Progress in the Application of Nano- and Micro-based Drug Delivery Systems in Pulmonary Drug Delivery
1School of Pharmaceutical Sciences, Wenzhou Medical University, Wenzhou 325035, China
*Correspondence to: Cui-Tao Lu, E-mail: lctuua@163.com; Ying-Zheng Zhao, E-mail: yqpharm@163.com
Received: August 13 2021; Revised: August 30 2021; Accepted: October 13 2021; Published Online: November 4 2021
Cite this paper:
Rejoice Thubelihle Ndebele, Qing Yao, Yan-Nan Shi, Yuan-Yuan Zhai, He-Lin Xu, Cui-Tao Lu and Ying-Zheng Zhao. Progress in the Application of Nano- and Micro-based Drug Delivery Systems in Pulmonary Drug Delivery. BIO Integration 2022; 3(2): 71–83.
DOI: 10.15212/bioi-2021-0028. Available at: https://bio-integration.org/
Download citation 
© 2022 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Nanotechnology is associated with the development of particles in the nano-size range that can be used in a wide range of applications in the medical field. It has gained more importance in the pharmaceutical research field particularly in drug delivery, as it results in enhanced therapeutic drug performance, improved drug solubility, targeted drug delivery to the specific sites, minimized side effects, and prolonged drug retention time in the targeted site. To date, the application of nanotechnology continues to offer several benefits in the treatment of various chronic diseases and results in remarkable improvements in treatment outcomes. The use of nano-based delivery systems such as liposomes, micelles, and nanoparticles in pulmonary drug delivery have shown to be a promising strategy in achieving drug deposition and maintained controlled drug release in the lungs. They have been widely used to minimize the risks of drug toxicity in vivo. In this review, recent advances in the application of nano- and micro-based delivery systems in pulmonary drug delivery for the treatment of various pulmonary diseases, such as lung cancer, asthma, and chronic obstructive pulmonary disease, are highlighted. Limitations in the application of these drug delivery systems and some key strategies in improving their formulation properties to overcome challenges encountered in drug delivery are also discussed.
Keywords
Nanotechnology, pulmonary drug delivery, nanoparticles, liposomes, micelles, controlled release.
Introduction
Pulmonary diseases have become one of the common threats to human health and are known to be a leading cause of mortality worldwide. These are diseases that mainly affect the lungs and can also spread to the other parts of the respiratory system, and they include asthma, lung cancer, and chronic obstructive pulmonary diseases (COPD; e.g., chronic bronchitis and emphysema) [1]. Pulmonary drug delivery is one of the effective routes of drug administration in the treatment of pulmonary diseases and has been widely used owing to its potential in achieving both systemic and local drug delivery.
Pulmonary drug delivery has gained much biomedical importance in the field of pharmaceutical research. At present, it has become one of the most preferred routes of administration. This is mainly because, through the pulmonary route, drugs can be directly delivered to the lungs [2]. When compared with oral and intravenous routes of administration, pulmonary route offers a number of advantages in the treatment of respiratory diseases. It also achieves a rapid onset of drug action and results in a high pulmonary efficacy with low drug doses whereas higher doses are required in peroral applications to achieve the same effect and may possibly result in more side effects. Additionally, through the pulmonary route, drug bioavailability can be improved unlike in the other routes of drug administration. More importantly, when drugs are administered via the pulmonary route, the first-pass metabolism that normally occurs following oral administration can be avoided [3, 4]. Drug inhalation has been proven to result in an increased pulmonary efficacy and a rapid onset of action in the lungs and is also associated with reduced systemic side effects [2]. In addition, it is a non-invasive route of administration and is therefore preferred by most of the patients.
The type of drug delivery device, dosage form used, and deposition of drug particles are some of the several factors that influence pulmonary drug efficacy [5, 6]. The technique of drug delivery to the targeted site also plays a prominent role in achieving maximum drug efficacy. Challenges encountered in conventional therapy, such as the need for drug administration in high doses to achieve high drug concentration in specific sites, have led to the clinical application of drug-targeted delivery systems as an alternative strategy to improve the treatment outcomes of several pulmonary diseases. At present, the challenges encountered in drug delivery in the treatment of pulmonary diseases such as in vivo instability, poor solubility, and absorption of the drugs can be overcome by the use of nano- and micro-based drug delivery systems owing to their ability to enhance drug solubility, absorption, and controlled release in the target site. Several limitations in the efficient drug delivery to the site of action, such as limited amount of drug particles passing through physiological barriers, have led to the development of drug delivery systems as a strategy to ensure maximal delivery of therapeutic agents to the targeted sites with minimized systemic side effects. For instance, in the treatment of lung cancer, the delivery of chemotherapeutic drugs via inhalation can be limited by several physiological barriers that can affect drug efficacy and deposition in the lung. To overcome this challenge, lipid-based drug carriers can be used for both passive and active targeting [7], owing to their enhanced permeability and retention effect and their ability to be modified with various targeting moieties. Drugs can be encapsulated in various drug delivery systems to not only protect them from enzyme degradation but also improve their stability in vivo, ensure targeted delivery, and controlled release to the site of action thereby improving the treatment outcomes [8]. Targeted drug delivery and controlled drug release result in an increased drug therapeutic index, and a less amount of drug accumulation in normal healthy tissues since drug targeting is site-specific. As a result, the frequent dosing that is normally required in conventional therapy to achieve maximum drug deposition at a specific site can be minimized. In recent years, the developments in nano-based drug delivery have shown to have several benefits, which include improved drug efficacy as well as minimized risks of systemic side effects. The introduction of nanotechnology in the treatment of lung diseases has allowed researchers to improve the bioavailability and pharmacokinetics of drugs when inside a biological entity, thereby overcoming several challenges in drug delivery. For example, in the treatment of COPD, drug delivery systems can be used to encapsulate antioxidants so as to combat oxidative stress which is involved in the pathogenesis of COPD [9]. Drug delivery vehicles, including microparticles and nanoparticles, have been known to achieve effective drug deposition and controlled release in the lungs. Presently, the use of drug-targeted delivery systems, namely liposomes, micelles, and nanoparticles, is highly effective in the delivery of therapeutic agents to specific sites in the lungs [10]. In addition, the encapsulation of drugs in polymeric delivery systems has been proven to protect the drugs from enzymatic degradation before reaching the specific site of action [11]. To effectively deliver drugs to the targeted site in the lung, some formulation properties, such as particle size, need to be considered during the preparation stage. At present, there has been much progress in the synthesis and application of drug delivery systems in pulmonary drug delivery. This article reviews the latest developments in the application of several novel drug delivery systems in pulmonary drug delivery. Furthermore, the main mechanisms in pulmonary drug administration, absorption, and clearance are also discussed. Challenges in the future clinical application of drug delivery vehicles are also highlighted.
Mechanisms of drug delivery, absorption, and clearance in the lungs
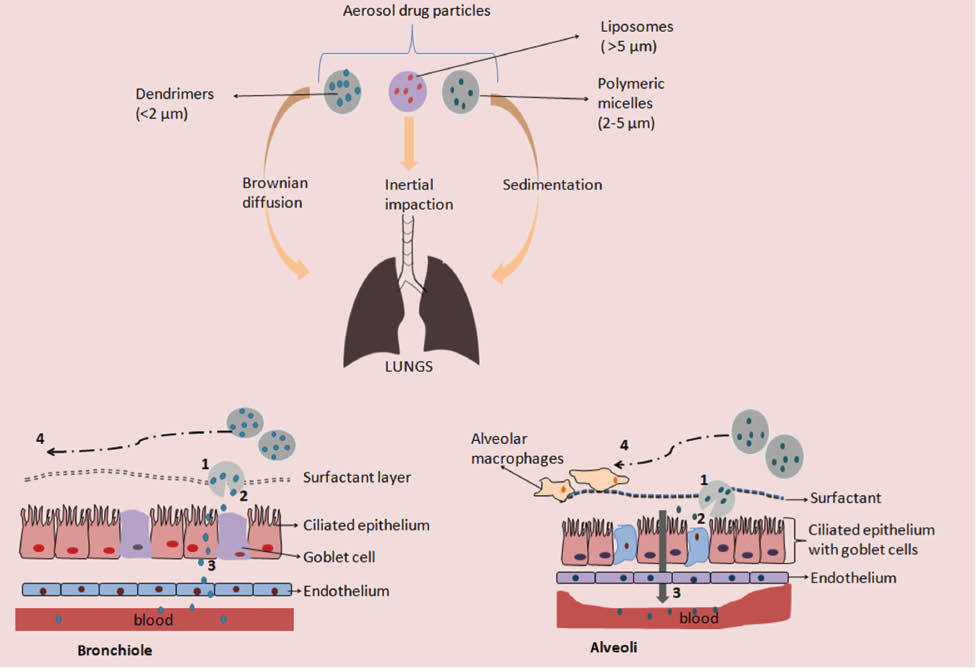
The lung is the organ of interest in pulmonary drug delivery. The physiological characteristics of the lungs, such as the large absorptive surface area, highly influence the drug absorption in the pulmonary system [4]. Additionally, the enzymatic metabolic activity in the lungs, which is significantly low and the presence of a thin alveolar epithelium (~0.2–0.5 μm thick) are also favorable for rapid drug absorption [12, 13]. Proper selection of the type of device to be used in the pulmonary delivery of various drug formulations is crucial to ensure effective drug deposition in the lungs. Devices used in the delivery of drugs via inhalation route include nebulizers [14], dry-powder inhalers, and pressurized meter dose inhalers [15]. More importantly, various factors influence the availability of therapeutic drugs in the lungs following their administration via the pulmonary route. The deposition of drug particles in the respiratory system is also determined by their physicochemical properties such as size and density. The main mechanisms that occur following inhalation of particles include inertial impaction, sedimentation, and Brownian diffusion [16, 17]. The deposition pattern is dependent on the size of particles, which is expressed as an aerodynamic diameter. The particle size also affects how deep in the lungs the inhaled particles can be deposited. Larger particles (>6 μm) get deposited in the upper airways (trachea) by inertial impaction, whereas those ranging from 2 to 5 μm are deposited in the bronchioles by sedimentation. Smaller particles (<2 μm) get deposited in the alveoli by Brownian diffusion [18] (Figure 1).
