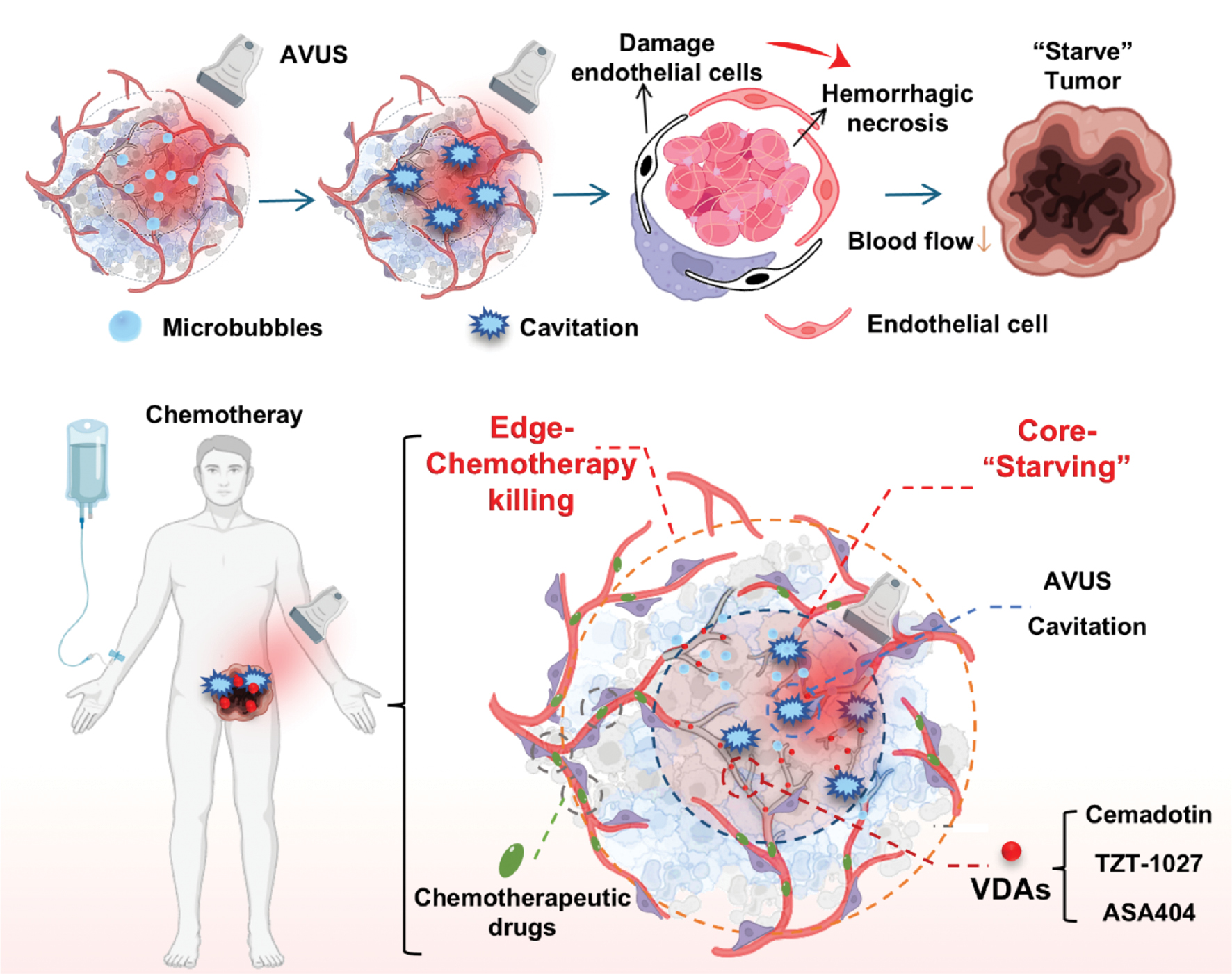
AVUS additionally exhibits favorable synergy with chemotherapy in tumor treatment [83, 84]. Although vascular disruption therapy theoretically decreases the efficiency of drug delivery and might decrease chemotherapy efficacy, clinical trials have explored the use of ultrasound cavitation to enhance the efficacy of systemic chemotherapy in patients with pancreatic cancer. As early as 2005, a chemotherapy strategy based on VDAs was proposed to prevent the survival of tumor cells at the edges of necrotic cores and potentially overcome tumor treatment resistance [85]. These complementary therapeutic effects based on spatial distribution occur because VDAs and anti-vascular ultrasound preferentially damage smaller, less mature microvessels in the tumor core, whereas the delivery of chemotherapeutic agents and other anticancer drugs relies predominantly on relatively well-established intratumoral vasculature (on the edge) for delivery [86] (Figure 5). Pellow et al. have designed monodisperse, size-tunable nanodroplets to achieve high vascular occlusion rates while minimizing the occurrence of other vascular events [17]. Additionally, given the risks associated with the activation of the fibrinolytic system in the body, antifibrinolytic agents have been proposed to precisely destroy tumor vascular endothelial cells while inducing thrombotic ischemia in tumors [87].
Figure 5 Mechanisms underlying the synergistic effects between AVUS and chemotherapy. AVUS and VDAs both preferentially disrupt immature tumor vasculature in the core region. AVUS induces MB cavitation, which mechanically disrupts endothelial cell membranes, induces hemorrhagic necrosis, disrupts tumor blood flow, and effectively “starves” the tumor core. Chemotherapeutic drugs act primarily on the more mature tumor vasculature in the periphery. These agents achieve synergistic tumor killing through complementary spatial targeting.
Improving treatment efficacy: ultrasound-based vascular normalization
Vascular normalization, a novel therapeutic approach derived from anti-angiogenic therapy, is aimed at improving the tumor vasculature. In clinical trials, bevacizumab, a single anti-VEGF drug, has shown a modest response rate of 6.7% in patients with metastatic breast cancer [88]. However, when combined with chemotherapy, it significantly enhances progression-free survival and overall survival [89, 90]. Consequently, anti-VEGF therapy has been proposed to induce vascular “normalization” by decreasing tumor vascular density while restoring the structure and function of remaining vessels, thereby improving drug and oxygen delivery [91, 92]. Studies in patients with rectal cancer have confirmed this hypothesis by demonstrating a 40–50% decrease in vascular density with no significant change in FDG uptake, thus suggesting enhanced efficiency of the “normalized” vessels [93, 94].
The mechanism of vascular normalization involves pruning vessels, enhancing pericyte coverage, and strengthening vascular walls [95]. Extensive research has shown that vascular normalization is only a temporary therapeutic window during which the tumor vasculature undergoes pruning, strengthening, and decompression [96]. Notably, the tumor vasculature is not completely normalized, but abnormalities caused by signal dysregulation are partially corrected [12]. Anti-angiogenic drugs, such as bevacizumab, typically induce vascular normalization within 1–4 days, after which vascular degradation and increased tumor hypoxia occur [97, 98]. Controlling drug dosages is key to extending the normalization window. Preclinical studies have shown that lower doses have enhanced effectiveness in prolonging normalization and improving the tumor microenvironment [99–101]. By decreasing drug dosage and treatment frequency, the normalization window might be prolonged, and the adverse effects associated with high-dose VEGF inhibitors might be avoided [92]. Clinical studies have highlighted the need for biomarkers to identify patients who would benefit from bevacizumab treatment, given that only a subset of patients show prolonged survival or radiological relief.
Given these challenges, developing drug-independent strategies for vascular normalization is highly promising. Ultrasound-mediated MB cavitation increases shear stress and induces vasodilation, while regulating endothelial cell metabolism by elevating hydrogen peroxide, calcium ion flow, and ATP generation [19, 102, 103]. Studies in animal models have indicated that therapeutic ultrasound combined with C3F8 MBs induces a short-term increase in blood perfusion lasting approximately 30 minutes, whereas combined treatment with oxygen MBs extends this effect to 2–8 days, thereby decreasing HIF-1α and VEGF expression and regulating angiogenesis [18]. Additionally, low mechanical index (MI < 0.5) ultrasound can induce “sonoperfusion,” which enhances blood flow and dilates tumor vessels [104, 105]. This phenomenon is based on mild inflammatory reactions caused by low-intensity ultrasound cavitation, which lead to tumor vascular dilation and accelerated blood flow. This mechanical index, lower than conventional ultrasound (MI 1.0–1.3), achieves enhanced perfusion lasting more than 4 hours [18, 106–108]. Variations in ultrasound parameters further complicate vascular normalization, because MBs respond differently to stable or inertial cavitation [109, 110]. Lower peak negative pressures, such as 0.43 MPa, induce sonoperfusion, whereas higher values (1.65 MPa) cause inertial cavitation, which can inhibit tumor growth by disrupting blood vessels [105, 111].
Clinical trials have focused on monitoring vessel damage through ultrasound, and applications of ultrasound for vascular normalization remain limited. Combining ultrasound with piezoelectric materials might offer new strategies for vascular normalization. Preclinical studies have shown that low-intensity pulsed ultrasound (1 MHz, 1.0 W/cm2) combined with piezoelectric nanomaterials inhibits endothelial cell migration, increases pericyte coverage to 68%, and increases blood perfusion (861% of blank), thereby improving tumor hypoxia [112]. Researchers have also developed nanodroplets containing the extracellular domain of VEGF receptor 1 and CD93 ligand, which, after acoustic vaporization, release fragments that help clear VEGF and promote vascular normalization [113]. Future research should focus on optimizing ultrasound parameters, electrical stimulation, and tailoring treatments to different tumor types to develop more precise and effective vascular normalization therapies.
Notably, the selection between two mechanistically distinct strategies, vascular disruption and vascular normalization, must be carefully evaluated within specific pathological contexts. Vascular disruption is aimed primarily at rapidly decreasing tumor burden by destroying abnormal blood vessels, thereby starving the tumor. This approach might be particularly relevant in highly vascularized tumors such as HCC, which often progress asymptomatically and are frequently diagnosed in advanced stages, when surgical resection is no longer feasible. Although transarterial embolization can regionally suppress tumor growth by occluding major feeding arteries, it often fails to completely block the blood supply in multifocal HCC. In such cases, VDAs provide an alternative by selectively targeting established tumor vasculature. However, the acute disruption exacerbates hypoxia in residual tumor regions, thus upregulating hypoxia-inducible factors such as HIF-1α and enhancing VEGF expression, and potentially further aggravating vascular abnormality. Additionally, vascular disruption promotes an immunosuppressive microenvironment, characterized by elevated M2 macrophage polarization and PD-L1 expression, which contributes to tumor recurrence and metastasis [114, 115]. Therefore, this strategy often requires combination with subsequent treatments to eliminate surviving, aggressive tumor cells at the periphery. One promising approach is to combine VDAs with immunotherapeutic agents, which may not only counteract the immune suppression induced by VDAs but also promote immune activation against the surviving tumor cells [114].
In contrast, vascular normalization, which focuses on remodeling aberrant vasculature to improve the tumor microenvironment, serves as an adjuvant therapy to enhance the efficacy of chemotherapy or immunotherapy. This strategy enables fine-tuning of the TME, particularly in immunologically “cold” tumors such as breast cancer, which exhibit low baseline T cell infiltration and abundant immunosuppressive myeloid cells. Even in relatively immunoresponsive subtypes such as triple-negative breast cancer, monotherapy with PD-1/PD-L1 inhibitors yielded objective response rates of only 5.2%–18.5% in early trials. Abnormal tumor vasculature impairs perfusion and immune cell infiltration, exacerbates hypoxia, dampens cytotoxic T cell function, and recruits immunosuppressive cells such as MDSCs and Tregs. Hypoxia also stimulates the secretion of immunosuppressive cytokines and upregulates PD-1 on T cells. Low-dose anti-VEGFR2 antibody treatment has been found to induce vascular normalization, promote immune cell infiltration and activation, and stimulate osteopontin secretion by CD8⁺ T cells. OPN triggers TGF-β production by tumor cells and leads to PD-1 upregulation on immune cells. Combined low-dose VEGFR2 inhibition and anti-PD-1 therapy have shown promising tolerability and efficacy in patients with advanced TNBC.
Notably, the two strategies are not mutually exclusive, and their combination could yield synergistic anti-tumor outcomes. For example, although CA4-NP-induced vascular disruption decreases tumor burden, it often elevates VEGF expression, thus resulting in highly abnormal vasculature that impedes CD8⁺ T cell infiltration and compromises anti–PD-1 efficacy [106]. Bao et al. have sequentially applied vascular disruption and normalization and observed that CA4-NPs induced vascular collapse and hypoxia-mediated necrosis, thereby decreasing tumor burden, whereas subsequent DC101 (anti-VEGFR2) normalized the vasculature, alleviated hypoxia, and enhanced intratumoral CD8⁺ T cell infiltration [116]. This sequential approach rebalanced the CD8⁺ T cell–tumor burden ratio. On day 10 of treatment, the tumor inhibition rates were 47.0%, 25.3%, and 63.5% in the CA4-NP, DC101, and combination groups, respectively. With the addition of anti–PD-1 therapy, the inhibition rate reached 86.4%.
Improving treatment efficacy: ultrasound-based vasodilation
Vascular normalization plays a crucial role in enhancing therapeutic efficacy by restoring vascular function, thereby decreasing interstitial fluid pressure and improving blood perfusion. However, emerging evidence suggests that transiently increasing vascular permeability might also enhance treatment sensitivity. A notable example is nanoparticle-based drug delivery systems, which exploit the inherent structural defects in the tumor vasculature, such as defective endothelial cell alignment and intercellular gaps, thereby facilitating nanomedicine accumulation. Although the enhanced permeability and retention effect has been widely used, passive reliance on this phenomenon alone is often insufficient for effective nanoparticle penetration into tumors. Therefore, strategies aimed at further augmenting vascular permeability have considerable therapeutic potential.
