Effects of Vitamin D Supplementation During Pregnancy on Preterm Birth Risk and Maternal-Neonatal Outcomes: A Systematic Review and Meta-Analysis of 38 Randomized Controlled Trials
1Center for Reproductive Medicine, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan 450052, China
2Department of Pharmacy, The Second Xiangya Hospital, Central South University, Changsha, Hunan 410011, PR China
3Institute of Clinical Pharmacy, Central South University, Changsha, Hunan 410011, PR China
4Mathematical Engineering Academy of Chinese Medicine, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong 510006, PR China
5Department of Gynecology and Obstetrics, The Second Xiangya Hospital of Central South University, 139 Middle Renmin Road, Changsha, Hunan 410011, PR China
6Department of Geriatrics, The Second Xiangya Hospital, Central South University, Changsha, Hunan 410011, PR China
7Department of Urology, The Second Xiangya Hospital of Central South University, Changsha, Hunan 410011, PR China
aThese authors contributed equally to this work.
*Correspondence to: Zhaokai Zhou, Department of Pharmacy and Department of Urology, The Second Xiangya Hospital of Central South University, 139 Middle Renmin Road, Changsha, Hunan 410011, PR China. E-mail: 13526278113@163.com; Qiyue Zheng, Department of Pharmacy, The Second Xiangya Hospital of Central South University, Changsha 410011, PR China. E-mail: yz_2606@163.com
Received: December 24 2025; Revised: April 30 2026; Accepted: June 23 2026; Published Online: July 14 2026
Cite this paper:
Zuo L, Wang J, Xie X et al. Effects of Vitamin D Supplementation During Pregnancy on Preterm Birth Risk and Maternal-Neonatal Outcomes: A Systematic Review and Meta-Analysis of 38 Randomized Controlled Trials. BIO Integration 2026; 7: 1–17.
DOI: 10.15212/bioi-2025-0224. Available at: https://bio-integration.org/
Download citation
© 2026 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Background and objective: Preterm birth complications are among leading causes of mortality in neonates and children under 5 years of age worldwide. The association between prenatal vitamin D supplementation and risk of preterm birth is controversial based on randomized controlled trials (RCTs). We aimed to determine the effect of vitamin D supplementation during pregnancy on preterm birth and maternal and neonatal secondary outcomes, and to ascertain whether the effects of vitamin D supplementation on preterm birth differed by baseline 25(OH)D status, supplementation dose, and timing of initiation.
Data sources: PubMed, Web of Science, Medline, Cochrane Library, and Embase were searched from inception to April 2023 with no language restrictions.
Study selection: RCTs comparing vitamin D supplementation with placebo, no treatment, or standard low-dose vitamin D (≤ 600 IU/day) in pregnant women were included. The primary outcome was preterm birth (<37 weeks’ gestation) and secondary outcomes included maternal adverse events and neonatal anthropometric indicators.
Results: Thirty-eight RCTs involving 17,392 pregnant women were included. Nineteen RCTs involving 7959 pregnant women reported preterm birth. Vitamin D supplementation was associated with a borderline increase in preterm birth risk in the primary analysis (RR, 1.13; 95% CI, 1.01–1.26; P = 0.04; I2 = 0%) but this association was modest and largely driven by one large RCT among women living with HIV. An increased preterm birth signal was noted among participants with a baseline 25(OH)D ≥ 30 nmol/L (OR, 1.25; 95% CI, 1.05–1.48) in exploratory subgroup analyses presented as ORs and this signal was entirely derived from the same HIV trial. No significant subgroup associations were detected in the < 30 nmol/L subgroup or by supplementation dose or initiation timing. No significant effects were noted for maternal or neonatal secondary outcomes.
Limitations: The main study limitations included incomplete reporting of preterm births across trials, reliance on the risk signal on a single population-specific risk signal, dichotomization of baseline 25(OH)D status, and lack of individual participant data for refined subgroup analyses.
Conclusions: Current evidence does not support universal vitamin D supplementation to prevent preterm birth. A possible increased risk of preterm birth among participants with a baseline 25(OH)D ≥ 30 nmol/L should be interpreted cautiously because this finding was driven by a single trial in HIV-positive pregnant women and should not be generalized to healthy pregnant women. Further large-scale RCTs and individual participant data meta-analyses are warranted to clarify whether baseline vitamin D status modifies effects of vitamin D supplementation.
Keywords
Maternal outcomes, neonatal outcomes, pregnancy, preterm birth, randomized controlled trials, vitamin D.