Figure 1 Mechanism of drug delivery in the lungs.
1. Penetration of the drug encapsulated system into the lung surfactant layer.
2. Controlled drug release of drug particles from the delivery system.
3. Absorption of drug particles across the pulmonary epithelium.
4. Clearance of unabsorbed drug particles by mucociliary clearance in the upper airways and phagocytosis by alveolar macrophages in the alveoli.
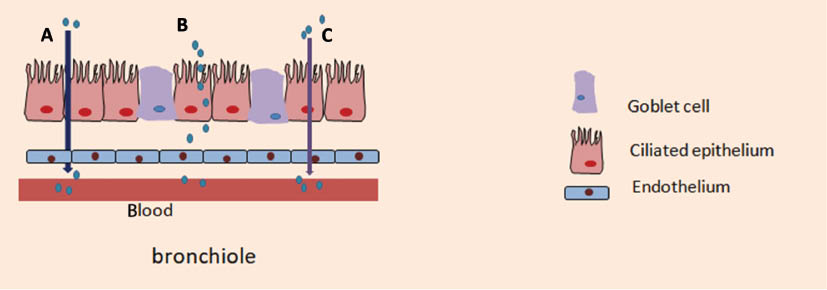
Following deposition in the lungs, drug particles dissolve in the lung epithelial lining prior to absorption across the epithelium through various transport mechanisms, as summarized in Figure 2. The most common transport pathway in drug absorption in the lungs is the transcellular pathway (absorption through cells). This transport mechanism involves drug absorption through both passive diffusion and receptor-mediated drug transport [19]. Transmembrane transporters such as ATP-binding cassettes (ABC) and solute-linked transporters also play a role in the absorption, distribution, and elimination of therapeutic agents in the lung [20]. Some drug particles can also be absorbed through the paracellular transport mechanism (between adjacent cells) [21].
Figure 2 Transport mechanisms of drug particles across the lung epithelium.
A. Paracellular absorption of hydrophilic drug particles.
B. Absorption of larger drug particles by endocytosis.
C. Transcellular absorption of lipophilic drug particles.
Drug clearance mechanisms in the lungs can be a limitation in the efficacy of inhaled drugs. The main clearance mechanism in the lung involves the phagocytosis of drug particles by the alveolar macrophages [6]. The lung has its own defense mechanism against foreign materials and protects the airways from being exposed to them by phagocytic and mucociliary clearance. Although this may be a protective mechanism, it also appears to be a barrier in the effective delivery of therapeutic agents to the lungs [22]. The epithelial cells act as a barrier against foreign inhaled materials [23]. Drug clearance mechanisms differ according to the location of the deposited drugs in the lung. Particles deposited in the conducting airway region are mainly eliminated by mucociliary clearance whereas those deposited in the respiratory part are mostly cleared by alveolar macrophage clearance [24]. Transepithelial transport is also a clearance mechanism for inhaled soluble particles in the alveoli [25]. Taken together, various ways in modifying drug delivery vehicles to reduce drug clearance and achieve efficient drug delivery and successful drug deposition in the lungs should be addressed in future studies. Presently, coating the drug delivery vehicles with polymers such as chitosan is known to improve their mucoadhesive properties and increase their stability in vivo.
Pulmonary drug administration can be achieved through various mechanisms, which include intratracheal instillation, inhalation, and nebulization (Table 1). The main types of devices commonly used in delivering drugs as aerosols include dry-powder inhalers, pressurized metered-dose inhalers, and nebulizers [14]. Compared with the dry-powder and metered-dose inhalers, nebulizers have been known to achieve drug administration in larger doses. However, this may result in an extended administration time [30]. Pressurized metered-dose inhalers have been widely used owing to their effectiveness in achieving delivery of aerosols and have also shown to be portable devices that can deliver a fixed amount of drug formulation [1]. Dry-powder inhalers have been successfully used in the delivery of aerosol drugs in higher concentration in the airways, for the treatment of COPDs, and have been known to achieve minimized systemic toxicity [31]. The extent of drug particle deposition as aerosols is mainly influenced by the type of device used and formulation [32]. Therefore, to achieve maximum concentrations of drug particles at the specific site, careful selection of the device to be used and the physicochemical properties of the drug particles have to be carefully considered.
Table 1 Mechanisms in Pulmonary Drug Administration
| Route of administration | Device used | Type of drug delivery system administered | Aim of study | Outcome | Reference |
|---|---|---|---|---|---|
| Inhalation | Dry-powder inhaler, soft-mist inhaler, pressurized metered-dose inhaler | Nanoliposomal salbutamol sulfate | Evaluation of dry-powder inhalation of salbutamol sulfate liposomes in treatment of asthma | Liposomal dry-powder inhalers achieved a prolonged drug release in vitro which lasted up to 14 hours. They also exhibited an excellent aerosol performance. | [26] |
| Intratracheal instillation | Polyvinylpyrrolidone-coated AgNPs | Evaluation of silver biodistribution following intratracheal instillation of nanoparticles | More silver ions were detected in the lungs of mice exposed to smaller AgNPs (5 nm), whereas higher concentration of silver was detected in the blood in mice exposed to larger AgNPs (50 nm). | [27] | |
| Doxorubicin-conjugated dendrimers | Effect of doxorubicin dendrimers in enhancing drug exposure to lung resident tumors | 7 days after intratracheal administration of doxorubicin dendrimers in rats, approximately 15% of the drug dose could still be detected in the lungs, suggesting that the dendrimers complex achieved a prolonged retention time. | [28] | ||
| Nebulization | Air-jet nebulizer, actively vibrating mesh nebulizer, passively vibrating-mesh nebulizer | Beclometasone dipropionate-loaded dendrimers | Evaluation of PAMAM dendrimers in the pulmonary delivery of beclometasone dipropionate | Air-jet and active mesh nebulizers achieved excellent delivery of PAMAM dendrimers. Nebulization analysis data indicated that aerosol properties of the beclometasone dipropionate-loaded dendrimers were influenced by the type of nebulizer used. | [29] |
AgNPs, silver nanoparticles; PAMAM, poly(amidoamine).
Types of novel drug delivery systems
The application of novel drug delivery systems has gained much attention in the treatment of pulmonary diseases. In the last decade, the concept of drug-targeted delivery has been investigated in the treatment of various pulmonary diseases and has proved to be a promising route in the delivery of drugs to the desired specific sites. Drug delivery systems are materials that include liposomes, nanoparticles, polymeric micelles, microparticles, and dendrimers among others that are used in the delivery of therapeutic agents to targeted sites [33]. The preparation techniques used vary depending on the carrier type, as summarized in Table 2. These delivery vehicles have shown to be highly effective in the treatment of various pulmonary diseases, including asthma and COPDs. Their unique features such as enhanced stability and small size range enable them to effectively deliver both hydrophilic and hydrophobic drugs to the targeted sites. They have the ability to achieve drug deposition in the lung, improve the rate of drug uptake by the targeted cells, and achieve high drug efficacy. Drug delivery vehicles are highly effective in the treatment of several lung diseases owing to their ability to achieve maintained therapeutic concentrations over a prolonged time. The application of these vehicles results in a reduced dosing frequency.
Table 2 Summary of Drug Delivery Systems Used in Pulmonary Drug Delivery
| Carrier type | Composition | Preparation technique | Model drug | Advantages | References |
|---|---|---|---|---|---|
| Liposomes | Consist of phospholipid bilayers | Film hydration method, pH gradient method, Surface coating using polymers such as chitosan | Ibuprofen, diazepam, midazolam | Can be used in the delivery of both hydrophobic and hydrophilic drugs and they improve drug solubility | [35, 36] |
| Micelles | Consist of phospholipids with hydrophobic core and hydrophilic head groups on the outer region | Thin-film hydration method, solvent evaporation method | Insulin | Polymeric micelles are stable in vivo and have the ability to dissolve several drugs with poor solubility | [37] |
| Microparticles | Consist of synthetic or natural polymers (glyceryl trimyristate and soy lecithin) | Hot solvent diffusion method, Hot homogenization method | Quercetin | Protect the encapsulated drugs from enzymatic degradation | [38] |
| Solid lipid nanoparticles | Consists of solid lipids, e.g., triglycerides, fatty acids (glycerol palmitostearate and polysorbate) | melted homogenization technique | Paclitaxel | Can encapsulate lipophilic drugs, with high biocompatibility | [39] |
| Inorganic nanoparticles | Consists of inorganic materials such as silicon oxide and calcium phosphate or metals such as gold. | Citrate reduction method | Zinc oxide | Gold nanoparticles have high drug loading capacity and can achieve surface modification with targeting ligands | [40] |
| Polymeric nanoparticles | Consists of polymeric materials such as PEG and chitosan | Ionic gelation method | Rhodamine-conjugated erythropoietin | Can achieve surface modification with ligands for targeted drug delivery | [9, 41] |
| Dendrimers | PAMAM, PEG, polylysine | Direct PEGylation, two-step PEGylation, co-solvent-free method | Doxorubicin | Can be effectively used as absorption enhancers, small in size compared with other nanoparticles, and can effectively penetrate epithelial barrier and achieve tumor penetration | [42, 43] |
PEG, polyethylene glycol; PAMAM, poly(amidoamine).