Wang et al. have engineered ultrasound-responsive liposomes for targeted GSNO delivery, which induce vasodilation through vascular smooth muscle cells, and consequently enhance tumor perfusion and permeability, particularly in low-permeability tumors with denser vascular smooth muscle cells in more rigid vasculature [117]. Intratumoral vascular heterogeneity, characterized by immature central vessels and structured peripheral vasculature, has prompted important questions regarding regional variations in NO responsiveness. Therefore, a dual strategy was devised by combining NO-induced vasodilation in peripheral vessels with ultrasound-mediated ablation of central vessels to improve chemosensitization. Bellary et al. have further advanced this concept by demonstrating focused ultrasound-guided MB delivery of plasmids bearing inducible nitric oxide synthase sequences into the tumor vasculature, thus enabling sustained localized NO production via endothelial transfection [118]. This approach effectively addresses the spatial limitations of conventional NO delivery and offers precise spatiotemporal control within tumors.
Mild hyperthermia is another promising approach for enhancing vascular permeability by thermally expanding microvascular pores. Clinical studies have shown that combining hyperthermia with chemotherapy significantly improves local tumor control [119]. Xia et al. have demonstrated that laser-induced thermal effects promote localized vascular dilation and markedly increase chemotherapeutic drug accumulation in tumors [120]. Similarly, Xiang et al. have used ultrasound-mediated hyperthermia, which has superior tissue penetration, and observed post-sonication vascular expansion and an increase in average vessel diameter [121]. This approach not only increased intratumoral drug concentrations but also enhanced T-cell infiltration, thus suggesting a potential synergistic immunomodulatory effect.
Ultrasound-based tumor vasculature monitoring strategies
Therapeutic strategies targeting the tumor vasculature effectively inhibit tumor growth. The Response Evaluation Criteria in Solid Tumors (RECIST) criteria are used primarily to assess therapeutic effects and prognosis by measuring tumor volume changes and lymph node metastasis [122]. However, alterations in tumor size are often not measurable until several months post-treatment, and current clinical response criteria based solely on dimensional changes might be misleading [123]. Certain therapeutic strategies, such as anti-angiogenic therapy and the induction of vascular normalization, can exacerbate tumor aggressiveness and treatment resistance if they are over-administered or inadequately dosed [14, 124]. Angiogenesis, an early biological alteration in tumors, often precedes tumor growth and consequently is a valuable predictive biomarker for tumor prognosis. Additionally, monitoring the time window of vascular normalization is critical for optimal treatment timing [125]. Therefore, assessment of dynamic changes in the tumor vasculature is essential for effective tumor control. Ultrasound, a non-invasive, cost-effective, and real-time imaging technique, has been widely used in clinical trials to monitor the tumor vasculature (Table 1). Methods include Doppler ultrasound imaging, such as spectral Doppler, color Doppler, and power Doppler, which are limited to larger vessels; contrast-enhanced ultrasound, which can comprehensively evaluate microvascular structures and perfusion with diameters less than 200 μm; and UMI, which overcomes structural imaging limitations. Demand for high-resolution imaging has driven the emergence of advanced ultrasound techniques such as ultrasound localization microscopy and super-resolution ultrasound imaging, which enable non-invasive visualization of fine vascular structures. Consequently, ultrasound-based tumor vascular monitoring strategies have undergone rapid development [126] (Figure 6).
Figure 6 Advances in ultrasound-based monitoring strategies for the tumor vasculature.
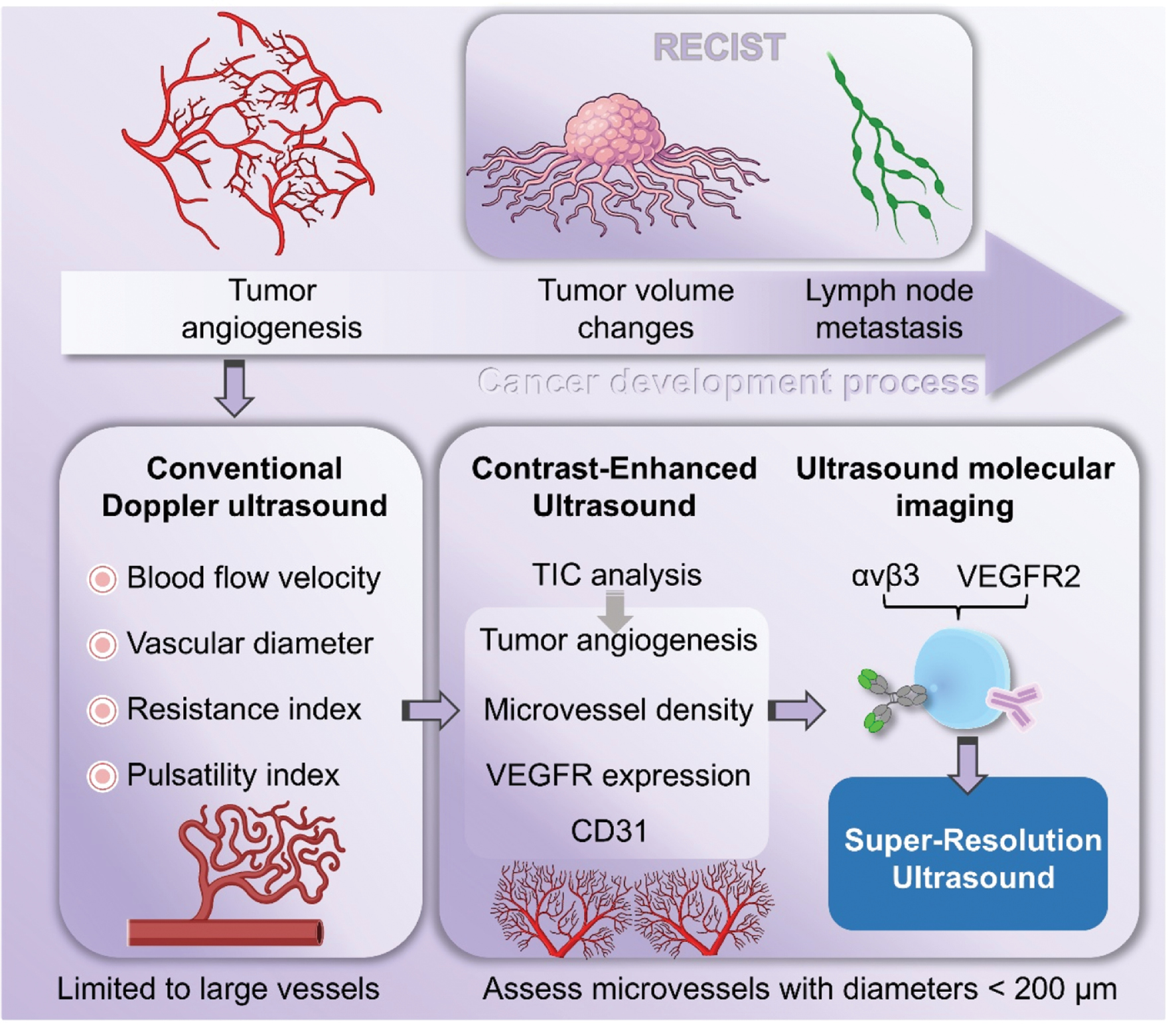
Table 1 Clinical Trials of Ultrasound-Based Tumor Vascular Monitoring
| Year Author | Modality | Rationale for Modality Selection | Disease | Key Metrics | Key Founding | Refs. |
|---|---|---|---|---|---|---|
| 1999 Bogers et al. | Contrast-enhanced 3D Power Doppler | Microvasculature imaging for deep pelvic organ | Prostate cancer | Sens: 85%, Spec: 80%, PPV: 92%, NPV: 67% | Contrast-enhanced 3D power Doppler improves accuracy in detecting prostate cancer | [176] |
| 2003 Görges et al. | High-Resolution B-mode and Power Doppler | Superficial location, cost-effective vascular assessment | Thyroid cancer | B-mode and Power Doppler: Sensitivity 90%, Specificity 82%, Accuracy 88% (Youden’s index = 0.72) | Provide a standardized, cost-effective US solution for cervical lesion differentiation in thyroid cancer follow-up, with specificity superior to MRI | [177] |
| 2013 Kabil Kucur et al. | Power Doppler | Transvaginal access for uterine vascular patterns | Endometrial polyps | Sens: 66.67%, Spec: 98.28%, PPV: 96.3%, NPV: 81.43% | IETA-defined vascular patterns are core to differentiating endometrial lesions; IOTA color score lacks discriminative value | [178] |
| Endometrial cancer | Sens: 42.86%, Spec: 91.11%, PPV: 27.27%, NPV: 95.35% | |||||
| Non-specific endometria | Sens: 81.25%, Spec: 89.23%, PPV: 78.79%, NPV: 90.62% | |||||
| Endometrial hyperplasia | Sens: 88.89%, Spec: 88.64%, PPV: 44.4%, NPV: 98.73% | |||||
| Submucosal fibroids | Sens: 80%, Spec: 100%, PPV: 100%, NPV: 97.75% | |||||
| 2014 Chen et al. | 3D Contrast-Enhanced Ultrasound | 3D tumor vascular architecture mapping | Breast tumors (benign vs. malignant) | Penetrating vessels: Specificity 88.6%, Sensitivity 35.1%, Accuracy 45.4% Roughness of marginal perfusion: Sensitivity 90.2%, Specificity 70.4%, Accuracy 85.3% Intratumoral perfusion pattern: Sensitivity 77.8%, Specificity 57.1%, Accuracy 73.5% Intratumoral vascular dilatation: Specificity 88.9%, Sensitivity 38.0%, Accuracy 48.8% |
3D-CEUS differ significantly between benign & malignant and non-invasively correlates with MVD/VEGF | [179] |
| 2015 Hoyt et al. | Dynamic Contrast-Enhanced Ultrasound | Real-time perfusion monitoring for therapy response | Breast cancer | Changes in perfusion parameters: IPK decreased by 14.8%, AUC decreased by 16.8% (P < 0.012); VR decreased by 26.1%, NB decreased by 27.5%, NV decreased by 23.9% (P ≈ 0.20) | Perfusion parameters predict chemotherapy response at 6 weeks, and baseline parameters correlate with residual cancer burden | [180] |
| 2012 Bezircioglu et al. | Transvaginal US and Doppler | Vascular indices evaluation alongside endometrial thickness | Endometrial pathology in breast cancer patients | Radial artery RI = 0.66 (AUC = 0.697 ± 0.076, Sensitivity 73.3%, Specificity 49.2%) Spiral artery PI = 0.52 (AUC = 0.338 ± 0.084, Sensitivity 73.3%, Specificity 12.5%) |
Doppler vascular indices (esp. spiral artery PI, uterine artery PI/RI) offer limited diagnostic value. Endometrial thickness via TVS remains the most effective assessment tool. | [181] |
Conventional doppler ultrasound
Doppler ultrasound enables non-invasive assessment of tumor angiogenesis by detecting hemodynamic parameters such as the pulsatility index (PI) and resistance index (RI) [127, 128]. Doppler ultrasound encompasses multiple modalities, such as spectral Doppler, color Doppler, and power Doppler. Spectral Doppler, including continuous-wave Doppler, is suitable for high-velocity blood flow analysis but cannot precisely localize flow velocity. Pulsed-wave Doppler offers better spatial resolution but diminished accuracy in distant flow measurements. Color Doppler provides intuitive visualization of flow direction and velocity; however, its accuracy diminishes at the Nyquist limit. Power Doppler achieves superior sensitivity for low-velocity flow and deeper structures, but lacks directional information [125]. To enhance capabilities by providing comprehensive spatial hemodynamic data, 3D power Doppler was developed. This method is particularly useful for evaluating overall tumor blood perfusion, for example, through the vascularization index, flow index, and vascularization-flow index in endometrial cancer [129]. Nevertheless, because conventional Doppler techniques remain limited in detecting flows below 1 cm/s, they have limited utility in imaging the tumor microvasculature.
To overcome sensitivity limitations, ultrafast Doppler technology has emerged as a major advancement. With plane-wave imaging and spatiotemporal filtering, flow detection sensitivity is enhanced more than 50-fold, and low-velocity flows as slow as 1 mm/s can be visualized with an in-plane resolution of 100 μm at 15 MHz [130]. Further innovation led to ultrafast Doppler tomography (UFD-T), which enables 3D high-resolution vascular imaging. UFD-T accurately delineates tumor vascular networks and local hemodynamics, and notably aids in monitoring of angiogenesis and responses to anti-angiogenic treatments such as vascular normalization. UFD-T offers considerable advantages: its high resolution and sensitivity can reveal typical tumor microvessel features, narrow diameters, and slow flow, and can clearly visualize vascular evolution from pre-existing skin vessels to new branches induced by tumor growth, culminating in ischemia as tumors exceed a critical size. It can track spatiotemporal changes in individual vessels, such as a distant vessel becoming a major supply artery. Quantitative analyses have shown that tumor vessel diameter follows an exponential distribution (R2 > 0.93), and >74% of vessels are <200 μm, in line with histological findings by Hashizume et al. (2000), thus confirming the biological relevance of these parameters [131]. Additionally, the finding that UFD-T’s vascular developmental stages strongly correlate with perfusion changes observed on dynamic contrast-enhanced ultrasound (DCE-US) has validated its role in monitoring tumor angiogenesis. Although conventional Doppler ultrasound is useful for assessing macroscale perfusion (e.g., in endometrial lesions), it has limited sensitivity and lacks strong correlation with VEGF expression or MVD.
Contrast-enhanced ultrasound
The visualization of microvascular blood flow is crucial for differentiating normal from abnormal tissue. In patients with glioma, increased tumor perfusion correlates with increased progression-free survival and overall survival [132]. CEUS using MB contrast agents enhances microvascular perfusion visualization, thereby improving tumor vascular imaging sensitivity [133].