In addition, these delivery systems improve drug solubility, dissolution, and bioavailability. More importantly, they play a vital role in minimizing the toxicity of the encapsulated drug molecules and also extend the amount of time the drug resides in the targeted site [34]. Various materials, including polymers, polysaccharides, and proteins are widely used in the preparation of these delivery systems.
Liposomes
Liposomes are a type of drug delivery systems that are made up of one or more phospholipid bilayers. According to their size and number of bilayers, liposomes can be classified into small unilamellar vesicles, large unilamellar vesicles, and multilamellar vesicles [44]. To date, liposomes have been used as delivery vehicles in pulmonary drug delivery, owing to their ability to encapsulate both hydrophilic and hydrophobic therapeutic agents and maintain a controlled drug release profile at the targeted site [32]. When administered via the pulmonary route, liposomes can extend the residence time of the encapsulated drug in the lungs and achieve an enhanced local therapeutic drug effect with minimized systemic side effects; thus, they have been known to be promising nanocarriers in pulmonary drug delivery [45]. To ensure effective drug deposition in the lung, the particle size of the liposomal formulation should be maintained in the nano-size range. Lamellarity is one of the properties that affect the application of liposomes in pulmonary drug delivery; for example, the number of lamellae significantly affects the amount of therapeutic agent to be encapsulated in the liposomes. Both small and large unilamellar vesicles have a single lipid bilayer and work best in encapsulating lipophilic and hydrophilic compounds, respectively, with small unilamellar vesicles having a low aqueous core volume-to-lipid ratio, whereas large unilamellar vesicles have a large aqueous volume-to-lipid ratio [46]. Multilamellar vesicles consist of two or more lipid bilayers and have the ability to encapsulate various lipophilic compounds. These have been shown to work best in achieving a sustained release profile of the encapsulated compounds.
In a recent study, Chennakesavulu et al. designed dry-powder inhaler liposomes and further investigated their efficacy in the pulmonary delivery of budesonide and colchicine for the treatment of idiopathic pulmonary fibrosis. A sustained drug release profile for up to 24 hours following administration of the liposomal formulation was observed. From this study, it can be concluded that the composition of the liposomal membrane and the concentration of the drug trapped in the liposomes greatly influence the diffusion rate of the drug upon reaching the targeted site [47]. Current studies have also shown that the concept of surface modification of liposomes by polyethylene glycol (PEG) significantly enhances their stability in vivo. PEG is one of the most preferred polymers that have been widely used in polymer-based drug delivery due to its high biocompatibility as well as its ability to prolong drug residence time in biological systems [48]. The presence of PEG on the liposomal surface protects the liposomes from rapid degradation and phagocytosis in vivo, thereby leading to an extended systemic circulation period [49]. Lin et al. investigated the pulmonary delivery of triptolide-loaded liposomes with anti-carbonic anhydrase IX antibody (CA IX liposomes) for the treatment of lung cancer and found that a sustained drug release profile at the targeted site was achieved [50]. The liposomal formulation achieved direct drug delivery in the lungs, thereby leading to a higher concentration of drug accumulation in the targeted site and minimized systemic side effects.
In a previous study, Manconi et al. reported the effectiveness of liposomes coated with chitosan and hyaluronan in the delivery of curcumin in the lungs [51]. The liposomal surface modification with chitosan and hyaluronan significantly improved the bioavailability of curcumin. Moreover, the coating of liposomes with chitosan improved their mucoadhesive properties and prolonged their residence time in the airways. Several studies have also confirmed that when compared with uncoated liposomes, chitosan-coated liposomes can achieve an extended residence period in the pulmonary system [52]. Recent studies have shown that liposomes are an effective delivery vehicle in the pulmonary delivery of fluticasone. As evidenced by the in vivo biodistribution analysis, it was clearly shown that the amount of fluticasone encapsulated in liposomes that had accumulated in the lungs 3 hours after intranasal administration was approximately 30 times more compared to that of the free drug [53]. The in vitro test results also indicated that the fluticasone liposomes did not have any toxic effects on the A549 cells (alveolar epithelial cell lines). Recently, the pulmonary delivery of transferrin receptors, which target peptide surface-functionalized liposomes in the treatment of lung cancer, was investigated [54]. From both in vivo and in vitro data, it can be concluded that the T7 surface functionalized liposomes proved to be an effective drug delivery system in the treatment of lung cancer by receptor-mediated targeting at the tumor area.
Although the use of liposomes as carriers in pulmonary drug delivery has showed great benefits, there are some limitations involved, for example, drug leakage from the liposomes [55]. When drug-loaded liposomes are delivered to the lung as liquid dispersions via nebulization, the stability of vesicles can be reduced, and drug may also leak during nebulization [56]. To overcome these challenges, freeze drying has shown to be a potential method applied during the formulation preparation stage. Nevertheless, the need for more studies to investigate various ways of minimizing drug leakage and increasing vesicle stability remains an issue of concern in pulmonary drug delivery. Future studies can also focus on overcoming the current challenges encountered in the formulation of liposomes with much emphasis on the careful selection of materials to be used in modifying the liposomal surfaces so as to improve their stability.
Microparticles
Microparticles are particles ranging between 1 and 1000 μm that are used as drug delivery systems. They have been widely used in the field of respiratory therapy owing to their ability to achieve controlled drug release, enhanced drug loading properties, and biocompatibility. Moreover, their use in inhalation therapy has become an area of interest in pharmaceutical research. To achieve effective drug deposition into the lungs, their particle size should be in the range of 1 to 5 μm because those larger than 5 μm easily get deposited in the larynx and oropharynx [57].
Yildiz-Peköz et al. designed doripenem aerosolized microparticles using the ionotropic gelation and spray drying method, and further investigated their effectiveness in pulmonary drug delivery for the treatment of pneumonia. When compared to other micro particle formulations, the microparticles with 20% leucine showed the highest fine particle fraction ratio; thus, the presence of leucine significantly improved their aerosolization properties [58]. Additionally, for the microparticles with leucine, higher encapsulation efficiency was observed compared with the other formulations with lactose and trehalose. This indicates that the encapsulation efficiency of microparticles is also influenced by both the quantity and type of excipients used in the formulation. Therefore, proper selection of the types of excipients to be used in the preparation of microparticles is of paramount importance to achieve high encapsulation efficiency and effective pulmonary drug delivery.
In a recent study, the pulmonary delivery of azithromycin-loaded respirable microparticles was investigated for the treatment of pneumonia [59]. From the in vivo data, it was clearly shown that when compared with the intravenous and intragastric administration, the microparticle formulation that was administered via intratracheal insufflation achieved an extended retention time in the lungs, with a strong fluorescent intensity, 24 hours following administration. This further shows that administration of microparticles via the pulmonary route can significantly increase the amount of drug that accumulates in the lungs compared to the other routes of administration. Microparticles that consist of biocompatible polymers such as chitosan have been known to be stable, have mucoadhesive property, and can achieve controlled drug release in the targeted sites. However, the molecular weight of chitosan to be used must be thoroughly considered, since a high molecular weight (190–300 kDa) could possibly result in high toxic effects. On the contrary, low-molecular-weight (50–180 kDa) chitosan microparticles have been successfully used in the pulmonary delivery of isoniazid and proved to be nontoxic to the alveolar macrophage [60].
Spray-dried fucoidan microparticles were investigated for their effectiveness in pulmonary delivery of antitubercular drugs. The aerodynamic properties of the microparticles made them suitable for delivering antibiotics. The microparticles showed great potential in depositing the drugs directly to the alveoli, owing to their particle size that was within the suitable range (1–5 μm) [61]. Solid lipid microparticles have been used in encapsulating salmeterol xinafoate (SX) in the treatment of COPD [62]. When compared with the free drug, the SX-loaded microparticles were able to achieve an enhanced cAMP expression. The retention time of the drug in the lung was prolonged owing to the suitable aerodynamic diameter, drug loading efficiency, and mucoadhesive characteristics of the solid lipid microparticles, suggesting that they have a great potential as delivery vehicles in pulmonary drug delivery. Uneven dispersion of solid lipid particles will affect the drug’s deposition ability in the lungs. Particle-generating technologies is needed for the generation of particles with suitable aerodynamic diameter in order to achieve an even dispersion, thereby resulting in an effective drug deposition within the lungs.
In a similar study, Amore et al. analyzed the effectiveness of using chitosan and alginate mucoadhesive solid lipid microparticles in the pulmonary delivery of fluticasone propionate. Effective delivery and controlled release of fluticasone propionate into the secondary bronchi were achieved, mainly due to the suitable size and enhanced mucoadhesive properties of the microparticles [63].
Micelles
The development of inhalable nanocarriers such as micelles for lung cancer therapy has become an area of interest in biomedical research. Polymeric micelles are a type of drug delivery systems that are formed from several block polymers, with the hydrophobic part as the interior region and the hydrophilic part as the outer region. They are spherical in shape and their size varies (∼10–100 nm) [64]. They have been known to be promising nanocarriers in the pulmonary delivery of drugs for the treatment of respiratory diseases, owing to their ability to encapsulate both hydrophilic and hydrophobic drugs. Hydrophobic drugs are enclosed in the interior region (core) whereas the hydrophilic drugs get attached on the outer region (shell) [65]. Shang et al. found that the pulmonary delivery of mycolic acid (MA)-loaded polymeric micelles could achieve induction of Mycobacterium tuberculosis lipid-specific T-cell responses in the lungs of hCD1Tg mice [66]. Unlike the intravenous route that could result in drug distribution to many organs, the intranasal route proved to be effective, as it could mainly target the lungs and achieve a high amount of drug accumulation in the lungs. In vitro data also confirmed that when compared with the free drug, the MA-loaded micelles showed high efficacy in activating MA-specific TCR transgenic (DN1) T cells.