Visualization of tumor microvascular perfusion
Imaging with MBs (1–10 μm in diameter), which remain intravascular, enhances blood flow and tissue perfusion imaging by exploiting their unique acoustic and nonlinear oscillation properties, and therefore is ideal for contrast enhancement in ultrasound imaging [134, 135]. This method improves dynamic tumor imaging and vascular depiction, and supports early tumor diagnosis and treatment monitoring. Furthermore, Caremani has proposed that the time taken for contrast agents to reach benign versus malignant lesions differs [136]. With dynamic MB imaging, the spatiotemporal characteristics of blood flow can be determined to enable early diagnosis and treatment assessment of the tumor vasculature [24, 31, 40].
Quantitative analysis of tumor microvascular perfusion and clinical applications
A key strength of CEUS is its quantitative analysis ability. Through generation of time-intensity curves (TICs), several perfusion parameters, such as peak intensity, rise time, and area under the curve (AUC), can be derived. These metrics closely correlate with tumor MVD and angiogenic activity, and provide critical information for personalized treatment strategies [137, 138]. The clinical utility of CEUS has been widely demonstrated. For example, lymph node metastasis, a hallmark of active tumor angiogenesis, is significantly positively correlated with six TIC parameters (P < 0.05), among which peak enhancement (r = 0.415, P = 0.020) and time to peak (TTP, r = 0.421, P = 0.018) also significantly correlate with CD31-labeled microvascular area. The perfusion patterns observed via CEUS align with characteristic pathological features of colorectal cancer angiogenesis. Although no significant correlation has been found between VEGFR1/VEGFR2 gene expression and TIC parameters, CEUS has core value as a minimally invasive, quantitative, and reproducible tool for monitoring angiogenesis. CEUS has been applied to evaluate pancreatic lesions: TIC-derived parameters have been used to differentiate pancreatic adenocarcinoma, chronic pancreatitis, and neuroendocrine tumors. Clinical studies in colorectal cancer indicating that TIC-derived parameters correlate with immune markers such as CD31 have offered new evidence that CEUS can be used to predict postoperative recurrence-free survival and overall survival [139]. However, compared with endothelial markers such as CD31 and CD34, CD105 enables more precise assessment of angiogenesis and microvessel density, although CE-EUS-derived perfusion parameters show no significant correlation with CD105, thus indicating both its potential and limitations in early tumor diagnosis and treatment response evaluation. In 2016, the FDA approved SonoVue for pediatric liver and bladder imaging, in a notable advancement in pediatric CEUS applications [140]. EFSUMB guidelines recommend dynamic CE-EUS for assessing the response of metastatic tumors to biologic therapies with an A-level endorsement [135].
Innovations in contrast-enhanced ultrasound technology
The development of novel contrast agents, such as nanoparticles, has enhanced both imaging resolution and targeting capabilities, and has positioned CEUS as a promising tool in precision medicine. Santiesteban et al. have developed a multimodal imaging platform using color-coded perfluorocarbon nanodroplets, which enables both ultrasound and photoacoustic imaging for multimodal analysis. This platform can target specific receptors, providing comprehensive anatomical and information for pathological tissues [141]. Additionally, the integration of artificial intelligence (AI) in image analysis has further advanced vascular imaging. Combining deep learning models with ultrasound images has yielded increased diagnostic accuracy [142]. In a chick embryo chorioallantoic membrane model of tumor angiogenesis, deep learning-based algorithms have successfully detected small-caliber blood vessels. The integration of ultrasound with AI has great promise as a research tool for monitoring tumor angiogenesis.
Ultrasound molecular imaging
Despite its enhanced capability for quantifying tumor perfusion, CEUS fundamentally relies on the non-specific hemodynamic distribution of MBs. This approach assesses angiogenesis through anatomic or functional changes yet falls short in capturing key molecular information during early angiogenic stages. Signaling molecules such as VEGF and integrin αvβ3 play central roles in regulating tumor microcirculation and tissue perfusion, as critical mediators of angiogenesis. To enable non-invasive and specific detection of these biomarkers at the molecular level, UMI has emerged as a cutting-edge technology. Molecular imaging using targeted contrast agents enables the visualization of cellular and molecular processes in vivo, and can provide early insights into potential changes before they manifest anatomically or physiologically [143]. Common techniques include single-photon emission computed tomography (SPECT) and positron emission tomography with radiotracer agents, magnetic resonance imaging (MRI)-based molecular imaging using magnetic nanoparticles, and UMI [144–146]. UMI notably strikes an optimal balance among resolution, sensitivity, cost-effectiveness, and clinical accessibility. Unlike conventional ultrasound using MBs, it uses targeted MBs modified with specific ligands that bind disease-specific biomarkers at lesion sites [147], thus enabling lesion localization and monitoring of molecular-level tumor vascular pathophysiological changes, and offering new opportunities for early tumor diagnosis and precise treatment.
Imaging signal processing techniques
UMI relies on the nonlinear response of ultrasound waves when they interact with contrast MBs. Because these MBs scatter ultrasound waves nonlinearly, their signals can be distinguished from linear waves reflected by surrounding tissues. This distinction enables precise imaging of MB contrast agents while avoiding interference from the surrounding tissue [133]. Advanced imaging techniques such as pulse inversion imaging, power modulation imaging, and contrast pulse sequencing are used to capture the MB signals without damaging the MBs themselves, thereby ensuring high image quality [148, 149]. Sensitive particle acoustic quantification quantifies signals from bound MBs by selectively destroying unbound, free MBs, thus enhancing imaging accuracy [150]. Additionally, the destruction-replenishment technique further increases imaging precision by destroying MBs after they bind targets and analyzing the signal differences before and after destruction [151].
Molecular-targeted vascular imaging strategies
Unlike traditional imaging methods, molecular imaging overcomes the limitations of anatomical imaging by achieving molecular-level precision [152]. This goal is accomplished by designing contrast agents that specifically target biomarkers associated with particular pathologies. A prominent target in UMI is VEGFR2, a transmembrane protein found on the surfaces of neovascular endothelial cells and a key marker for imaging angiogenesis (Table 2). BR55, a VEGFR2-targeted contrast agent commercially available from Bracco, was designed for imaging endothelial cells involved in angiogenesis [152]. Studies have demonstrated the safety and feasibility of using UMI to target VEGFR2 in patients with prostate cancer [153]. BR55 MBs have also demonstrated efficacy in diagnosing breast cancer and ovarian lesions, by enhancing ultrasound contrast in 93% of malignant breast lesions and 85% of malignant ovarian lesions [154]. Furthermore, recent advancements in dual-targeting strategies, combining multiple ligands such as VEGFR1 with follicle-stimulating hormone receptor, or VEGFR2 with αvβ3 integrin, have further increased the specificity of contrast agents and consequently enhanced the overall quality of molecular imaging [155].
Table 2 Ultrasound Molecular Imaging in Monitoring Tumor Angiogenesis
| Probe | Target | Application | Year | Modality | Key Metrics | Research Findings | Ref |
|---|---|---|---|---|---|---|---|
| BR55 | VEGFR2 | Prostate Cancer | 2017 | Ultrasound Molecular Imaging (iU22 scanner, C8-4v/C10-3v probes, MI ≤ 0.12; VueBox quantification) | 23 patients with radical prostatectomy: 52 malignant lesions, overall detection rate 50% 11 patients with optimized protocol: 28 malignant lesions, detection rate 68% Gleason 3+3 tumors most frequently missed |
Conducted exploratory Phase 0 study in humans; shows potential in detecting prostate lesions but has limitations such as difficulty detecting Gleason score 3+3 tumors. | [153] |
| BR55 | VEGFR2 | Breast Cancer | 2010 | Contrast-Specific Ultrasound Imaging (Siemens Sequoia 512, 15L8 transducer, CPS mode, MI = 0.25) | Tumors showed specific enhancement 10 min post-BR55 injection (circulating bubbles cleared) SonoVue (nontargeted) showed no tumor enhancement at 10 min |
Tumors were significantly contrasted with 10 minutes post-application due to the specific accumulation of targeted microbubbles on VEGFR2-expressing endothelial cells; SonoVue showed no enhancement after 10 minutes. | [182] |
| BR55 | VEGFR2 | Skin Squamous Cell Carcinoma | 2015 | VEGFR2-Targeted Ultrasound Imaging (Vevo2100, MS-250 transducer, MI = 0.03; Imalytics analysis) | Day 4 post-anti-VEGF therapy: BR55 bound signal (0.04 au) vs. control (0.14 au), P = 0.0058 Day 14: VEGFR2-positive area fraction 0.8% (treated) vs. 1.9% (control), P = 0.0079 |
BR55 used for VEGFR2 evaluation showed significant differences between treatment and control groups as early as day 4 of treatment, unlike non-targeting microbubbles at most time points. | [183] |
| BR55 | VEGFR2 | Breast Cancer | 2020 | Ultrasound Molecular Imaging (iU22 scanner, L12–5 transducer, MI = 0.08 for contrast mode; VueBox quantification) | Early response: VEGFR2 signal decreased by 25% at 12 h (tumor size no change), 80% at 72 h Anatomical parameters decreased by ~40% at 72 h Functional parameter decreased by 32% at 24 h, 48% at 72 h IHC confirmed VEGFR2 expression trend consistent with USMI |
Significant differences in VEGFR2 expression were observed 12 hours after administration, whereas tumor size changes appeared at 24 hours. After 72 hours of treatment, VEGFR2 expression decreased by 80%, while anatomical parameters decreased by about 40% | [184] |
| microbubbles | VEGFR2 | Tumor Angiogenesis (Angiosarcoma/Glioma) | 2008 | Targeted Contrast-Enhanced US (VisualSonics Vevo 770, 40-MHz transducer, MI = 0.14; destruction-replenishment protocol) | video intensity difference: 34.4 (angiosarcoma) &; 28.4 (glioma) vs. 2 (normal muscle), P < 0.001 Reproducibility: CV = 11.1% ± 3.8, intraclass correlation = 0.88 |
VEGFR2-targeted microbubbles specifically bound to tumor blood vessels, enabling noninvasive imaging of tumor angiogenesis in murine models. Signal intensity was significantly higher with targeted versus control microbubbles and was reduced after VEGFR2 blockade. | [155] |
| microbubbles | VEGFR2 | Liver Allograft Fibrosis (LAF) | 2021 | VEGFR2-Targeted US Molecular Imaging (GE Logiq E9, ML9 probe, MI = 0.13; SWE elastography for comparison) | Quantitative NID (normalized intensity difference) correlated with Metavir score (R2 = 0.77) vs. SWE (R2 = 0.35) NID correlated with VEGFR2 IOD (R2 = 0.78) vs. SWE (R2 = 0.49) Early fibrosis (F ≤ 1): ROC AUC = 0.99 (SWE = 0.69, P = 0.01) Peak NID (53.3 ± 10.2%) at 7 d, consistent with pathological fibrosis peak |
VEGFR2-targeted ultrasound molecular imaging (USMI) enabled noninvasive, specific detection of angiogenesis in a rat model of liver allograft fibrosis (LAF). This method demonstrated stronger imaging signals in fibrotic livers compared to controls and showed higher correlation with histological fibrosis and VEGFR2 expression than conventional ultrasound elastography, which was significantly influenced by inflammation. The targeted microbubbles proved safe with no observed toxicity. | [185] |
Multimodal integration for tumor vascular monitoring
Substantial progress has been made in multimodal detection by integrating UMI with other imaging modalities such as MRI, CT, and fluorescence imaging [156–158]. The combination of MBs with these imaging techniques has advanced the resolution and accuracy of tumor vascular monitoring. For example, the development of 3D UMI, paired with matrix transducers for multi-frame frequency data acquisition, has increased the quality of tumor vascular multimodal imaging, particularly in the detection of VEGFR2 expression. Ultrasound localization microscopy (ULM), a rapidly advancing technology that overcomes the diffraction limits of ultrasound resolution, has also been crucial. ULM can distinguish microvessels and track individual MBs to gather flow speed information. Preclinical studies exploring the combination of UMI with ULM have achieved super-resolution vascular imaging with a resolution of 28.8 μm, and enabled the co-localization of VEGFR2-targeted MB signals [159]. These developments have provided a robust theoretical and practical foundation for the multimodal application of UMI in tumor detection, which might enhance diagnostic accuracy and therapeutic outcomes. This model represents a promising direction for the future of UMI in tumor detection and personalized treatment evaluation.
Super-resolution ultrasound imaging
Ultrasound imaging enhances sensitivity to unresolved microvasculature through the use of contrast agents. However, similarly to MRI, CT, or SPECT, it remains constrained by spatial resolution limitations. Conventional imaging modalities cannot resolve microvasculature that is highly sensitive to anti-angiogenic therapies. The ability to visualize and analyze structural and functional characteristics of the microvascular system is essential for assessing and monitoring vascular responses to treatment. Consequently, super-resolution ultrasound (SR-US) imaging was developed. SR-US encompasses a range of techniques using high-frequency sound waves to resolve structures spaced closer than the conventional diffraction limit (approximately half the wavelength), including ULM, super-resolution fluctuation imaging, structured illumination, and near-field methods. The concept of SR-US has been explored for decades [160], and a key breakthrough occurred in 2010 with the introduction of ULM based on ultrasound contrast agents (MBs) and ultrahigh-frame-rate scanners [161]. Analogously to fluorescence-based super-resolution microscopy, ULM replaces optical with acoustic signals to surpass the ultrasonic diffraction limit. Its core principle involves continuous tracking and precise localization of flowing MBs; by compiling spatial coordinates from millions of individual events, microvascular images surpassing wavelength-limited resolution can be reconstructed [162, 163]. In 2013, ULM achieved subwavelength resolution in vitro, by distinguishing microvessels spaced less than half a wavelength apart [164]. Subsequent studies have shown that SR-US can visualize structural changes in tumor microvasculature after bevacizumab therapy [165]. In practice, the resolution of SR-US is no longer constrained by acoustic wavelength but depends primarily on MB localization accuracy and the system point spread function. Under ideal conditions, ULM can achieve in-plane resolutions of 10–20 μm, and approximately 28.8 μm in small animal models [112, 152].