It has also been discovered that introducing some modifications in the micelle formulation could enhance their drug delivery properties further. For example, in the preparation of inhalable powders containing polymeric micelles, micelles can be incorporated in lactose carriers by spray drying to enhance the maximal delivery of therapeutic agents in the alveoli [67]. Lactose carriers are nontoxic and also degradable; thus, they are recommended as excipients for use in polymeric micelle formulation [68]. When curcumin acetate-loaded micelles were delivered to rats by intratracheal administration, a higher concentration of curcumin acetate was detected in the lungs compared with the lower concentration detected following intravenous administration [69]. In addition, following the intratracheal administration of the micelle formulation, a sustained drug release profile and an extended drug retention time in the lungs were achieved. These findings show that when compared with other routes of administration, the intratracheal delivery of micelles facilitates drug uptake in the pulmonary tract.
Polymeric micelles have been used in the preparation of powders for pulmonary delivery of insulin. Previous studies have been reported that the aerosolization properties (e.g., fine particle fraction) of these powders differ, depending on the polymer used in the formulation [70]. When PEG is added in the micelle formulation, it improves the mucus-penetrating properties, thereby achieving effective deposition of insulin in the lung as well as its absorption in the bronchial region.
One of the main limitations in using micelles as drug carriers in pulmonary delivery is that due to their small size, they can be exhaled from the respiratory system, leading to failure in achieving drug deposition in the deeper regions of the lung [68]. Future studies can focus on modification strategies for micelle formulations to prevent their exhalation from the respiratory tract prior to achieving drug delivery to the targeted sites.
Nanoparticles
Nanoparticles have been widely used in drug delivery owing to their ability to overcome systemic barriers and deliver encapsulated drugs to the targeted sites [71]. More importantly, understanding the physicochemical properties of nanoparticles can result in the production of safe nanoparticles since their extent of toxicity in biological systems is largely influenced by these properties [72]. Their nano-size range enables them to easily penetrate the biological systems and deliver drugs to the specific sites [64]. Nanoparticles can be modified to enhance their drug delivery properties; for instance, they can be coated with various polymers to improve their mucoadhesive properties. Further advancements have been accomplished in the use of biodegradable nanoparticles. Poly(lactic-co-glycolic acid) (PLGA) nanoparticles have been investigated in the pulmonary delivery of levofloxacin for the treatment of tuberculosis. More importantly, during the preparation stage, the amount of polymer added and the homogenization speed should be carefully considered because they significantly influence the particle size of the nanoparticles and their drug release properties. It was discovered that, the higher the amount of PLGA added, the larger the nanoparticle size and a higher homogenization speed led to a reduction in particle size [73]. With a mass median aerodynamic diameter of 4.4 μm, the nanoparticles were able to achieve effective lung penetration and controlled drug release. Therefore, the use of drug-loaded nanoparticles proved to be more effective, as evidenced by more drug accumulation in the targeted site and controlled drug release achieved. The pulmonary administration of nanoparticles in lung cancer therapy has been known to minimize systemic toxicity of anticancer drugs as they can achieve drug delivery to the targeted site [74]. To further enhance the specific interaction between tumor cells and the drug nanoparticles, the latter can be modified by the attachment of tumor-specific ligands [28]. This can also minimize toxicity and prevent interactions between the normal lung cells and the nanoparticles. Some of the challenges encountered in tumor penetration are a result of chemical and physical properties of nanoparticles. It has also been discovered that the shape of nanoparticles affects their fate in vivo (i.e., their penetration and cell uptake as well as their accumulation in the target site). It can be concluded that nanoparticle penetration capabilities differ according to their shapes [75, 76]. Surface charge is another property that affects the interaction between nanoparticles and tumor cells, with cationic nanoparticles known for easy adherence to tumor cells [77].
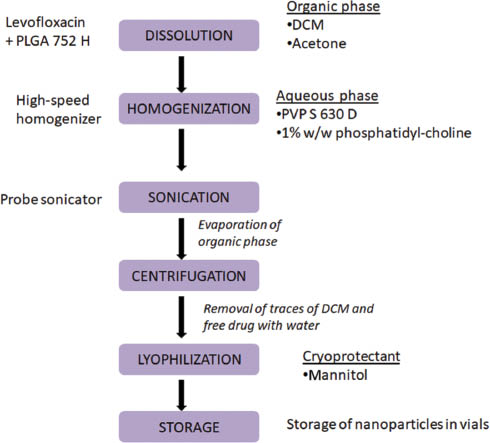
Chishti et al. designed optimized docetaxel-loaded nanoparticles (DTX-NPs) and investigated their effectiveness in the treatment of non-small cell lung cancer [78]. In vivo analysis data showed the presence of docetaxel in the lungs 72 hours following pulmonary administration of DTX-NPs, whereas the free drug had been cleared at approximately 8 hours after administration. This indicates that nanoparticles play a major role in achieving a prolonged drug retention time in the targeted site. Taken together, both in vitro and in vivo data confirmed that controlled drug release was maintained when DTX-NPs were administered. During the synthesis of nanoparticle formulations, the type of preparation technique used is of paramount importance in achieving effective drug delivery to the targeted site. In the preparation of levofloxacin nanoparticles (Figure 3), the homogenization speed and the amount of PLGA added were shown to have a significant effect on the mean particle size and drug release [73].
Figure 3 Preparation of levofloxacin nanoparticles for pulmonary drug delivery [83].
Chitosan is a natural polymer that has been widely used in the preparation of nanoparticles. Chitosan nanoparticles are known to be effective in the delivery of therapeutic agents via pulmonary route owing to their high compatibility, enhanced encapsulation, and ability to resist enzyme degradation. From in vivo pharmacokinetic analysis results, a higher concentration of bedaquiline accumulated in the lungs following pulmonary administration of bedaquiline-loaded chitosan nanoparticles compared to the free drug. For the cell viability assay using J774 macrophage cell line, the freeze-dried bedaquiline-loaded nanoparticles showed 90% cell viability for 24 hours, indicating the safeness of the nanoparticle formulation [79]. In a similar study, low-molecular-weight chitosan-coated PLGA nanoparticles were investigated in pulmonary delivery of tobramycin for cystic fibrosis treatment [80]. Low-molecular-weight chitosan was used to coat PLGA nanoparticles to improve their mucoadhesive properties, enhance drug deposition, and prolong their retention time in the lungs. The particle size of the nanoparticles was influenced by the concentration of chitosan added in the formulation. An increase in concentration of chitosan was linked to an increase in the particle size. However, there are some drawbacks that may be encountered as a result of adding chitosan as an excipient in nanoparticle formulation. For instance, the incompatibility of chitosan with some biological fluids can result in particle degradation. To overcome this challenge, polypeptides can be added to the chitosan nanoparticle formulation [81].
Although inorganic nanoparticles have been used in the targeted drug delivery to the lungs, they have also been discovered to result in toxic effects in biological systems, for example, lung inflammation [82, 83]. Roda et al. discovered lung injury patterns in rats, 7 days after intratracheal administration of silver nanoparticles (AgNPs) [84]. In a similar study, pulmonary administration of citrate-coated 20 nm AgNPs resulted in a high level of acute lung inflammation as a result of their rapid dissolution rate compared with the 110-nm particles suggesting that the size and dissolution rate of AgNPs has a significant effect on the extent of potential pulmonary injury [85]. Hamilton et al. used transmission electron microscopy and also confirmed the high dissolution rate of two types of smaller (20 nm) AgNPs (PVC- and citrate-coated) compared with the larger ones (110 nm). As evidenced by the analysis results, the 20-nm AgNPs resulted in higher toxicity in the epithelial cell lines [86]. It is still unclear if coating the surfaces of AgNPs has a significant effect in reducing their toxicity; therefore, more studies are needed to investigate the effect of coating AgNPs with different materials in minimizing their toxicity.
Dendrimers
Dendrimers are highly defined, branched polymeric materials in the nano-size range that can be used in various applications, for example, in the medical field, particularly in drug delivery, owing to their distinctive properties such as their branching and high biocompatibility [87, 88]. They have been used as nanocarriers in drug delivery owing to their ability to improve the bioavailability of drugs and to achieve controlled drug release at the targeted sites [87]. Structurally, they mainly consist of three components, which are the central core, branches, and terminal groups [89]. Their shapes differ mainly depending on their generation numbers (branching points). To enhance the drug delivery properties, dendrimer surface can be modified by various procedures such as PEGylation and acetylation [90]. Addition of various excipients such as PLGA during the preparation stage also results in several benefits in pulmonary drug delivery (Table 3). Dendrimers are small in size compared with other nanoparticles and can therefore be used as drug delivery systems to achieve tumor penetration [91]. Poly(amidoamine) (PAMAM) dendrimers have been successfully used as carriers in the delivery of proteins and nucleic acids to specific sites [92, 93].