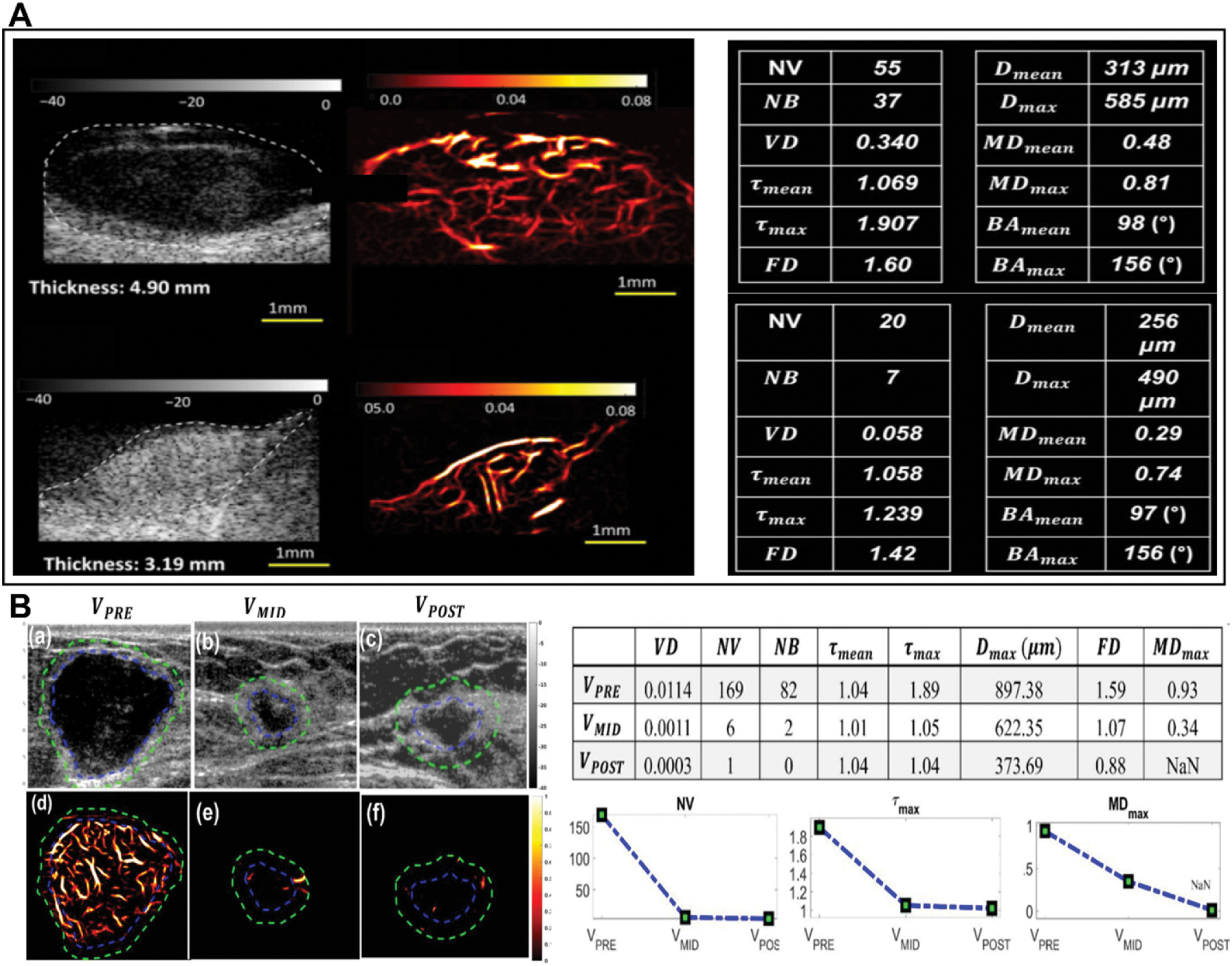
Two primary factors limiting SR-US are MB localization uncertainty and localization density. To enable single-MB tracking, contrast agent concentrations must often be decreased; consequently, thousands of images must be acquired to compensate for weak scattered signals. Real-time SR-US image reconstruction is therefore highly challenging [125]. Additionally, the stability and biocompatibility of MBs in vivo are critical considerations. Factors such as susceptibility to acoustic destruction, rapid clearance rates, and low targeting efficiency might compromise imaging performance. In certain anatomical sites, such as ocular choroidal melanoma, potential risks of vascular injury induced by MBs also warrant attention [166]. To address contrast-related limitations, recent advances have focused on contrast-free ultrasound microvascular imaging. These techniques integrate morphological filtering and vascular enhancement algorithms to visualize tumor microvessels as small as 150 μm and to extract vascular morphological features as novel biomarkers for cancer diagnosis [167, 168]. For example, a clinical study differentiating choroidal tumors has identified six high-definition microvascular imaging (HDMI) biomarkers—number of vessel segments (NV, p = 0.003), number of branch points (NB, p = 0.003), vessel density (VD, p = 0.03), maximum tortuosity (τₘₐₓ, p = 0.001), microvessel fractal dimension (mvFD, p = 0.002), and maximum diameter (Dₘₐₓ, p = 0.003)—that exhibited significant differences between malignant melanomas and benign nevi [169] (Figure 7A). Furthermore, NV, NB, FD, and mean/maximum tortuosity have also shown discriminative power between benign and malignant liver lesions [169]. A recent study has highlighted the utility of quantitative HDMI (qHDMI) for evaluating neoadjuvant chemotherapy response in patients with breast cancer. qHDMI biomarkers capturing tumor vascular morphology detected response trends within weeks of treatment initiation, and significant differences were found between responders and non-responders. For example, six key biomarkers—VD (p = 0.023), maximum tortuosity (τₘₐₓ, p = 0.049), maximum diameter (Dₘₐₓ, p = 0.002), FD (p = 0.002), mean Murray’s deviation (MDₘₑₐₙ, p = 0.034), and maximum Murray’s deviation (MDₘₐₓ, p = 0.022)—exhibited distinctly different trends throughout the treatment course between groups [170] (Figure 7B). Future studies may involve larger patient cohorts with more longitudinal time points to enhance statistical robustness, as well as volumetric microvascular imaging to enable comprehensive analysis of the tumor microvasculature for predictive modeling.
Figure 7 Advances in super-resolution ultrasound (SRUS) imaging technology. (A) High-definition microvascular imaging (HDMI) for differentiating choroidal tumors in humans in 2024. Comparison of B-mode and HDMI images of choroidal melanoma and hemangioma, emphasizing enhanced vascular visualization for tumor characterization (Adusei SA et al. (2024). Cancers (Basel) 16(2):395. doi: 10.3390/cancers16020395. Licensed under CC BY 4.0) [169]. (B) Quantitative HDMI (qHDMI) images and biomarkers from a 36-year-old patient with breast cancer before, during, and after chemotherapy, showing dynamic microvascular changes in response to therapy (Sabeti S et al. (2025). Breast Cancer Res 27(1):24. doi: 10.1186/s13058-025-01978-y. Licensed under CC BY 4.0) [170].
Clinical translation and future challenges
Ultrasound-based tumor vascular targeting exemplifies the transformative potential of multidisciplinary modalities. Integration of expertise from acoustic physics, molecular oncology, and biomedical imaging has overcome the constraints of conventional unimodal therapies by achieving mechanistic synergy. Ultrasound’s mechanical, cavitation, and thermal effects enable spatiotemporally controlled interventions, with applications as diverse as molecular-scale drug targeting and macroscale tumor ablation. Advanced monitoring modalities, super-resolution hemodynamic imaging, and molecular contrast-enhanced ultrasound facilitate real-time, quantitative vascular phenotyping, thereby enabling precision-guided therapeutic window optimization. Critically, ultrasound-driven vascular modulation has led to a paradigm shift in immuno-oncology.
Several clinically translated products have achieved notable vascular effects. The Edison system by HistoSonics has innovated controlled acoustic cavitation by enabling tissue destruction through non–thermal mechanical effects, under ultrasound real–time visualization guidance. Clinical data have indicated that the Edison system selectively preserves larger vessels in the ablation area, thus significantly decreasing intraoperative bleeding risk (NCT04572633 and NCT04573881). In 2023, the device was granted breakthrough device designation by the FDA (DEN220087). The HOPE4LIVER clinical trial has reported a technical success rate of 95% (42 of 44) in treating primary and metastatic liver tumors [171].
Additionally, the JC series HIFU devices by Haifu Medical, using phased–array focusing technology, enable millimeter–precise positioning. In clinical studies, the devices’ thermal ablation effects have been shown to severely damage tumor vessels, particularly immature vessels with a diameter below 2 millimeters [172]. The devices also effectively inhibit tumor proliferation, invasion, and metastasis. This technology has been demonstrated to induce a strong immune response in primary breast cancer lesions (100% vs 64% in the control group), manifesting as significant expansion of cytotoxic T lymphocyte and natural killer cell populations in the axillary lymph nodes [173]. A novel portable ultrasound–guided HIFU system is currently under development [174].
In ultrasound–based vascular monitoring, the combination of ultrasound and molecular imaging for early and high–precision imaging is expected to be the next mainstream trend in translation. Building on the success of its conventional ultrasound contrast agent SonoVue®, Bracco has advanced its targeted agent BR55 into Phase II clinical trials for multiple cancers, including prostate and ovarian cancers. (CTR20220634, NCT03486327, and NCT04248153). This technology has marked a shift from ultrasound anatomical imaging to functional–molecular imaging, by providing a real–time efficacy assessment tool for individualized anti–angiogenic therapy.
These technological advances demonstrate the growing clinical relevance of ultrasound in cancer therapy. The ability of ultrasound to target blood vessels and the tumor microenvironment has opened opportunities for better treatment delivery, higher precision in imaging, and enhanced drug efficacy, thus facilitating more effective clinical interventions. However, despite these promising developments, several challenges remain in translating ultrasound-based vascular targeting technologies into widespread clinical practice. A major challenge lies in the influence of ultrasound parameters (e.g., frequency, acoustic pressure, and pulse width) on the acoustic cavitation effects and subsequent biological responses, thus hindering treatment reproducibility and consistency. The lack of standardized protocols across devices and treatment regimens has further impeded multicenter studies and clinical use. Additionally, physical limitations in penetration depth required for imaging and treating deep-seated tumors necessitate systematic optimization of beam characteristics and tissue interactions. Moreover, the complexity of ultrasound-based treatments, compounded by challenges including skull attenuation in brain tumor applications and the high costs associated with advanced equipment, poses challenges to their broader use. For example, although UMI has shown promise, its limitations in imaging depth (particularly in transcranial or abdominal imaging), need for real-time monitoring with high temporal resolution, and technical intricacies have restricted its accessibility in certain settings.
In the future, another crucial aspect requiring in-depth evaluation is treatment safety. Although the violent oscillation or collapse (cavitation) of MBs under acoustic fields enhances vascular permeability, it can also cause microvascular damage, endothelial erosion, and even microthrombosis, thus potentially leading to thromboembolic risks. Off-target cavitation effects also warrant caution, particularly in highly perfused or fragile tissues, in which inappropriate acoustic exposure could potentially result in hemorrhage or tissue injury. Therefore, advancing therapeutic ultrasound and molecular imaging applications requires integrated consideration of acoustic parameters, MB dosage, and individual vascular anatomy, underpinned by rigorous safety assessment frameworks. The development of real-world evidence through multi-center international studies would help address current gaps in clinical knowledge. Collaborations such as the Focused Ultrasound Foundation (FUSF) aim to create large, diverse databases to better understand ultrasound treatment outcomes across various demographics and tumor types. Furthermore, early cancer signals, such as trace tumor methylation in the blood, can be detected with circulating tumor DNA methylation multi–cancer screening technologies, which can identify minimal traces of tumor methylation in the blood as many as 4 years before conventional clinical diagnosis [175]. The Guardant360 CDx assay (Guardant Health; FDA-approved PMA P200010, 2020) may be integrated with ultrasound-derived parameters to enable dynamic optimization of therapeutic windows. The integration of AI with ultrasound systems holds promise for next-generation oncology tools, particularly in advancing image-guided therapeutic strategies. A major milestone was achieved in 2020 with the FDA approval of Caption Guidance, the first AI-assisted ultrasound diagnostic software (DEN190040), a breakthrough that has paved the way to more personalized and precise treatment plans. As molecular ultrasound imaging-guided therapies, nanotechnology, and AI algorithms continue to evolve, ultrasound technology is poised to play an increasingly essential role in precision medicine. These innovations are expected to enhance the development of targeted therapies, particularly in oncology, by improving the accuracy and personalization of tumor treatments. The integration of AI with ultrasound systems promises to enable next-generation oncologic tools. Caption Guidance has provided a foundation for standardized image acquisition and interpretation to support larger clinical validation studies. With continued advances in UMI-guided therapy, nanotechnology, and AI algorithms, the role of ultrasound in precision oncology is expected to expand. Ultimately, the clinical utility and cost-effectiveness of these technologies must be validated through large prospective trials in diverse populations to facilitate their transition from technical platforms to routine clinical use, thereby advancing more precise and personalized cancer treatment.
Data availability statement
Data sharing is not applicable, because no new data were created or analyzed in this study.
Ethics statement
No direct interactions with human or animal subjects were involved. Therefore, ethical approval and informed consent were not required.
Author contributions
LL: Writing—review & editing, Writing—original draft, Conceptualization, Investigation, Methodology. YX: Writing—review & editing, Writing—original draft, Investigation, Conceptualization, Methodology. MD: Writing, review & editing, Supervision, Resources, Funding acquisition. ZC: Writing—review & editing, Supervision, Resources, Funding acquisition, Project administration. All authors read and approved the final manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (82272028, 81971621, and 82102087), the Key R&D Program of Hunan Province (2021SK2035), the Natural Science Foundation of Hunan Province (2022JJ30039 and 2022JJ40392), the Natural Science Foundation of Guangdong Province (2021A1515011177), and the Project of Science and Technology Innovation of Hunan Province (2021SK51807).