Table 3 Effects of Various Excipients in the Preparation of Drug Carrier Formulations
| Excipient agents | Effects | Carrier type | Reference |
|---|---|---|---|
| Polylactide-PEG-polylactide | Improves the lung deposition of the dendrimer formulation | Dendrimers | [97] |
| Chitosan | A highly biocompatible and biodegradable polymer that extends the residence time of drug carriers in the pulmonary system | Liposomes | [101] |
| Low-molecular-weight chitosan improves the mucoadhesiveness of the microparticle formulation | Microparticles | [60] | |
| PLGA | Biodegradable polymer that improves the mucoadhesive property of the drug delivery vehicles | Nanoparticles | [73] |
| Maintains sustained drug release in the pulmonary system | |||
| PEG | Its presence on the liposomal surface protects the liposomes from phagocytosis and rapid degradation and improves their circulation time | Liposomes | [49] |
| Increases the stability of drug delivery vehicles and minimizes drug particle aggregation by steric stabilization in vivo. | Micelles | [102] | |
| Lactose | Reduces drug particle aggregation and improves deposition of the aerosolized drug particles | Microparticles | [103] |
| Trehalose | Prevents drug particle aggregation | Microparticles | [58] |
| Leucine | Enhances the aerosolization properties of the microparticles | Microparticles | [104] |
PEG, polyethylene glycol; PLGA, poly(lactic-co-glycolic acid).
Pulmonary delivery of siRNA-targeting tumor necrosis factor α (TNF-α) using third-generation PAMAM dendrimers as transfection agents was investigated by Bohr et al. PAMAM dendrimers were used to deliver siRNAs to the lungs and their effect on induction of gene silencing in the lung was examined in a murine acute lung inflammation model. Mice treated with the non-complexed TNF-α siRNA resulted in 2% TNF-α silencing 4 hours after mice exposure to lipopolysaccharide, whereas mice treated with dendriplex TNF-α siRNA showed a higher TNF-α silencing of 24%, thereby confirming the effective delivery of siRNAs to the lungs when a transfection agent is used [94]. However, these dendrimers achieved a rapid response in the inhibition of TNF-α that only lasted for a short time that could be associated with their low stability as well as elimination of the dendriplex TNF-α siRNAs by mucociliary clearance. To improve the stability of this dendrimer formulation, higher-generation dendrimers could have been used, but the main challenge that could have resulted was that of increased toxicity. Therefore, future studies may focus on evaluating various ways to improve stability of dendrimers with minimized toxicity.
Previous studies have shown that PAMAM dendrimers can improve pulmonary drug absorption of peptide and protein drugs that are known to be poorly absorbed due to their weak membrane permeability properties [95]. PAMAM dendrimers can therefore be effectively used as absorption enhancers. Yan et al. investigated the pulmonary absorption of insulin using different levels of caproyl-modified G2 PAMAM dendrimer (G2-AC) as absorption enhancers. It was discovered that G2-AC6 dendrimers were able to cross the epithelial barrier through both paracellular and transcellular transport routes and enhanced insulin absorption at low concentrations without any pulmonary membrane damage [96]. In a similar study, when doxorubicin was conjugated to PAMAM dendrimers, its transportation across the pulmonary epithelium was significantly improved compared to with the free drug. Furthermore, the surface modification of these dendrimers by addition of PEG also enhanced their penetration in the pulmonary epithelium [97].
The mechanism of pulmonary administration also influences the extent of effective delivery of drugs to the targeted site. Three types of nebulizers with different operation techniques were investigated in the pulmonary delivery of beclometasone dipropionate (BDP)-loaded dendrimers and differences in the aerosol properties of the BDP-dendrimer complexes were discovered. The aerosol output analysis results indicated that the dendrimer formulations (different generations) had no effect on the aerosol output; instead, the output performance of dendrimer complexes differed depending on the type of nebulizer used [29]. When polylysine dendrimers modified with different sizes of PEG groups were administered in rats through inhalation, their absorption into the systemic circulation differed depending on their sizes. Larger dendrimers resulted in prolonged drug retention in the lungs for up to 1 week, but the absorption into the blood was poor compared with the small dendrimers, which were well absorbed, although their retention in the lungs was limited [98]. This also indicates that the level of PEGylation has a significant influence on the breakdown and absorption of dendrimers in the lungs. Similar studies have also showed the relationship between the rate of absorption and molecular weight of drug carriers with larger carriers being absorbed at a slower rate compared with the smaller ones [21, 99].
Although dendrimers have been widely used for targeted drug delivery, they also have some disadvantages that limit their roles as drug delivery vehicles, which include poor encapsulation for some therapeutic agents in the dendrimer cavities as well as cytotoxicity [100].
Challenges in the clinical application of drug delivery systems
Limitations in large-scale manufacturing of drug delivery systems could be a challenge in their clinical application in the future. For example, in combination therapy, the process of encapsulating more than one drug into a single nano-sized drug carrier is complicated and involves a series of steps, which make large-scale production difficult and also results in an increase in production cost. Furthermore, nanomedicine-based therapy is very expensive due to the high cost of the raw materials used in the manufacturing process. Advancements in the exploration and use of innovative manufacturing processes will play a major role in improving the industrial large-scale manufacturing as well as clinical application of these drug delivery vehicles [105, 106].
Some of the challenges likely to be encountered in the future clinical application of these drug delivery systems include the potential cytotoxic effects. For example, in the application of liposomes, drug leakage from the liposomal formulation can result in high risks of systemic toxicity. In addition, it has also been discovered in some studies that charged liposomes can be toxic [107]. Such drawbacks will also limit the successful market developments. Nanomedicine toxicity concerns could also limit the clinical application of nanoparticles. Ensuring the safety of nanoparticle-based drug delivery in inhalation therapy could also be one of the major challenges in the future clinical application. To improve the nanomedicine safety features, in vivo toxicity assessment should be carefully designed and should also focus more on toxicokinetics and other aspects that are not fully assessed in the in vitro experiments
Although there have been great results in the use of nanoparticles in preclinical experiments, the clinical application of nanomedicine may possibly result in a reduced success rate, due to the variations in species-dependent physiological and pathological processes in animal models and humans [105, 108]. To improve the correlation between preclinical and clinical trials in the application of nanoparticles, animal-based disease models that are more similar to the human pathophysiological mechanisms should be used.
Conclusion
Pulmonary drug delivery is one of the most preferred routes of administration, as it is offers a wide range of benefits over other routes of drug administration. Additionally, first-pass metabolism is avoided, making it an even more promising route in targeting the lungs. The application of drug delivery systems in pulmonary drug delivery offers a number of advantages, which include controlled drug release at the specific targeted sites, prolonged drug retention time, and reduced side effects in the untargeted regions, and is has also been shown to result in great improvements in treatment outcomes. Surface modification of these drug delivery vehicles is a promising strategy widely used in protecting the encapsulated drugs from rapid degradation, for example, the use of chitosan in coating nanoparticles to improve their mucoadhesive properties. To date, low-molecular-weight chitosan can be recommended as an excipient, to prevent the toxic effects that may possibly occur following the use of high-molecular-weight chitosan. Several studies in pharmaceutical research have highlighted that the amount of polymer added during the preparation stage should be carefully considered, as it significantly influences the particle size. Moreover, encapsulation efficiency of these delivery systems depends on the type of excipients used; therefore, selection of the types of excipients and polymers to be used in the preparation of drug delivery systems should be carefully considered to achieve effective drug delivery to the lungs. Although the use of novel drug delivery systems has been proven to improve pulmonary drug delivery, there are still some drawbacks encountered. The leakage of encapsulated drug particles from some of these drug delivery vehicles especially in liposomal formulations still remains a major limitation in pulmonary drug delivery. Therefore, in future studies, researchers can address the various ways to overcome drug leakage from the drug delivery vehicles to ensure maximum drug deposition in the lungs, minimize drug toxic effects, and achieve effective treatment of pulmonary diseases in clinical application.
Acknowledgments
This research was supported by the National Natural Science Foundation of China (grant nos. 81903551, 81772316, and 81803443], Zhejiang Province Natural Science Foundation (grant nos. LY19H180001, LQ19H300001, and LY20H300002], and Zhejiang Provincial Program for the Cultivation of High-level Innovative Health Talents, Wenzhou Municipal Science and Technology Bureau (to Y.Z. Zhao; grant no. Y20190177].