Acknowledgments
Not applicable.
Conflict of interest
The authors declare that there are no conflicts of interest.
Graphical abstract
Highlights
- US enables multi-mechanism modulation via anti-angiogenesis and vessel disruption.
- It achieves hemodynamic normalization through vasodilation for increased perfusion.
- Advanced US imaging provides real-time monitoring of tumor vascular alterations.
- Theranostic integration enables vascular intervention and treatment assessment.
In brief
This review presents ultrasound as a multi-effect theranostic platform that enables dynamic tumor vascular intervention through mechanisms including angiogenesis suppression, vessel disruption, and hemodynamic normalization. This versatile approach overcomes limitations of single-mechanism strategies by integrating real-time monitoring of vascular alterations via contrast-enhanced and molecular ultrasound imaging. Despite its therapeutic promise, clinical translation faces parameter optimization, standardization, and validation hurdles across diverse tumor types.
References
- Koos B, Kamali-Moghaddam M, David L, Sobrinho-Simões M, Dimberg A, et al. Next-generation pathology–surveillance of tumor microecology. J Mol Biol 2015;427(11):2013-22. [PMID: 25725260 DOI: 10.1016/j.jmb.2015.02.017]
- Hanahan D, Weinberg R. Hallmarks of cancer: the next generation. Cell 2011;144(5):646-74. [PMID: 21376230 DOI: 10.1016/j.cell.2011.02.013]
- Huang Z. Roles of main pro- and anti-angiogenic factors in tumor angiogenesis. World J Gastroenterol 2004;10(4):463. [PMID: 14966899 DOI: 10.3748/wjg.v10.i4.463]
- Al-Ostoot FH, Salah S, Khamees HA, Khanum SA. Tumor angiogenesis: current challenges and therapeutic opportunities. Cancer Treat Res Commun 2021;28:100422. [PMID: 34147821 DOI: 10.1016/j.ctarc.2021.100422]
- Mazzone M, Dettori D, de Oliveira RL, Loges S, Schmidt T, et al. Heterozygous deficiency of PHD2 restores tumor oxygenation and inhibits metastasis via endothelial normalization. Cell 2009;136(5):839-51. [PMID: 19217150 DOI: 10.1016/j.cell.2009.01.020]
- De Palma M, Biziato D, Petrova TV. Microenvironmental regulation of tumour angiogenesis. Nat Rev Cancer 2017;17(8):457-74. [PMID: 28706266 DOI: 10.1038/nrc.2017.51]
- Giaccia AJ, Simon MC, Johnson R. The biology of hypoxia: the role of oxygen sensing in development, normal function, and disease. Genes Dev 2004;18(18):2183-94. [PMID: 15371333 DOI: 10.1101/gad.1243304]
- De Bock K, Cauwenberghs S, Carmeliet P. Vessel abnormalization: another hallmark of cancer? Molecular mechanisms and therapeutic implications. Curr Opin Genet Dev 2011;21(1):73-9. [PMID: 21106363 DOI: 10.1016/j.gde.2010.10.008]
- Goel S, Duda DG, Xu L, Munn LL, Boucher Y, et al. Normalization of the vasculature for treatment of cancer and other diseases. Physiol Rev 2011;91(3):1071-121. [PMID: 21742796 DOI: 10.1152/physrev.00038.2010]
- Jain RK. Normalizing tumor microenvironment to treat cancer: bench to bedside to biomarkers. J Clin Oncol 2013;31(17):2205-18. [PMID: 23669226 DOI: 10.1200/jco.2012.46.3653]
- Sivakumar B, Harry LE, Paleolog EM. Modulating angiogenesis: more vs less. JAMA 2004;292(8):972. [PMID: 15328330 DOI: 10.1001/jama.292.8.972]
- Guelfi S, Hodivala-Dilke K, Bergers G. Targeting the tumour vasculature: from vessel destruction to promotion. Nat Rev Cancer 2024;24(10):655-75. [PMID: 39210063 DOI: 10.1038/s41568-024-00736-0]
- Jain R. Antiangiogenesis strategies revisited: from starving tumors to alleviating hypoxia. Cancer Cell 2014;26(5):605-22. [PMID: 25517747 DOI: 10.1016/j.ccell.2014.10.006]
- Yang T, Xiao H, Liu X, Wang Z, Zhang Q, et al. Vascular normalization: a new window opened for cancer therapies. Front Oncol 2021;11:719836. [PMID: 34476218 DOI: 10.3389/fonc.2021.719836]
- Hinnen P, Eskens FALM. Vascular disrupting agents in clinical development. Br J Cancer 2007;96(8):1159-65. [PMID: 17375046 DOI: 10.1038/sj.bjc.6603694]
- Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med 1971;285(21):1182-6. [PMID: 4938153 DOI: 10.1056/nejm197111182852108]
- Pellow C, Jafari Sojahrood A, Zhao X, Kolios MC, Exner AA, et al. Synchronous intravital imaging and cavitation monitoring of antivascular focused ultrasound in tumor microvasculature using monodisperse low boiling point nanodroplets. ACS Nano 2023;18(1):410-27. [PMID: 38147452 DOI: 10.1021/acsnano.3c07711]
- Ho YJ, Chu SW, Liao EC, Fan CH, Chan HL, et al. Normalization of tumor vasculature by oxygen microbubbles with ultrasound. Theranostics 2019;9(24):7370-83. [PMID: 31695774 DOI: 10.7150/thno.37750]
- Belcik JT, Davidson BP, Xie A, Wu MD, Yadava M, et al. Augmentation of muscle blood flow by ultrasound cavitation is mediated by ATP and purinergic signaling. Circulation 2017;135(13):1240-52. [PMID: 28174191 DOI: 10.1161/circulationaha.116.024826]
- Padilla F, Brenner J, Prada F, Klibanov AL. Theranostics in the vasculature: bioeffects of ultrasound and microbubbles to induce vascular shutdown. Theranostics 2023;13(12):4079-101. [PMID: 37554276 DOI: 10.7150/thno.70372]
- Wang J, Lv F, Fei X, Cui Q, Wang L, et al. Study on the characteristics of contrast-enhanced ultrasound and its utility in assessing the microvessel density in ovarian tumors or tumor-like lesions. Int J Biol Sci 2011;7(5):600-6. [PMID: 21614152 DOI: 10.7150/ijbs.7.600]
- Pysz MA, Guracar I, Foygel K, Tian L, Willmann JK. Quantitative assessment of tumor angiogenesis using real-time motion-compensated contrast-enhanced ultrasound imaging. Angiogenesis 2012;15(3):433-42. [PMID: 22535383 DOI: 10.1007/s10456-012-9271-3]
- Yin J, Dong F, An J, Guo T, Cheng H, et al. Pattern recognition of microcirculation with super-resolution ultrasound imaging provides markers for early tumor response to anti-angiogenic therapy. Theranostics 2024;14(3):1312-24. [PMID: 38323316 DOI: 10.7150/thno.89306]
- Rao SR, Shelton SE, Dayton PA. The “fingerprint” of cancer extends beyond solid tumor boundaries: assessment with a novel ultrasound imaging approach. IEEE Trans Biomed Eng 2016;63(5):1082-6. [PMID: 26394410 DOI: 10.1109/TBME.2015.2479590]
- Kaneko OF, Willmann JK. Ultrasound for molecular imaging and therapy in cancer. Quant Imaging Med Surg 2012;2(2):87-97. [PMID: 23061039 DOI: 10.3978/j.issn.2223-4292.2012.06.06]
- Tian L, Goldstein A, Wang H, Ching Lo H, Sun Kim I, et al. Mutual regulation of tumour vessel normalization and immunostimulatory reprogramming. Nature 2017;544(7649):250-4. [PMID: 28371798 DOI: 10.1038/nature21724]
- Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases. Nature 2000;407(6801):249-57. [PMID: 11001068 DOI: 10.1038/35025220]
- Hashizume H, Falcón BL, Kuroda T, Baluk P, Coxon A, et al. Complementary actions of inhibitors of angiopoietin-2 and VEGF on tumor angiogenesis and growth. Cancer Res 2010;70(6):2213-23. [PMID: 20197469 DOI: 10.1158/0008-5472.can-09-1977]
- Zhu D, Li Y, Zhang Z, Xue Z, Hua Z, et al. Recent advances of nanotechnology-based tumor vessel-targeting strategies. J Nanobiotechnol 2021;19(1):435. [PMID: 34930293 DOI: 10.1186/s12951-021-01190-y]
- Cooney MM, van Heeckeren W, Bhakta S, Ortiz J, Remick SC. Drug insight: vascular disrupting agents and angiogenesis–novel approaches for drug delivery. Nat Clin Pract Oncol 2006;3(12):682-92. [PMID: 17139319 DOI: 10.1038/ncponc0663]
- Davis GE, Senger DR. Endothelial extracellular matrix: biosynthesis, remodeling, and functions during vascular morphogenesis and neovessel stabilization. Circ Res 2005;97(11):1093-107. [PMID: 16306453 DOI: 10.1161/01.res.0000191547.64391.e3]
- Reymond N, d’Água BB, Ridley AJ. Crossing the endothelial barrier during metastasis. Nat Rev Cancer 2013;13(12):858-70. [PMID: 24263189 DOI: 10.1038/nrc3628]
- Munn LL, Jain RK. Vascular regulation of antitumor immunity. Science 2019;365(6453):544-5. [PMID: 31395771 DOI: 10.1126/science.aaw7875]
- Vasudev NS, Reynolds AR. Anti-angiogenic therapy for cancer: current progress, unresolved questions and future directions. Angiogenesis 2014;17(3):471-94. [PMID: 24482243 DOI: 10.1007/s10456-014-9420-y]
- Wong PP, Bodrug N, Hodivala-Dilke K. Exploring novel methods for modulating tumor blood vessels in cancer treatment. Curr Biol 2016;26(21):R1161-6. [PMID: 27825457 DOI: 10.1016/j.cub.2016.09.043]
- Wong PP, Demircioglu F, Ghazaly E, Alrawashdeh W, Stratford M, et al. Dual-action combination therapy enhances angiogenesis while reducing tumor growth and spread. Cancer Cell 2015;27(1):123-37. [PMID: 25584895 DOI: 10.1016/j.ccell.2014.10.015]
- Tannock IF. Population kinetics of carcinoma cells, capillary endothelial cells, and fibroblasts in a transplanted mouse mammary tumor. Cancer Res 1970;30(10):2470-6. [PMID: 4097429]
- Gray LH, Conger AD, Ebert M, Hornsey S, Scott OC. The concentration of oxygen dissolved in tissues at the time of irradiation as a factor in radiotherapy. Br J Radiol 1953;26(312):638-48. [PMID: 13106296 DOI: 10.1259/0007-1285-26-312-638]
- Suwa T, Kobayashi M, Nam JM, Harada H. Tumor microenvironment and radioresistance. Exp Mol Med 2021;53(6):1029-35. [PMID: 34135469 DOI: 10.1038/s12276-021-00640-9]
- Pan Y, Liu L, Mou X, Cai Y. Nanomedicine strategies in conquering and utilizing the cancer hypoxia environment. ACS Nano 2023;17(21):20875-924. [PMID: 37871328 DOI: 10.1021/acsnano.3c07763]
- Pinzón-Daza ML, Cuellar-Saenz Y, Nualart F, Ondo-Mendez A, Del Riesgo L, Castillo-Rivera F, et al. Oxidative stress promotes doxorubicin-induced Pgp and BCRP expression in colon cancer cells under hypoxic conditions. J Cell Biochem 2017;118(7):1868-78. [PMID: 28106284 DOI: 10.1002/jcb.25890]
- Lv Y, Zhao S, Han J, Zheng L, Yang Z, Zhao L. Hypoxia-inducible factor-1α induces multidrug resistance protein in colon cancer. Onco Targets Ther 2015;8:1941-8. [PMID: 26251616 DOI: 10.2147/OTT.S82835]
- Mohammadi M, Aghanajafi C, Soltani M, Raahemifar K. Numerical investigation on the anti-angiogenic therapy-induced normalization in solid tumors. Pharmaceutics 2022;14(2):363. [PMID: 35214095 DOI: 10.3390/pharmaceutics14020363]
- Mpekris F, Voutouri C, Baish JW, Duda DG, Munn LL, et al. Combining microenvironment normalization strategies to improve cancer immunotherapy. Proc Natl Acad Sci U S A 2020;117(7):3728-37. [PMID: 32015113 DOI: 10.1073/pnas.1919764117]
- Viallard C, Audiger C, Popovic N, Akla N, Lanthier K, et al. BMP9 signaling promotes the normalization of tumor blood vessels. Oncogene 2020;39(14):2996-3014. [PMID: 32042114 DOI: 10.1038/s41388-020-1200-0]
- Roma-Rodrigues C, Mendes R, Baptista PV, Fernandes AR. Targeting tumor microenvironment for cancer therapy. Int J Mol Sci 2019;20(4):840. [PMID: 30781344 DOI: 10.3390/ijms20040840]
- Fukumura D, Kloepper J, Amoozgar Z, Duda DG, Jain RK. Enhancing cancer immunotherapy using antiangiogenics: opportunities and challenges. Nat Rev Clin Oncol 2018;15(5):325-40. [PMID: 29508855 DOI: 10.1038/nrclinonc.2018.29]
- Khan KA, Kerbel RS. Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat Rev Clin Oncol 2018;15(5):310-24. [PMID: 29434333 DOI: 10.1038/nrclinonc.2018.9]
- Kashyap AS, Schmittnaegel M, Rigamonti N, Pais-Ferreira D, Mueller P, et al. Optimized antiangiogenic reprogramming of the tumor microenvironment potentiates CD40 immunotherapy. Proc Natl Acad Sci USA 2020;117(1):541-51. [PMID: 31889004 DOI: 10.1073/pnas.1902145116]