Declaration of Interest
All authors involved in this article declare that there is no conflict of interest regarding the publication of this paper
References
- Chandel A, Goyal AK, Ghosh G, Rath G. Recent advances in aerosolised drug delivery. Biomed Pharmacother 2019;112:108601. [PMID: 30780107 DOI: 10.1016/j.biopha.2019.108601]
- Borghardt JM, Kloft C, Sharma A. Inhaled therapy in respiratory disease: the complex interplay of pulmonary kinetic processes. Can Respir J 2018;2018:2732017. [PMID: 30018677 DOI: 10.1155/2018/2732017]
- Fontana MC, Laureano JV, Forgearini B, Dos Santos J, Pohlmann AR, et al. Spray-dried raloxifene submicron particles for pulmonary delivery: development and in vivo pharmacokinetic evaluation in rats. Int J Pharm 2020;585:119429. [PMID: 32470484 DOI: 10.1016/j.ijpharm.2020.119429]
- Patil JS, Sarasija S. Pulmonary drug delivery strategies: a concise, systematic review. Lung India 2012;29:44-9. [PMID: 22345913 DOI: 10.4103/0970-2113.92361]
- Garrastazu Pereira G, Lawson A, Buttini F, Sonvico F. Loco-regional administration of nanomedicines for the treatment of lung cancer. Drug Deliv 2016;23:2881-96. [PMID: 26585837 DOI: 10.3109/10717544.2015.1114047]
- Mangal S, Gao W, Li T, Zhou Q. Pulmonary delivery of nanoparticle chemotherapy for the treatment of lung cancers: challenges and opportunities. Acta Pharmacol Sin 2017;38:782-97. [PMID: 28504252 DOI: 10.1038/aps.2017.34]
- Guo H, Hou Y, Ding J. Nanomedicines for intravesical chemotherapy in bladder cancer. Curr Pharm Des 2019;25:371-3. [PMID: 31215365 DOI: 10.2174/138161282504190516080607]
- Jahangirian H, Lemraski EG, Webster TJ, Rafiee-Moghaddam R, Abdollahi Y. A review of drug delivery systems based on nanotechnology and green chemistry: green nanomedicine. Int J Nanomed 2017;12:2957-78. [PMID: 28442906 DOI: 10.2147/IJN.S127683]
- Xu Y, Liu H, Song L. Novel drug delivery systems targeting oxidative stress in chronic obstructive pulmonary disease: a review. J Nanobiotechnol 2020;18:145. [PMID: 33076918 DOI: 10.1186/s12951-020-00703-5]
- Smola M, Vandamme T, Sokolowski A. Nanocarriers as pulmonary drug delivery systems to treat and to diagnose respiratory and non respiratory diseases. Int J Nanomedicine 2008;3:1-19. [PMID: 18488412 DOI: 10.2147/IJN.S1045]
- Beck-Broichsitter M, Merkel O, Kissel T. Controlled pulmonary drug and gene delivery using polymeric nano-carriers. J Control Release 2012;161:214-24. [PMID: 22192571 DOI: 10.1016/j.jconrel.2011.12.004]
- Zhou Y, Niu B, Wu B, Luo S, Fu J, et al. A homogenous nanoporous pulmonary drug delivery system based on metal-organic frameworks with fine aerosolization performance and good compatibility. Acta Pharm Sin B 2020;10:2404-16. [PMID: 33354510 DOI: 10.1016/j.apsb.2020.07.018]
- Agu RU, Ugwoke MI, Armand M, Kinget R, Verbeke N. The lung as a route for systemic delivery of therapeutic proteins and peptides. Respir Res 2001;2:198-209. [PMID: 11686885 DOI: 10.1186/rr58]
- Ibrahim M, Verma R, Garcia-Contreras L. Inhalation drug delivery devices: technology update. Med Devices (Auckland, NZ) 2015;8:131-9. [PMID: 25709510 DOI: 10.2147/MDER.S48888]
- Goel A, Baboota S, Sahni J, Ali J. Exploring targeted pulmonary delivery for treatment of lung cancer. Int J Pharm Invest 2013;3:8-14. [PMID: 23799201 DOI: 10.4103/2230-973X.108959]
- Jin X, Song L, Ma C, Zhang Y, Yu S. Pulmonary route of administration is instrumental in developing therapeutic interventions against respiratory diseases. Saudi Pharm J 2020;28:1655-65. [PMID: 33424258 DOI: 10.1016/j.jsps.2020.10.012]
- Darquenne C. Deposition mechanisms. J Aerosol Med Pulm Drug Deliv 2020;33:181-5. [PMID: 32598200 DOI: 10.1089/jamp.2020.29029.cd]
- Chaurasiya B, Zhao Y. Dry powder for pulmonary delivery: a comprehensive review. Pharmaceutics 2020;13:31. [PMID: 33379136 DOI: 10.3390/pharmaceutics13010031]
- Ibrahim M, Garcia-Contreras L. Mechanisms of absorption and elimination of drugs administered by inhalation. Ther Deliv 2013;4:1027-45. [PMID: 23919477 DOI: 10.4155/tde.13.67]
- Nickel S, Clerkin CG, Selo MA, Ehrhardt C. Transport mechanisms at the pulmonary mucosa: implications for drug delivery. Expert Opin Drug Deliv 2016;13:667-90. [PMID: 26909544 DOI: 10.1517/17425247.2016.1140144]
- Patton JS, Fishburn CS, Weers JG. The lungs as a portal of entry for systemic drug delivery. Proc Am Thorac Soc 2004;1:338-44. [PMID: 16113455 DOI: 10.1513/pats.200409-049TA]
- Loira-Pastoriza C, Todoroff J, Vanbever R. Delivery strategies for sustained drug release in the lungs. Adv Drug Deliv Rev 2014;75:81-91. [PMID: 24915637 DOI: 10.1016/j.addr.2014.05.017]
- Magalhães J, Pinheiro M, Drasler B, Septiadi D, Petri-Fink A, et al. Lipid nanoparticles biocompatibility and cellular uptake in a 3D human lung model. Nanomedicine (Lond) 2020;15:259-71. [PMID: 31789097 DOI: 10.2217/nnm-2019-0256]
- Liu Q, Guan J, Qin L, Zhang X, Mao S. Physicochemical properties affecting the fate of nanoparticles in pulmonary drug delivery. Drug Discov Today 2020;25:150-9. [PMID: 31600580 DOI: 10.1016/j.drudis.2019.09.023]
- Wittekindt OH. Tight junctions in pulmonary epithelia during lung inflammation. Pflugers Arch 2017;469:135-47. [PMID: 27921210 DOI: 10.1007/s00424-016-1917-3]
- Honmane S, Hajare A, More H, Osmani R, Salunkhe S. Lung delivery of nanoliposomal salbutamol sulfate dry powder inhalation for facilitated asthma therapy. J Liposome Res 2019;29:332-42. [PMID: 30296863 DOI: 10.1080/08982104.2018.1531022]
- Rosário F, Duarte I, Pinto R, Santos C, Hoet P, et al. Biodistribution and pulmonary metabolic effects of silver nanoparticles in mice following acute intratracheal instillations. Environ Sci Pollut Res Int 2021;28:2301-14. [PMID: 32885333 DOI: 10.1007/s11356-020-10563-z]
- Kaminskas L, McLeod V, Ryan G, Kelly B, Haynes J, et al. Pulmonary administration of a doxorubicin-conjugated dendrimer enhances drug exposure to lung metastases and improves cancer therapy. J Control Release 2014;183:18-26. [PMID: 24637466 DOI: 10.1016/j.jconrel.2014.03.012]
- Nasr M, Najlah M, D’Emanuele A, Elhissi A. PAMAM dendrimers as aerosol drug nanocarriers for pulmonary delivery via nebulization. Int J Pharm 2014;461:242-50. [PMID: 24275446 DOI: 10.1016/j.ijpharm.2013.11.023]
- Hess D. Nebulizers: principles and performance. Respir Care 2000;45:609-22.
- Onoue S, Misaka S, Kawabata Y, Yamada S. New treatments for chronic obstructive pulmonary disease and viable formulation/device options for inhalation therapy. Expert Opin Drug Deliv 2009;6:793-811. [PMID: 19558334 DOI: 10.1517/17425240903089310]
- Elhissi A. Liposomes for pulmonary drug delivery: the role of formulation and inhalation device design. Curr Pharm Des 2017;23:362-72. [PMID: 27848886 DOI: 10.2174/1381612823666161116114732]
- Vega-Vásquez P, Mosier NS, Irudayaraj J. Nanoscale drug delivery systems: from medicine to agriculture. Front Bioeng Biotechnol 2020;8:79. [PMID: 32133353 DOI: 10.3389/fbioe.2020.00079]
- Keshavarz A, Alobaida A, McMurtry IF, Nozik-Grayck E, Stenmark KR, et al. CAR, a homing peptide, prolongs pulmonary preferential vasodilation by increasing pulmonary retention and reducing systemic absorption of liposomal fasudil. Mol Pharm 2019;16:3414-29. [PMID: 31194563 DOI: 10.1021/acs.molpharmaceut.9b00208]
- Khadke S, Stone P, Rozhin A, Kroonen J, Perrie Y. Point of use production of liposomal solubilised products. Int J Pharm 2018;537:1-8. [PMID: 29225099 DOI: 10.1016/j.ijpharm.2017.12.012]
- Carugo D, Bottaro E, Owen J, Stride E, Nastruzzi C. Liposome production by microfluidics: potential and limiting factors. Sci Rep 2016;6:25876. [PMID: 27194474 DOI: 10.1038/srep25876]
- Andrade F, Fonte P, Oliva M, Videira M, Ferreira D, et al. Solid state formulations composed by amphiphilic polymers for delivery of proteins: characterization and stability. Int J Pharm 2015;486:195-206. [PMID: 25818062 DOI: 10.1016/j.ijpharm.2015.03.050]
- Silva LFC, Kasten G, de Campos CEM, Chinelatto AL, Lemos-Senna E. Preparation and characterization of quercetin-loaded solid lipid microparticles for pulmonary delivery. Powder Technol 2013;239:183-92. [DOI: 10.1016/j.powtec.2013.01.037]
- Videira M, Almeida A, Fabra A. Preclinical evaluation of a pulmonary delivered paclitaxel-loaded lipid nanocarrier antitumor effect. Nanomed Nanotechnol Biol Med 2012;8:1208-15. [PMID: 22206945 DOI: 10.1016/j.nano.2011.12.007]
- Fukui H, Iwahashi H, Endoh S, Nishio K, Yoshida Y, et al. Ascorbic acid attenuates acute pulmonary oxidative stress and inflammation caused by zinc oxide nanoparticles. J Occup Health 2015;57:118-25. [PMID: 25735507 DOI: 10.1539/joh.14-0161-OA]
- Menon JU, Ravikumar P, Pise A, Gyawali D, Hsia CC, et al. Polymeric nanoparticles for pulmonary protein and DNA delivery. Acta Biomater 2014;10:2643-52. [PMID: 24512977 DOI: 10.1016/j.actbio.2014.01.033]
- Zhong Q, da Rocha S. Poly(amidoamine) dendrimer-doxorubicin conjugates: in vitro characteristics and pseudosolution formulation in pressurized metered-dose inhalers. Mol Pharm 2016;13:1058-72. [PMID: 26832992 DOI: 10.1021/acs.molpharmaceut.5b00876]
- Win-Shwe T, Sone H, Kurokawa Y, Zeng Y, Zeng Q, et al. Effects of PAMAM dendrimers in the mouse brain after a single intranasal instillation. Toxicol Lett 2014;228:207-15. [PMID: 24813635 DOI: 10.1016/j.toxlet.2014.04.020]
- Rudokas M, Najlah M, Alhnan MA, Elhissi A. Liposome delivery systems for inhalation: a critical review highlighting formulation issues and anticancer applications. Med Princ Pract 2016;25(Suppl 2):60-72. [PMID: 26938856 DOI: 10.1159/000445116]
- Ehsan Z, Wetzel J, Clancy J. Nebulized liposomal amikacin for the treatment of Pseudomonas aeruginosa infection in cystic fibrosis patients. Expert Opin Invest Drugs 2014;23:743-9. [PMID: 24597573 DOI: 10.1517/13543784.2014.895322]
- Emami S, Azadmard-Damirchi S, Peighambardoust SH, Valizadeh H, Hesari J. Liposomes as carrier vehicles for functional compounds in food sector. J Exp Nanosci 2016;11:737-59. [DOI: 10.1080/17458080.2016.1148273]
- Chennakesavulu S, Mishra A, Sudheer A, Sowmya C, Suryaprakash Reddy C, et al. Pulmonary delivery of liposomal dry powder inhaler formulation for effective treatment of idiopathic pulmonary fibrosis. Asian J Pharm Sci 2018;13:91-100. [PMID: 32104382 DOI: 10.1016/j.ajps.2017.08.005]
- Harris J, Chess R. Effect of pegylation on pharmaceuticals. Nat Rev Drug Discov 2003;2:214-21. [PMID: 12612647 DOI: 10.1038/nrd1033]
- Suk JS, Xu Q, Kim N, Hanes J, Ensign LM. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev 2016;99(Pt A):28-51. [PMID: 26456916 DOI: 10.1016/j.addr.2015.09.012]
- Lin C, Wong BCK, Chen H, Bian Z, Zhang G, et al. Pulmonary delivery of triptolide-loaded liposomes decorated with anti-carbonic anhydrase IX antibody for lung cancer therapy. Sci Rep 2017;7:1097. [PMID: 28428618 DOI: 10.1038/s41598-017-00957-4]
- Manconi M, Manca M, Valenti D, Escribano E, Hillaireau H, et al. Chitosan and hyaluronan coated liposomes for pulmonary administration of curcumin. Int J Pharm 2017;525:203-10. [PMID: 28438698 DOI: 10.1016/j.ijpharm.2017.04.044]
- Manca M, Manconi M, Valenti D, Lai F, Loy G, et al. Liposomes coated with chitosan-xanthan gum (chitosomes) as potential carriers for pulmonary delivery of rifampicin. J Pharm Sci 2012;101:566-75. [PMID: 21997465 DOI: 10.1002/jps.22775]
- Dogbe M, Mafilaza A, Eleutério C, Cabral-Marques H, Simões S, et al. Pharmaceutical benefits of fluticasone propionate association to delivery systems: in vitro and in vivo evaluation. Pharmaceutics 2019;11:521. [PMID: 31658657 DOI: 10.3390/pharmaceutics11100521]
- Riaz M, Zhang X, Wong K, Chen H, Liu Q, et al. Pulmonary delivery of transferrin receptors targeting peptide surface-functionalized liposomes augments the chemotherapeutic effect of quercetin in lung cancer therapy. Int J Nanomed 2019;14:2879-902. [PMID: 31118613 DOI: 10.2147/IJN.S192219]
- Fujie T, Yoshimoto M. Rapid leakage from PEGylated liposomes triggered by bubbles. Soft Matter 2019;15:9537-46. [PMID: 31712795 DOI: 10.1039/c9sm01820d]
- Manca M, Valenti D, Sales O, Nacher A, Fadda A, et al. Fabrication of polyelectrolyte multilayered vesicles as inhalable dry powder for lung administration of rifampicin. Int J Pharm 2014;472:102-9. [PMID: 24928129 DOI: 10.1016/j.ijpharm.2014.06.009]
- Pulivendala G, Bale S, Godugu C. Inhalation of sustained release microparticles for the targeted treatment of respiratory diseases. Drug Deliv Transl Res 2020;10:339-53. [PMID: 31872342 DOI: 10.1007/s13346-019-00690-7]
- Yildiz-Peköz A, Akbal O, Tekarslan S, Sagirli A, Mulazimoglu L, et al. Preparation and characterization of doripenem-loaded microparticles for pulmonary delivery. J Aerosol Med Pulm Drug Deliv 2018;31:347-57. [PMID: 29877747 DOI: 10.1089/jamp.2017.1378]
- Wang Q, Mi G, Hickey D, Li Y, Tu J, et al. Azithromycin-loaded respirable microparticles for targeted pulmonary delivery for the treatment of pneumonia. Biomaterials 2018;160:107-23. [PMID: 29407340 DOI: 10.1016/j.biomaterials.2018.01.022]
- Oliveira P, Matos B, Pereira P, Gratieri T, Faccioli L, et al. Microparticles prepared with 50-190kDa chitosan as promising non-toxic carriers for pulmonary delivery of isoniazid. Carbohydr Polym 2017;174:421-31. [PMID: 28821088 DOI: 10.1016/j.carbpol.2017.06.090]
- Cunha L, Rosa da Costa A, Lourenço J, Buttini F, Grenha A. Spray-dried fucoidan microparticles for pulmonary delivery of antitubercular drugs. J Microencapsul 2018;35:392-405. [PMID: 30112917 DOI: 10.1080/02652048.2018.1513089]
- Amore E, Manca M, Ferraro M, Valenti D, La Parola V, et al. Salmeterol xinafoate (SX) loaded into mucoadhesive solid lipid microparticles for COPD treatment. Int J Pharm 2019;562:351-8. [PMID: 30935915 DOI: 10.1016/j.ijpharm.2019.03.059]
- Amore E, Ferraro M, Manca M, Gjomarkaj M, Giammona G, Pace E, et al. Mucoadhesive solid lipid microparticles for controlled release of a corticosteroid in the chronic obstructive pulmonary disease treatment. Nanomedicine (London, England) 2017;12:2287-302. [PMID: 28868971 DOI: 10.2217/nnm-2017-0072]
- Patra JK, Das G, Fraceto LF, Campos EVR, Rodriguez-Torres MDP, et al. Nano based drug delivery systems: recent developments and future prospects. J Nanobiotechnol 2018;16:71. [PMID: 30231877 DOI: 10.1186/s12951-018-0392-8]
- Kedar U, Phutane P, Shidhaye S, Kadam V. Advances in polymeric micelles for drug delivery and tumor targeting. Nanomed Nanotechnol Biol Med 2010;6:714-29. [PMID: 20542144 DOI: 10.1016/j.nano.2010.05.005]
- Shang S, Kats D, Cao L, Morgun E, Velluto D, et al. Mycobacterium tuberculosis induction of lipid-specific T cell responses by pulmonary delivery of mycolic acid-loaded polymeric micellar nanocarriers. Front Immunol 2018;9:2709. [PMID: 30538700 DOI: 10.3389/fimmu.2018.02709]
- Rezazadeh M, Davatsaz Z, Emami J, Hasanzadeh F, Jahanian-Najafabadi A. Preparation and characterization of spray-dried inhalable powders containing polymeric micelles for pulmonary delivery of paclitaxel in lung cancer. J Pharm Pharm Sci 2018;21:200s-14s. [PMID: 30321135 DOI: 10.18433/jpps30048]
- Sham J, Zhang Y, Finlay W, Roa W, Löbenberg R. Formulation and characterization of spray-dried powders containing nanoparticles for aerosol delivery to the lung. Int J Pharm 2004;269:457-67. [PMID: 14706257 DOI: 10.1016/j.ijpharm.2003.09.041]
- Hu X, Yang F, Quan L, Liu C, Liu X, et al. Pulmonary delivered polymeric micelles—pharmacokinetic evaluation and biodistribution studies. Eur J Pharm Biopharm 2014;88:1064-75. [PMID: 25460153 DOI: 10.1016/j.ejpb.2014.10.010]
- Andrade F, Fonte P, Costa A, Reis C, Nunes R, et al. Pharmacological and toxicological assessment of innovative self-assembled polymeric micelles as powders for insulin pulmonary delivery. Nanomedicine (London, England) 2016;11:2305-17. [PMID: 27487859 DOI: 10.2217/nnm-2016-0045]
- Omlor A, Nguyen J, Bals R, Dinh Q. Nanotechnology in respiratory medicine. Respir Res 2015;16:64. [PMID: 26021823 DOI: 10.1186/s12931-015-0223-5]
- Huang YW, Cambre M, Lee HJ. The toxicity of nanoparticles depends on multiple molecular and physicochemical mechanisms. Int J Mol Sci 2017;18:2702. [PMID: 29236059 DOI: 10.3390/ijms18122702]