- Ma S, Pradeep S, Hu W, Zhang D, Coleman R, et al. The role of tumor microenvironment in resistance to anti-angiogenic therapy. F1000Res 2018;7:326. [PMID: 29560266 DOI: 10.12688/f1000research.11771.1]
- Meadows KL, Hurwitz HI. Anti-VEGF therapies in the clinic. Cold Spring Harb Perspect Med 2012;2(10):a006577. [PMID: 23028128 DOI: 10.1101/cshperspect.a006577]
- Zarrin B, Zarifi F, Vaseghi G, Javanmard SH. Acquired tumor resistance to antiangiogenic therapy: mechanisms at a glance. J Res Med Sci 2017;22(1):117. [PMID: 29184575 DOI: 10.4103/jrms.JRMS_182_17]
- Pinto MP, Sotomayor P, Carrasco-Avino G, Corvalan AH, Owen GI. Escaping antiangiogenic therapy: strategies employed by cancer cells. Int J Mol Sci 2016;17(9):1489. [PMID: 27608016 DOI: 10.3390/ijms17091489]
- Liu Y, Liu X, Cui Y, Yuan W. Ultrasound for microalgal cell disruption and product extraction: a review. Ultrason Sonochem 2022;87:106054. [PMID: 35688121 DOI: 10.1016/j.ultsonch.2022.106054]
- Miller DL, Dou C. Induction of apoptosis in sonoporation and ultrasonic gene transfer. Ultrasound Med Biol 2009;35(1):144-54. [PMID: 18723272 DOI: 10.1016/j.ultrasmedbio.2008.06.007]
- Sitta J, Howard CM. Applications of ultrasound-mediated drug delivery and gene therapy. Int J Mol Sci 2021;22(21):11491. [PMID: 34768922 DOI: 10.3390/ijms222111491]
- Wu Y, Sun T, Tang J, Liu Y, Li F. Ultrasound-targeted microbubble destruction enhances the antitumor efficacy of doxorubicin in a mouse hepatocellular carcinoma model. Ultrasound Med Biol. 2020;46(3):679-89. [PMID: 31882167 DOI: 10.1016/j.ultrasmedbio.2019.09.017]
- Liu H, Li X, Chen Z, Bai L, Wang Y, et al. Synergic fabrication of pembrolizumab loaded doxorubicin incorporating microbubbles delivery for ultrasound contrast agents mediated anti-proliferation and apoptosis. Drug Deliv 2021;28(1):1466-77. [PMID: 34259093 DOI: 10.1080/10717544.2021.1921080]
- Barmin RA, Dasgupta A, Bastard C, De Laporte L, Rütten S, et al. Engineering the acoustic response and drug loading capacity of PBCA-based polymeric microbubbles with surfactants. Mol Pharm 2022;19(9):3256-66. [PMID: 35905480 DOI: 10.1021/acs.molpharmaceut.2c00416]
- Ingram N, McVeigh LE, Abou-Saleh RH, Maynard J, Peyman SA, et al. Ultrasound-triggered therapeutic microbubbles enhance the efficacy of cytotoxic drugs by increasing circulation and tumor drug accumulation and limiting bioavailability and toxicity in normal tissues. Theranostics 2020;10(24):10973-92. [PMID: 33042265 DOI: 10.7150/thno.49670]
- Ingram N, Abou-Saleh RH, Race AD, Loadman PM, Bushby RJ, et al. Maleimide-thiol linkages alter the biodistribution of SN38 therapeutic microbubbles compared to biotin-avidin while preserving parity in tumoral drug delivery. Pharmaceutics 2024;16(3):434. [PMID: 38543328 DOI: 10.3390/pharmaceutics16030434]
- Huo S, Liao Z, Zhao P, Zhou Y, Göstl R, Herrmann A. Mechano-nanoswitches for ultrasound-controlled drug activation. Adv Sci 2022;9(12):e2104696. [PMID: 35195372 DOI: 10.1002/advs.202104696]
- Bergers G, Song S, Meyer-Morse N, Bergsland E, Hanahan D. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J Clin Invest 2003;111(9):1287-95. [PMID: 12727920 DOI: 10.1172/JCI17929]
- Siemann DW, Bibby MC, Dark GG, Dicker AP, Eskens FA, et al. Differentiation and definition of vascular-targeted therapies. Clin Cancer Res 2005;11(2 Pt 1):416-20. [PMID: 15701823]
- Kudo M, Han G, Finn RS, Poon RT, Blanc JF, et al. Brivanib as adjuvant therapy to transarterial chemoembolization in patients with hepatocellular carcinoma: a randomized phase III trial. Hepatology 2014;60(5):1697-707. [PMID: 24996197 DOI: 10.1002/hep.27290]
- Monk BJ, Minion LE, Coleman RL. Anti-angiogenic agents in ovarian cancer: past, present, and future. Ann Oncol 2016;27(Suppl 1):i33-9. [PMID: 27141068 DOI: 10.1093/annonc/mdw093]
- Liu Z, Zhang Y, Shen N, Sun J, Tang Z, et al. Destruction of tumor vasculature by vascular disrupting agents in overcoming the limitation of EPR effect. Adv Drug Deliv Rev 2022;183:114138. [PMID: 35143895 DOI: 10.1016/j.addr.2022.114138]
- Lei X, Chen M, Huang M, Li X, Shi C, et al. Desacetylvinblastine monohydrazide disrupts tumor vessels by promoting VE-cadherin internalization. Theranostics 2018;8(2):384-98. [PMID: 29290815 DOI: 10.7150/thno.22222]
- Dark GG, Hill SA, Prise VE, Tozer GM, Pettit GR, et al. Combretastatin A-4, an agent that displays potent and selective toxicity toward tumor vasculature. Cancer Res 1997;57(10):1829-34. [PMID: 9157969]
- Chase DM, Chaplin DJ, Monk BJ. The development and use of vascular targeted therapy in ovarian cancer. Gynecol Oncol 2017;145(2):393-406. [PMID: 28238563 DOI: 10.1016/j.ygyno.2017.01.031]
- Zweifel M, Jayson GC, Reed NS, Osborne R, Hassan B, et al. Phase II trial of combretastatin A4 phosphate, carboplatin, and paclitaxel in patients with platinum-resistant ovarian cancer. Ann Oncol 2011;22(9):2036-41. [PMID: 21273348 DOI: 10.1093/annonc/mdq708]
- Eskens FA, Tresca P, Tosi D, Van Doorn L, Fontaine H, et al. A phase I pharmacokinetic study of the vascular disrupting agent ombrabulin (AVE8062) and docetaxel in advanced solid tumours. Br J Cancer 2014;110(9):2170-7. [PMID: 24714750 DOI: 10.1038/bjc.2014.137]
- McKeage MJ. The potential of DMXAA (ASA404) in combination with docetaxel in advanced prostate cancer. Expert Opin Investig Drugs 2008;17(1):23-9. [PMID: 18095916 DOI: 10.1517/13543784.17.1.23]
- Tamura K, Nakagawa K, Kurata T, Satoh T, Nogami T, et al. Phase I study of TZT-1027, a novel synthetic dolastatin 10 derivative and inhibitor of tubulin polymerization, which was administered to patients with advanced solid tumors on days 1 and 8 in 3-week courses. Cancer Chemother Pharmacol 2007;60(2):285-93. [PMID: 17136542 DOI: 10.1007/s00280-006-0382-7]
- Ho YJ, Wang TC, Fan CH, Yeh CK. Current progress in antivascular tumor therapy. Drug Discov Today 2017;22(10):1503-15. [PMID: 28625610 DOI: 10.1016/j.drudis.2017.06.001]
- El Kaffas A, Gangeh MJ, Farhat G, Tran WT, Hashim A, et al. Tumour vascular shutdown and cell death following ultrasound-microbubble enhanced radiation therapy. Theranostics 2018;8(2):314-27. [PMID: 29290810 DOI: 10.7150/thno.19010]
- Gu L, Shen Z, Ji L, Ng DM, Du N, et al. High-intensity focused ultrasound alone or combined with transcatheter arterial chemoembolization for the treatment of hepatocellular carcinoma with unsuitable indications for hepatectomy and radiofrequency ablation: a phase II clinical trial. Surg Endosc 2022;36(3):1857-67. [PMID: 33788029 DOI: 10.1007/s00464-021-08465-3]
- Lee J, Karshafian R, Papanicolau N, Giles A, Kolios MC, et al. Quantitative ultrasound for the monitoring of novel microbubble and ultrasound radiosensitization. Ultrasound Med Biol 2012;38(7):1212-21. [PMID: 22579547 DOI: 10.1016/j.ultrasmedbio.2012.01.028]
- Zhao X, Pellow C, Goertz DE. Intravital imaging and cavitation monitoring of antivascular ultrasound in tumor microvasculature. Theranostics 2023;13(1):250-66. [PMID: 36593952 DOI: 10.7150/thno.79186]
- Abdulkarim B, Deutsch E. Endothelial-cell apoptosis and tumour response to radiotherapy. Lancet Oncol 2004;5(1):9. [PMID: 14700602 DOI: 10.1016/s1470-2045(03)01317-2]
- Daecher A, Stanczak M, Liu JB, Zhang J, Du S, et al. Localized microbubble cavitation-based antivascular therapy for improving HCC treatment response to radiotherapy. Cancer Lett 2017;411:100-5. [PMID: 28969964 DOI: 10.1016/j.canlet.2017.09.037]
- Hwang JH, Brayman AA, Reidy MA, Matula TJ, Kimmey MB, et al. Vascular effects induced by combined 1-MHz ultrasound and microbubble contrast agent treatments in vivo. Ultrasound Med Biol 2005;31(4):553-64. [PMID: 15831334 DOI: 10.1016/j.ultrasmedbio.2004.12.014]
- Jing Y, Xiu-Juan Z, Hong-Jiao C, Zhi-Kui C, Qing-Fu Q, et al. Ultrasound-targeted microbubble destruction improved the antiangiogenic effect of endostar in triple-negative breast carcinoma xenografts. J Cancer Res Clin Oncol 2019;145(5):1191-200. [PMID: 30805775 DOI: 10.1007/s00432-019-02866-7]
- Liu Z, Gao S, Zhao Y, Li P, Liu J, et al. Disruption of tumor neovasculature by microbubble enhanced ultrasound: a potential new physical therapy of anti-angiogenesis. Ultrasound Med Biol 2012;38(2):253-61. [PMID: 22178162 DOI: 10.1016/j.ultrasmedbio.2011.11.007]
- Tozer GM, Kanthou C, Baguley BC. Disrupting tumour blood vessels. Nat Rev Cancer 2005;5(6):423-35. [PMID: 15928673 DOI: 10.1038/nrc1628]
- Frentzas S, Simoneau E, Bridgeman VL, Vermeulen PB, Foo S, et al. Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat Med 2016;22(11):1294-302. [PMID: 27748747 DOI: 10.1038/nm.4197]
- Xie H, Li W, Liu H, Chen Y, Ma M, et al. Erythrocyte membrane-coated invisible acoustic-sensitive nanoparticle for inducing tumor thrombotic infarction by precisely damaging tumor vascular endothelium. Small 2022;18(30):e2201933. [PMID: 35789094 DOI: 10.1002/smll.202201933]
- Cobleigh MA, Langmuir VK, Sledge GW, Miller KD, Haney L, et al. A phase I/II dose-escalation trial of bevacizumab in previously treated metastatic breast cancer. Semin Oncol 2003;30(5 Suppl 16):117-24. [PMID: 14613032 DOI: 10.1053/j.seminoncol.2003.08.013]
- Tebbutt NC, Wilson K, Gebski VJ, Cummins MM, Zannino D, et al. Capecitabine, bevacizumab, and mitomycin in first-line treatment of metastatic colorectal cancer: results of the Australasian Gastrointestinal Trials Group Randomized Phase III MAX Study. J Clin Oncol 2010;28(19):3191-8. [PMID: 20516443 DOI: 10.1200/JCO.2009.27.7723]
- Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350(23):2335-42. [PMID: 15175435 DOI: 10.1056/NEJMoa032691]
- Jain RK. Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combination therapy. Nat Med 2001;7(9):987-9. [PMID: 11533692 DOI: 10.1038/nm0901-987]
- Winkler F, Kozin SV, Tong RT, Chae SS, Booth MF, et al. Kinetics of vascular normalization by VEGFR2 blockade governs brain tumor response to radiation: role of oxygenation, angiopoietin-1, and matrix metalloproteinases. Cancer Cell 2004;6(6):553-63. [DOI: 10.1016/j.ccr.2004.10.011]
- Willett CG, Boucher Y, di Tomaso E, Duda DG, Munn LL, et al. Direct evidence that the VEGF-specific antibody bevacizumab has antivascular effects in human rectal cancer. Nat Med 2004;10(2):145-7. [PMID: 14745444 DOI: 10.1038/nm988]
- Willett CG, Boucher Y, Duda DG, di Tomaso E, Munn LL, et al. Surrogate markers for antiangiogenic therapy and dose-limiting toxicities for bevacizumab with radiation and chemotherapy: continued experience of a phase I trial in rectal cancer patients. J Clin Oncol 2005;23(31):8136-9. [PMID: 16258121 DOI: 10.1200/JCO.2005.02.5635]
- Mpekris F, Panagi M, Charalambous A, Voutouri C, Stylianopoulos T. Modulating cancer mechanopathology to restore vascular function and enhance immunotherapy. Cell Rep Med 2024;5(7):101626. [PMID: 38944037 DOI: 10.1016/j.xcrm.2024.101626]
- Trédan O, Galmarini CM, Patel K, Tannock IF. Drug resistance and the solid tumor microenvironment. J Natl Cancer Inst 2007;99(19):1441-54. [PMID: 17895480 DOI: 10.1093/jnci/djm135]
- Dickson PV, Hamner JB, Sims TL, Fraga CH, Ng CY, et al. Bevacizumabinduced transient remodeling of the vasculature in neuroblastoma xenografts results in improved delivery and efficacy of systemically administered chemotherapy . Clin Cancer Res 2007;13(13):3942-50. [PMID: 17606728 DOI: 10.1158/1078-0432.CCR-07-0278]
- McGee MC, Hamner JB, Williams RF, Rosati SF, Sims TL, et al. Improved intratumoral oxygenation through vascular normalization increases glioma sensitivity to ionizing radiation. Int J Radiat Oncol Biol Phys 2010;76(5):1537-45. [PMID: 20338480 DOI: 10.1016/j.ijrobp.2009.12.010]
- Van der Veldt AA, Lubberink M, Bahce I, Walraven M, de Boer MP, et al. Rapid decrease in delivery of chemotherapy to tumors after anti-VEGF therapy: implications for scheduling of anti-angiogenic drugs. Cancer Cell 2012;21(1):82-91. [PMID: 22264790 DOI: 10.1016/j.ccr.2011.11.023]
- Shan Y, Ni Q, Zhang Q, Zhang M, Wei B, et al. Targeting tumor endothelial hyperglycolysis enhances immunotherapy through remodeling tumor microenvironment. Acta Pharm Sin B 2022;12(4):1825-39. [PMID: 35847509 DOI: 10.1016/j.apsb.2022.02.014]
- Huang Y, Yuan J, Righi E, Kamoun WS, Ancukiewicz M, et al. Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. Proc Natl Acad Sci U S A 2012;109(43):17561-6. [PMID: 23045683 DOI: 10.1073/pnas.1215397109]
- Seyedmirzaei Sarraf S, Rokhsar Talabazar F, Namli I, Maleki M, Sheibani Aghdam A, et al. Fundamentals, biomedical applications and future potential of micro-scale cavitation-a review. Lab Chip 2022;22(12):2237-58. [DOI: 10.1039/D2LC00169A]
- Belcik JT, Mott BH, Xie A, Zhao Y, Kim S, et al. Augmentation of limb perfusion and reversal of tissue ischemia produced by ultrasound-mediated microbubble cavitation. Circ Cardiovasc Imaging 2015;8(4):e002979. [PMID: 25834183 DOI: 10.1161/CIRCIMAGING.114.002979]
- Li N, Tang J, Yang J, Zhu B, Wang X, et al. Tumor perfusion enhancement by ultrasound stimulated microbubbles potentiates PD-L1 blockade of MC38 colon cancer in mice. Cancer Lett 2021;498:121-9. [PMID: 33129956 DOI: 10.1016/j.canlet.2020.10.046]
- Tang N, Tang J, Tang J, Zhu Q, Dong X, et al. Sononeoperfusion: a new therapeutic effect to enhance tumour blood perfusion using diagnostic ultrasound and microbubbles. Cancer Imaging 2023;23(1):29. [PMID: 36959681 DOI: 10.1186/s40644-023-00545-y]
- Yang G, Li H, Yin J, Yao L, Yang J, et al. Alleviating tumor hypoxia and immunosuppression via sononeoperfusion: a new ally for potentiating anti-PD-L1 blockade of solid tumor. Ultrason Sonochem 2025;112:107115. [PMID: 39482116 DOI: 10.1016/j.ultsonch.2024.107115]
- Miller DL. Overview of experimental studies of biological effects of medical ultrasound caused by gas body activation and inertial cavitation. Prog Biophys Mol Biol 2007;93(1-3):314-30. [PMID: 16989895 DOI: 10.1016/j.pbiomolbio.2006.07.027]
- Gao Y, Gao S, Zhao B, Zhao Y, Hua X, et al. Vascular effects of microbubble-enhanced, pulsed, focused ultrasound on liver blood perfusion. Ultrasound Med Biol 2012;38(1):91-8. [PMID: 22104531 DOI: 10.1016/j.ultrasmedbio.2011.09.018]
- Mason OR, Davidson BP, Sheeran P, Muller M, Hodovan JM, et al. Augmentation of tissue perfusion in patients with peripheral artery disease using microbubble cavitation. JACC Cardiovasc Imaging 2020;13(3):641-51. [PMID: 31422129 DOI: 10.1016/j.jcmg.2019.06.012]
- Moccetti F, Belcik T, Latifi Y, Xie A, Ozawa K, et al. Flow augmentation in the myocardium by ultrasound cavitation of microbubbles: role of shear-mediated purinergic signaling. J Am Soc Echocardiogr 2020;3(8):1023-31.e2. [PMID: 32532642 DOI: 10.1016/j.echo.2020.03.016]
- Bulner S, Prodeus A, Gariepy J, Hynynen K, Goertz DE. Enhancing checkpoint inhibitor therapy with ultrasound stimulated microbubbles. Ultrasound Med Biol 2019;45(2):500-12. [PMID: 30447880 DOI: 10.1016/j.ultrasmedbio.2018.10.002]
- Li C, Xiao C, Zhan L, Zhang Z, Xing J, et al. Wireless electrical stimulation at the nanoscale interface induces tumor vascular normalization. Bioact Mater 2022;18:399-408. [PMID: 35415302 DOI: 10.1016/j.bioactmat.2022.03.027]
- Liang Y, Zhang S, Wang D, Ji P, Zhang B, et al. Dual-functional nanodroplet for tumor vasculature ultrasound imaging and tumor immunosuppressive microenvironment remodeling. Adv Healthc Mater 2024;13(31):e2401274. [PMID: 39031111 DOI: 10.1002/adhm.202401274]
- Qin H, Yu H, Sheng J, Zhang D, Shen N, et al. PI3Kgamma inhibitor attenuates immunosuppressive effect of poly(l-Glutamic Acid)-combretastatin A4 conjugate in metastatic breast cancer. Adv Sci 2019;6(12):1900327. [PMID: 31380170 DOI: 10.1002/advs.201900327]
- Zhao B, Dong Z, Liu W, Lou F, Wang Q, et al. Co-administration of combretastatin A4 nanoparticles and anti-PD-L1 for synergistic therapy of hepatocellular carcinoma. J Nanobiotechnology 2021;19(1):124. [PMID: 33933077 DOI: 10.1186/s12951-021-00865-w]
- Bao X, Shen N, Lou Y, Yu H, Wang Y, et al. Enhanced anti-PD-1 therapy in hepatocellular carcinoma by tumor vascular disruption and normalization dependent on combretastatin A4 nanoparticles and DC101. Theranostics 2021;11(12):5955-69. [PMID: 33897892 DOI: 10.7150/thno.58164]
- Wang B, Zhai Y, Shi J, Zhuang L, Liu W, et al. Simultaneously overcome tumor vascular endothelium and extracellular matrix barriers via a non-destructive size-controlled nanomedicine. J Control Release 2017;268:225-36. [PMID: 29054372 DOI: 10.1016/j.jconrel.2017.10.029]
- Bellary A, Nowak C, Iwanicki I, Flores-Guzman F, Wu L, et al. Non-viral nitric oxide-based gene therapy improves perfusion and liposomal doxorubicin sonopermeation in neuroblastoma models. Theranostics 2023;13(10):3402-18. [PMID: 37351172 DOI: 10.7150/thno.81700]
- Shirvalilou S, Tavangari Z, Parsaei MH, Sargazi S, Sheervalilou R, et al. The future opportunities and remaining challenges in the application of nanoparticle-mediated hyperthermia combined with chemo-radiotherapy in cancer. Wiley Interdiscip Rev Nanomed Nanobiotechnol 2023;15(6):e1922. [PMID: 37778031 DOI: 10.1002/wnan.1922]
- Xia H, Zhu J, Men C, Wang A, Mao Q, et al. Light-initiated aggregation of gold nanoparticles for synergistic chemo-photothermal tumor therapy. Nanoscale Adv 2023;5(11):3053-62. [PMID: 37260491 DOI: 10.1039/d3na00114h]
- Xiang Y, Tang L, Pang H, Xu H, He Y, et al. Ultrasound -induced thermal effect enhances the efficacy of chemotherapy and immunotherapy in tumor treatment. Int J Nanomedicine 2024;19:6677-92. [PMID: 38975322 DOI: 10.2147/IJN.S464830]
- Gouda MA, Janku F, Wahida A, Buschhorn L, Schneeweiss A, et al. Liquid biopsy response evaluation criteria in solid tumors (LB-RECIST). Ann Oncol 2024;35(3):267-75. [PMID: 38145866 DOI: 10.1016/j.annonc.2023.12.007]
- Jain RK, Duda DG, Willett CG, Sahani DV, Zhu AX, et al. Biomarkers of response and resistance to antiangiogenic therapy. Nat Rev Clin Oncol 2009;6(6):327-38. [PMID: 19483739 DOI: 10.1038/nrclinonc.2009.63]
- Huang Y, Goel S, Duda DG, Fukumura D, Jain RK. Vascular normalization as an emerging strategy to enhance cancer immunotherapy. Cancer Res 2013;73(10):2943-8. [PMID: 23440426 DOI: 10.1158/0008-5472.CAN-12-4354]
- Shrestha B, Stern NB, Zhou A, Dunn A, Porter T. Current trends in the characterization and monitoring of vascular response to cancer therapy. Cancer Imaging 2024;24(1):143. [PMID: 39438891 DOI: 10.1186/s40644-024-00767-8]
- Aziz MU, Eisenbrey JR, Deganello A, Zahid M, Sharbidre K, et al. Microvascular flow imaging: a state-of-the-art review of clinical use and promise. Radiology 2022;305(2):250-64.
- Yang WT, Chang J, Metreweli C. Patients with breast cancer: differences in color Doppler flow and gray-scale US features of benign and malignant axillary lymph nodes. Radiology 2000;215(2):568-73. [PMID: 10796941 DOI: 10.1148/radiology.215.2.r00ap20568]
- Liu M, Cai L, Li Q, Chen X, Gao L, et al. The expression of VEGF and CD31 in endometrial lesions and its associations with blood flow parameters of transvaginal 3D power Doppler ultrasonography: a preliminary study. Cancer Manag Res 2020;12:11211-8. [PMID: 33177872 DOI: 10.2147/CMAR.S277274]
- Demené C, Payen T, Dizeux A, Barrois G, Gennisson JL, et al. 3-D longitudinal imaging of tumor angiogenesis in mice in vivo using ultrafast Doppler tomography. Ultrasound Med Biol 2019;45(5):1284-96. [PMID: 30799125 DOI: 10.1016/j.ultrasmedbio.2018.12.010]
- Mace E, Montaldo G, Osmanski BF, Cohen I, Fink M, et al. Functional ultrasound imaging of the brain: theory and basic principles. IEEE Trans Ultrason Ferroelectr Freq Control 2013;60(3):492-506. [PMID: 23475916 DOI: 10.1109/TUFFC.2013.2592]
- Hashizume H, Baluk P, Morikawa S, McLean JW, Thurston G, et al. Openings between defective endothelial cells explain tumor vessel leakiness. Am J Pathol 2000;156(4):1363-80. [PMID: 10751361 DOI: 10.1016/S0002-9440(10)65006-7]
- Rix A, Piepenbrock M, Flege B, von Stillfried S, Koczera P, et al. Effects of contrast-enhanced ultrasound treatment on neoadjuvant chemotherapy in breast cancer. Theranostics 2021;11(19):9557-70. [PMID: 34646386 DOI: 10.7150/thno.64767]
- Schutt EG, Klein DH, Mattrey RM, Riess JG. Injectable microbubbles as contrast agents for diagnostic ultrasound imaging: the key role of perfluorochemicals. Angew Chem Int Ed Engl 2003;42(28):3218-35. [PMID: 12876730 DOI: 10.1002/anie.200200550]
- Leong-Poi H. Molecular imaging using contrast-enhanced ultrasound: evaluation of angiogenesis and cell therapy. Cardiovasc Res 2009;84(2):190-200. [PMID: 19628466 DOI: 10.1093/cvr/cvp248]
- Zhang G, Ye HR, Sun Y, Guo ZZ. Ultrasound molecular imaging and its applications in cancer diagnosis and therapy. ACS Sens 2022;7(10):2857-64. [PMID: 36190830 DOI: 10.1021/acssensors.2c01468]
- Caremani M, Benci A, Lapini L, Tacconi D, Caremani A, et al. Contrast enhanced ultrasonography (CEUS) in peripheral lung lesions: a study of 60 cases. J Ultrasound 2008;11(3):89-96. [PMID: 23397023 DOI: 10.1016/j.jus.2008.05.008]
- Wang Y, Li L, Wang YX, Cui NY, Zou SM, et al. Time-intensity curve parameters in rectal cancer measured using endorectal ultrasonography with sterile coupling gels filling the rectum: correlations with tumor angiogenesis and clinicopathological features. Biomed Res Int 2014;2014(1):587806. [PMID: 24900973 DOI: 10.1155/2014/587806]
- Cartana ET, Gheonea DI, Cherciu IF, Streaţa I, Uscatu CD, et al. Assessing tumor angiogenesis in colorectal cancer by quantitative contrast-enhanced endoscopic ultrasound and molecular and immunohistochemical analysis. Endosc Ultrasound 2018;7(3):175-83. [PMID: 28685747 DOI: 10.4103/eus.eus_7_17]
- Malmstrøm ML, Săftoiu A, Riis LB, Hassan H, Klausen TW, et al. Dynamic contrast-enhanced EUS for quantification of tumor perfusion in colonic cancer: a prospective cohort study. Gastrointest Endosc 2018;87(6):1530-8. [PMID: 29329991 DOI: 10.1016/j.gie.2018.01.001]
- Ntoulia A, Anupindi SA, Darge K, Back SJ. Applications of contrast-enhanced ultrasound in the pediatric abdomen. Abdom Radiol 2018;43(4):948-59. [PMID: 28980061 DOI: 10.1007/s00261-017-1315-0]
- Santiesteban DY, Hallam KA, Yarmoska SK, Emelianov SY. Color-coded perfluorocarbon nanodroplets for multiplexed ultrasound and Photoacoustic imaging. Nano Res 2019;12(4):741-7. [PMID: 31572565 DOI: 10.1007/s12274-019-2279-x]