- Shah SR, Prajapati HR, Sheth DB, Gondaliya EM, Vyas AJ, et al. Pharmacokinetics and in vivo distribution of optimized PLGA nanoparticles for pulmonary delivery of levofloxacin. J Pharm Pharmacol 2020;72:1026-37. [PMID: 32337714 DOI: 10.1111/jphp.13275]
- Roa W, Azarmi S, Al-Hallak M, Finlay W, Magliocco A, et al. Inhalable nanoparticles, a non-invasive approach to treat lung cancer in a mouse model. J Control Release 2011;150:49-55. [PMID: 21059378 DOI: 10.1016/j.jconrel.2010.10.035]
- Ding J, Chen J, Gao L, Jiang Z, Zhang Y, et al. Engineered nanomedicines with enhanced tumor penetration. Nanotoday 2019;29:100800. [DOI: 10.1016/j.nantod.2019.100800]
- Fox ME, Szoka FC, Fréchet JM. Soluble polymer carriers for the treatment of cancer: the importance of molecular architecture. Acc Chem Res 2009;42:1141-51. [PMID: 19555070 DOI: 10.1021/ar900035f]
- Stylianopoulos T, Poh MZ, Insin N, Bawendi MG, Fukumura D, et al. Diffusion of particles in the extracellular matrix: the effect of repulsive electrostatic interactions. Biophys J 2010;99:1342-9. [PMID: 20816045 DOI: 10.1016/j.bpj.2010.06.016]
- Chishti N, Jagwani S, Dhamecha D, Jalalpure S, Dehghan M. Preparation, optimization, and in vivo evaluation of nanoparticle-based formulation for pulmonary delivery of anticancer drug. Medicina (Kaunas, Lithuania) 2019;55:294. [PMID: 31226865 DOI: 10.3390/medicina55060294]
- Rawal T, Patel S, Butani S. Chitosan nanoparticles as a promising approach for pulmonary delivery of bedaquiline. Eur J Pharm Sci 2018;124:273-87. [PMID: 30176365 DOI: 10.1016/j.ejps.2018.08.038]
- Al-Nemrawi N, Alshraiedeh N, Zayed A, Altaani B. Low molecular weight chitosan-coated PLGA nanoparticles for pulmonary delivery of tobramycin for cystic fibrosis. Pharmaceuticals (Basel, Switzerland) 2018;11:28. [PMID: 29517998 DOI: 10.3390/ph11010028]
- Sun P, Huang W, Kang L, Jin M, Fan B, et al. siRNA-loaded poly(histidine-arginine)-modified chitosan nanoparticle with enhanced cell-penetrating and endosomal escape capacities for suppressing breast tumor metastasis. Int J Nanomed 2017;12:3221-34. [PMID: 28458542 DOI: 10.2147/IJN.S129436]
- Davenport L, Hsieh H, Eppert B, Carreira V, Krishan M, et al. Systemic and behavioral effects of intranasal administration of silver nanoparticles. Neurotoxicol Teratol 2015;51:68-76. [PMID: 26340819 DOI: 10.1016/j.ntt.2015.08.006]
- Gaiser B, Fernandes T, Jepson M, Lead J, Tyler C, et al. Interspecies comparisons on the uptake and toxicity of silver and cerium dioxide nanoparticles. Environ Toxicol Chem 2012;31:144-54. [PMID: 22002553 DOI: 10.1002/etc.703]
- Roda E, Bottone M, Biggiogera M, Milanesi G, Coccini T. Pulmonary and hepatic effects after low dose exposure to nanosilver: early and long-lasting histological and ultrastructural alterations in rat. Toxicol Rep 2019;6:1047-60. [PMID: 31673507 DOI: 10.1016/j.toxrep.2019.09.008]
- Wang X, Ji Z, Chang C, Zhang H, Wang M, et al. Use of coated silver nanoparticles to understand the relationship of particle dissolution and bioavailability to cell and lung toxicological potential. Small 2014;10:385-98. [PMID: 24039004 DOI: 10.1002/smll.201301597]
- Hamilton R, Buckingham S, Holian A. The effect of size on Ag nanosphere toxicity in macrophage cell models and lung epithelial cell lines is dependent on particle dissolution. Int J Mol Sci 2014;15:6815-30. [PMID: 24758926 DOI: 10.3390/ijms15046815]
- Mittal P, Saharan A, Verma R, Altalbawy F, Alfaidi M, et al. Dendrimers: a new race of pharmaceutical nanocarriers. BioMed Res Int 2021;2021:8844030. [PMID: 33644232 DOI: 10.1155/2021/8844030]
- Svenson S, Chauhan AS. Dendrimers for enhanced drug solubilization. Nanomedicine (London, England) 2008;3:679-702. [PMID: 18817470 DOI: 10.2217/17435889.3.5.679]
- Nagpal K, Kumar P, Mohan A, Thakur S. Dendrimers for therapeutic delivery: compositions, characterizations, and current status. Crit Rev Ther Drug Carrier Syst 2019;36:277-304. [PMID: 31679189 DOI: 10.1615/CritRevTherDrugCarrierSyst.2018025749]
- Pourianazar NT, Mutlu P, Gunduz U. Bioapplications of poly (amidoamine) (PAMAM) dendrimers in nanomedicine. J Nanopart Res 2014;16:1-38. [DOI: 10.1007/s11051-014-2342-1]
- Kaminskas L, Kelly B, McLeod V, Sberna G, Owen D, et al. Characterisation and tumour targeting of PEGylated polylysine dendrimers bearing doxorubicin via a pH labile linker. J Control Release 2011;152:241-8. [DOI: 10.1016/j.jconrel.2011.02.005]
- Navarro G, Maiwald G, Haase R, Rogach A, Wagner E, et al. Low generation PAMAM dendrimer and CpG free plasmids allow targeted and extended transgene expression in tumors after systemic delivery. J Control Release 2010;146:99-105. [PMID: 20438778 DOI: 10.1016/j.jconrel.2010.04.030]
- Svenson S. Dendrimers as versatile platform in drug delivery applications. Eur J Pharm Biopharm 2009;71:445-62. [PMID: 18976707 DOI: 10.1016/j.ejpb.2008.09.023]
- Bohr A, Tsapis N, Foged C, Andreana I, Yang M, et al. Treatment of acute lung inflammation by pulmonary delivery of anti-TNF-α siRNA with PAMAM dendrimers in a murine model. Eur J Pharm Biopharm 2020;156:114-20. [DOI: 10.1016/j.ejpb.2020.08.009]
- Bai S, Thomas C, Ahsan F. Dendrimers as a carrier for pulmonary delivery of enoxaparin, a low-molecular weight heparin. J Pharm Sci 2007;96:2090-106. [PMID: 17286291 DOI: 10.1002/jps.20849]
- Yan C, Gu J, Lv Y, Shi W, Wang Y, et al. Caproyl-modified G2 PAMAM dendrimer (G2-AC) nanocomplexes increases the pulmonary absorption of insulin. AAPS PharmSciTech 2019;20:298. [PMID: 31456109 DOI: 10.1208/s12249-019-1505-x]
- Zhong Q, Humia B, Punjabi A, Padilha F, da Rocha S. The interaction of dendrimer-doxorubicin conjugates with a model pulmonary epithelium and their cosolvent-free, pseudo-solution formulations in pressurized metered-dose inhalers. Eur J Pharm Sci 2017;109:86-95. [PMID: 28774811 DOI: 10.1016/j.ejps.2017.07.030]
- Ryan G, Kaminskas L, Kelly B, Owen D, McIntosh M, et al. Pulmonary administration of PEGylated polylysine dendrimers: absorption from the lung versus retention within the lung is highly size-dependent. Mol Pharm 2013;10:2986-95. [PMID: 23750747 DOI: 10.1021/mp400091n]
- Bailey M, Berkland C. Nanoparticle formulations in pulmonary drug delivery. Med Res Rev 2009;29:196-212. [PMID: 18958847 DOI: 10.1002/med.20140]
- Santos A, Veiga F, Figueiras A. Dendrimers as pharmaceutical excipients: synthesis, properties, toxicity and biomedical applications. Materials (Basel) 2019;13:65. [PMID: 31877717 DOI: 10.3390/ma13010065]
- Zaru M, Manca ML, Fadda AM, Antimisiaris SG. Chitosan-coated liposomes for delivery to lungs by nebulisation. Colloids Surfaces B Biointerfaces 2009;71:88-95. [PMID: 19201583 DOI: 10.1016/j.colsurfb.2009.01.010]
- Knop K, Hoogenboom R, Fischer D, Schubert US. Poly(ethylene glycol) in drug delivery: pros and cons as well as potential alternatives. Angew Chem Int Ed 2010;49:6288-308. [PMID: 20648499 DOI: 10.1002/anie.200902672]
- Lee HJ, Lee HG, Kwon YB, Kim JY, Rhee YS, et al. The role of lactose carrier on the powder behavior and aerodynamic performance of bosentan microparticles for dry powder inhalation. Eur J Pharm Sci 2018;117:279-89. [PMID: 29510172 DOI: 10.1016/j.ejps.2018.03.004]
- Rabbani NR, Seville PC. The influence of formulation components on the aerosolisation properties of spray-dried powders. J Control Release 2005;110:130-40. [PMID: 16226334 DOI: 10.1016/j.jconrel.2005.09.004]
- Zheng C, Li M, Ding J. Challenges and opportunities of nanomedicines in clinical translation. BIO Integr 2021;2:57-60. [DOI: 10.15212/bioi-2021-0016]
- Wicki A, Witzigmann D, Balasubramanian V, Huwyler J. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release 2015;200:138-57. [PMID: 25545217 DOI: 10.1016/j.jconrel.2014.12.030]
- Pattni BS, Chupin VV, Torchilin VP. New developments in liposomal drug delivery. Chem Rev 2015;115:10938-66. [PMID: 26010257 DOI: 10.1021/acs.chemrev.5b00046]
- Bae YH, Park K. Advanced drug delivery 2020 and beyond: perspectives on the future. Adv Drug Deliv Rev 2020;158:4-16. [PMID: 32592727 DOI: 10.1016/j.addr.2020.06.018]