- Laumer F, Di Vece D, Cammann VL, Würdinger M, Petkova V, et al. Assessment of artificial intelligence in echocardiography diagnostics in differentiating takotsubo syndrome from myocardial infarction. JAMA Cardiol 2022;7(5):494-503. [PMID: 35353118 DOI: 10.1001/jamacardio.2022.0183]
- Chen ZY, Wang YX, Lin Y, Zhang JS, Yang F, et al. Advance of molecular imaging technology and targeted imaging agent in imaging and therapy. Biomed Res Int 2014;2014(1):819324. [PMID: 24689058 DOI: 10.1155/2014/819324]
- Verger A, Grimaldi S, Ribeiro MJ, Frismand S, Guedj E. Single photon emission computed tomography/positron emission tomography molecular imaging for parkinsonism: a fast-developing field. Ann Neurol 2021;90(5):711-9. [PMID: 34338333 DOI: 10.1002/ana.26187]
- Siddiqui S, Kadlecek S, Pourfathi M, Xin Y, Mannherz W, et al. The use of hyperpolarized carbon-13 magnetic resonance for molecular imaging. Adv Drug Deliv Rev 2017;113:3-23. [PMID: 27599979 DOI: 10.1016/j.addr.2016.08.011]
- Zhang H, Tam S, Ingham ES, Mahakian LM, Lai CY, et al. Ultrasound molecular imaging of tumor angiogenesis with a neuropilin-1-targeted microbubble. Biomaterials 2015;56:104-13. [PMID: 25934284 DOI: 10.1016/j.biomaterials.2015.03.043]
- Wang J, Wang Y, Zhong L, Yan F, Zheng H. Nanoscale contrast agents: a promising tool for ultrasound imaging and therapy. Adv Drug Deliv Rev 2024;207:115200. [PMID: 38364906 DOI: 10.1016/j.addr.2024.115200]
- Seol SH, Lindner JR. A primer on the methods and applications for contrast echocardiography in clinical imaging. J Cardiovasc Ultrasound 2014;22(3):101-10. [PMID: 25309685 DOI: 10.4250/jcu.2014.22.3.101]
- Wang S, Hossack JA, Klibanov AL. Targeting of microbubbles: contrast agents for ultrasound molecular imaging. J Drug Target 2018;26(5-6):420-34. [PMID: 29258335 DOI: 10.1080/1061186X.2017.1419362]
- Reinhardt M, Hauff P, Briel A, Uhlendorf V, Linker RA, et al. Sensitive particle acoustic quantification (SPAQ): a new ultrasound-based approach for the quantification of ultrasound contrast media in high concentrations. Invest Radiol 2005;40(1):2-7. [PMID: 15597013]
- El Kaffas A, Sigrist RMS, Fisher G, Bachawal S, Liau J, et al. Quantitative three-dimensional dynamic contrast-enhanced ultrasound imaging: first-in-human pilot study in patients with liver metastases. Theranostics 2017;7(15):3745-58. [PMID: 29109773 DOI: 10.7150/thno.20329]
- Fournier L, de La Taille T, Chauvierre C. Microbubbles for human diagnosis and therapy. Biomaterials 2023;294:122025. [PMID: 36716588 DOI: 10.1016/j.biomaterials.2023.122025]
- Smeenge M, Tranquart F, Mannaerts CK, de Reijke TM, van de Vijver MJ, et al. First-in-human ultrasound molecular imaging with a VEGFR2-specific ultrasound molecular contrast agent (BR55) in prostate cancer: a safety and feasibility pilot study. Invest Radiol 2017;52(7):419-27. [PMID: 28257340 DOI: 10.1097/RLI.0000000000000362]
- Willmann JK, Bonomo L, Testa AC, Rinaldi P, Rindi G, et al. Ultrasound molecular imaging with BR55 in patients with breast and ovarian lesions: first-in-human results. J Clin Oncol 2017;35(19):2133-40. [PMID: 28291391 DOI: 10.1200/JCO.2016.70.8594]
- Willmann JK, Paulmurugan R, Chen K, Gheysens O, Rodriguez-Porcel M, et al. US imaging of tumor angiogenesis with microbubbles targeted to vascular endothelial growth factor receptor type 2 in mice. Radiology 2008;246(2):508-18. [PMID: 18180339 DOI: 10.1148/radiol.2462070536]
- John R, Nguyen FT, Kolbeck KJ, Chaney EJ, Marjanovic M, et al. Targeted multifunctional multimodal protein-shell microspheres as cancer imaging contrast agents. Mol Imaging Biol 2012;14(1):17-24. [PMID: 21298354 DOI: 10.1007/s11307-011-0473-7]
- Fan CH, Cheng YH, Ting CY, Ho YJ, Hsu PH, et al. Ultrasound/magnetic targeting with SPIO-DOX-microbubble complex for image-guided drug delivery in brain tumors. Theranostics 2016;6(10):1542-56. [PMID: 27446489 DOI: 10.7150/thno.15297]
- Li X, Xing L, Zheng K, Wei P, Du L, et al. Formation of gold nanostar-coated hollow mesoporous silica for tumor multimodality imaging and photothermal therapy. ACS Appl Mater Interfaces 2017;9(7):5817-27. [PMID: 28118704 DOI: 10.1021/acsami.6b15185]
- Zhao F, Unnikrishnan S, Herbst EB, Klibanov AL, Mauldin FW Jr, et al. A targeted molecular localization imaging method applied to tumor microvasculature. Invest Radiol 2021;56(4):197-206. [PMID: 32976207 DOI: 10.1097/RLI.0000000000000728]
- Ilovitsh T, Ilovitsh A, Foiret J, Fite BZ, Ferrara KW. Acoustical structured illumination for super-resolution ultrasound imaging. Commun Biol 2018;1(1):3. [DOI: 10.1038/s42003-017-0003-5]
- Christensen-Jeffries K, Couture O, Dayton PA, Eldar YC, Hynynen K, et al. Super-resolution ultrasound imaging. Ultrasound Med Biol 2020;46(4):865-91. [PMID: 31973952 DOI: 10.1016/j.ultrasmedbio.2019.11.013]
- Couture O, Bannouf S, Montaldo G, Aubry JF, Fink M, et al. Ultrafast imaging of ultrasound contrast agents. Ultrasound Med Biol 2009;35(11):1908-16. [PMID: 19699026 DOI: 10.1016/j.ultrasmedbio.2009.05.020]
- Couture O, Fink M, Tanter M. Ultrasound contrast plane wave imaging. IEEE Trans Ultrason Ferroelectr Freq Control 2012;59(12):2676-83. [PMID: 23221216 DOI: 10.1109/TUFFC.2012.2508]
- Viessmann OM, Eckersley RJ, Christensen-Jeffries K, Tang MX, Dunsby C. Acoustic super-resolution with ultrasound and microbubbles. Phys Med Biol 2013;58(18):6447-58. [PMID: 23999099 DOI: 10.1088/0031-9155/58/18/6447]
- Ghosh D, Xiong F, Sirsi SR, Mattrey R, Brekken R, et al. Monitoring early tumor response to vascular targeted therapy using super-resolution ultrasound imaging. Washington, DC, USA: IEEE International Ultrasonics Symposium (IUS); 2017. [DOI: 10.1109/ULTSYM.2017.8092944]
- Kollmann C, Jenderka KV, Moran CM, Draghi F, Jimenez Diaz JF, et al. EFSUMB clinical safety statement for diagnostic ultrasound – (2019 revision). Ultraschall Med 2020;41(4):387-9. [PMID: 31594007 DOI: 10.1055/a-1010-6018]
- Ternifi R, Wang Y, Gu J, Polley EC, Carter JM, et al. Ultrasound high-definition microvasculature imaging with novel quantitative biomarkers improves breast cancer detection accuracy. Eur Radiol 2022;32(11):7448-62. [PMID: 35486168 DOI: 10.1007/s00330-022-08815-2]
- Sabeti S, Ternifi R, Larson NB, Olson MC, Atwell TD, et al. Morphometric analysis of tumor microvessels for detection of hepatocellular carcinoma using contrast-free ultrasound imaging: a feasibility study. Front Oncol 2023;13:1121664. [PMID: 37124492 DOI: 10.3389/fonc.2023.1121664]
- Adusei SA, Sabeti S, Larson NB, Dalvin LA, Fatemi M, et al. Quantitative biomarkers derived from a novel, contrast-free ultrasound, high-definition microvessel imaging for differentiating choroidal tumors. Cancers 2024;16(2):395. [PMID: 38254884 DOI: 10.3390/cancers16020395]
- Sabeti S, Larson NB, Boughey JC, Stan DL, Solanki MH, et al. Ultrasound-based quantitative microvasculature imaging for early prediction of response to neoadjuvant chemotherapy in patients with breast cancer. Breast Cancer Res 2025;27(1):24. [PMID: 39962614 DOI: 10.1186/s13058-025-01978-y]
- Mendiratta-Lala M, Wiggermann P, Pech M, Serres-Créixams X, White SB, et al. The #HOPE4LIVER single-arm pivotal trial for histotripsy of primary and metastatic liver tumors. Radiology 2024;312(3):e233051. [PMID: 39225612 DOI: 10.1148/radiol.233051]
- Wu F, Wang ZB, Cao YD, Chen WZ, Bai J, et al. A randomised clinical trial of high-intensity focused ultrasound ablation for the treatment of patients with localised breast cancer. Br J Cancer 2003;89(12):2227-33. [PMID: 14676799 DOI: 10.1038/sj.bjc.6601411]
- Zhu XQ, Lu P, Xu ZL, Zhou Q, Zhang J, et al. Alterations in immune response profile of tumor-draining lymph nodes after high-intensity focused ultrasound ablation of breast cancer patients. Cells 2021;10(12):3346. [PMID: 34943854 DOI: 10.3390/cells10123346]
- Lee JY, Chung HH, Kang SY, Park EJ, Park DH, et al. Portable ultrasound-guided high-intensity focused ultrasound with functions for safe and rapid ablation: prospective clinical trial for uterine fibroids-short-term and long-term results. Eur Radiol 2020;30(3):1554-63. [PMID: 31705252 DOI: 10.1007/s00330-019-06468-2]
- Chen X, Gole J, Gore A, He Q, Lu M, et al. Non-invasive early detection of cancer four years before conventional diagnosis using a blood test. Nat Commun 2020;11(1):3475. [PMID: 32694610 DOI: 10.1038/s41467-020-17316-z]
- Bogers HA, Sedelaar JP, Beerlage HP, de la Rosette JJ, Debruyne FM, et al. Contrast-enhanced three-dimensional power Doppler angiography of the human prostate: correlation with biopsy outcome. Urology 1999;54(1):97-104. [PMID: 10414734 DOI: 10.1016/s0090-4295(99)00040-0]
- Görges R, Eising EG, Fotescu D, Renzing-Köhler K, Frilling A, et al. Diagnostic value of high-resolution B-mode and power-mode sonography in the follow-up of thyroid cancer. Eur J Ultrasound. 2003;16(3):191-206. [PMID: 12573788 DOI: 10.1016/s0929-8266(02)00073-3]
- Kabil Kucur S, Temizkan O, Atis A, Gozukara I, Uludag EU, et al. Role of endometrial power Doppler ultrasound using the international endometrial tumor analysis group classification in predicting intrauterine pathology. Arch Gynecol Obstet 2013;288(3):649-54. [PMID: 23529686 DOI: 10.1007/s00404-013-2813-0]
- Chen M, Wang WP, Jia WR, Tang L, Wang Y, et al. Three-dimensional contrast-enhanced sonography in the assessment of breast tumor angiogenesis: correlation with microvessel density and vascular endothelial growth factor expression. J Ultrasound Med 2014;33(5):835-46. [PMID: 24764339 DOI: 10.7863/ultra.33.5.835]
- Hoyt K, Umphrey H, Lockhart M, Robbin M, Forero-Torres A. Ultrasound imaging of breast tumor perfusion and neovascular morphology. Ultrasound Med Biol 2015;41(9):2292-302. [PMID: 26116159 DOI: 10.1016/j.ultrasmedbio.2015.04.016]
- Bezircioglu I, Baloglu A, Tarhan MO, Oziz E, Yigit S. Evaluation of endometrium by transvaginal ultrasonography and Doppler in tamoxifen-treated women with breast cancer. Eur J Gynaecol Oncol 2012;33(3):295-9. [PMID: 22873103 DOI: 10.12892/ejgo201203295]
- Pochon S, Tardy I, Bussat P, Bettinger T, Brochot J, et al. BR55: a lipopeptide-based VEGFR2-targeted ultrasound contrast agent for molecular imaging of angiogenesis. Invest Radiol 2010;45(2):89-95. [PMID: 20027118 DOI: 10.1097/RLI.0b013e3181c5927c]
- Baetke SC, Rix A, Tranquart F, Schneider R, Lammers T, et al. Squamous cell carcinoma xenografts: use of VEGFR2-targeted microbubbles for combined functional and molecular US to monitor antiangiogenic therapy effects. Radiology 2016;278(2):430-40. [PMID: 26313618 DOI: 10.1148/radiol.2015142899]
- Helbert A, Von Wronski M, Colevret D, Botteron C, Padilla F, et al. Ultrasound molecular imaging with BR55, a predictive tool of antiangiogenic treatment efficacy in a chemo-induced mammary tumor model. Invest Radiol 2020;55(10):657-65. [PMID: 32229739 DOI: 10.1097/RLI.0000000000000661]
- Qiu C, Sha T, Yin T, Zhang W, Chen X, et al. VEGFR2-targeted ultrasound molecular imaging of angiogenesis to evaluate liver allograft fibrosis. Biomater Sci 2021;9(17):5802-11. [PMID: 34008615 DOI: 10.1039/d1bm00100k]