Introduction
Preterm birth, which is defined by the World Health Organization as a birth before 37 completed weeks of gestation or fewer than 259 days from the first day of the last menstrual period, remains a major contributor to neonatal morbidity and mortality worldwide [1]. Preterm infants are at increased risk of short-term complications, including respiratory distress syndrome, necrotizing enterocolitis, and sepsis, as well as long-term sequelae, such as neurodevelopmental impairment, chronic lung disease, and metabolic disorders, which impose substantial clinical, economic, and psychological burdens on families and healthcare systems [2–7]. Despite extensive research, the etiology of preterm birth is multifactorial and incompletely understood, and effective preventive strategies are limited [5, 8].
Vitamin D insufficiency and deficiency are common among pregnant women worldwide. Maternal vitamin D status has been investigated as a potentially modifiable factor related to adverse pregnancy outcomes [9]. Vitamin D is a fat-soluble secosteroid hormone, the active form of which [1,25-dihydroxyvitamin D3 (1,25(OH)2D3)] acts through the vitamin D receptor (VDR), which is expressed in placental trophoblasts, uterine smooth muscle, and immune cells. Vitamin D may contribute to maternal-fetal immune tolerance, placental trophoblast invasion and angiogenesis, and calcium homeostasis in uterine smooth muscle through these pathways [10]. Observational studies have linked lower maternal 25-hydroxyvitamin D (25(OH)D) concentrations with increased risks of adverse pregnancy outcomes, including preeclampsia, gestational diabetes, and preterm birth [11–15]. However, observational associations do not establish causality and findings from randomized controlled trials (RCTs) and meta-analyses evaluating prenatal vitamin D supplementation have been inconsistent with some studies reporting potential benefit, others showing neutral effects, and a few suggesting possible harm signals.
Several evidence gaps in the association between vitamin D and preterm birth remain. First, many meta-analyses have evaluated vitamin D supplementation using a “one-size-fits-all” approach, despite evidence suggesting that baseline maternal 25(OH)D status may modify the effects of supplementation on pregnancy outcomes. This issue is clinically relevant because baseline nutrient status is a key determinant of response to nutritional interventions and is central to precision nutrition frameworks [16]. Second, pooled analyses have included trials conducted in special populations, such as women living with human immunodeficiency virus (HIV), without fully examining how population-specific factors may influence pooled estimates or subgroup findings. Third, although recent evidence syntheses have updated overall effects of vitamin D supplementation during pregnancy, the extent to which supplementation effects differ by baseline 25(OH)D status, dose, and gestational age at initiation has not been established [17].
To address these gaps, we performed a systematic review and meta-analysis of 38 RCTs to evaluate the effect of vitamin D supplementation during pregnancy on preterm birth risk and secondary maternal and neonatal outcomes [18, 19]. We further performed prespecified subgroup analyses according to baseline 25(OH)D status, supplementation dose, and timing of initiation to explore potential effect modification and to facilitate more individualized interpretation of prenatal vitamin D supplementation evidence.
Materials and methods
This systematic review and meta-analysis were performed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (Supplementary Table S1). The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42022328941). The eligibility criteria were defined according to the PICOS framework, including population, intervention, comparison, outcome, and study design.
Data source and search strategy
We systematically searched five electronic databases, including PubMed, Web of Science, Medline, Cochrane Library, and Embase, from database inception to April 2023 with no language restrictions. The search combined MeSH terms and free-text terms related to “vitamin D,” “pregnancy,” and “randomized controlled trial.” The full search strategy for each database is provided in Supplementary Material 1. We also manually screened reference lists of included studies and relevant systematic reviews to identify additional eligible trials.
Eligibility criteria
Trials were eligible for inclusion if the following criteria were met: (1) [study design] parallel-group RCTs, including cluster-randomized RCTs; (2) [population] pregnant women enrolled before or during pregnancy and followed up until delivery; (3) [intervention] vitamin D supplementation, either alone or in combination with other micronutrients, with no restriction on dose, frequency, or duration; (4) [comparison] placebo, no treatment, or standard low-dose vitamin D supplementation defined as ≤ 600 IU/d and treated as a background or standard-care comparator rather than therapeutic-dose supplementation; and (5) [outcomes] at least one primary or secondary outcome. The primary outcome was preterm birth, defined as birth before 37 completed weeks of gestation. The secondary outcomes included stillbirth, spontaneous abortion, preeclampsia, gestational hypertension, birth length, birth weight, head circumference at birth, and low birth weight.
Non-randomized studies, secondary analyses of RCTs, animal studies, in vitro studies, conference abstracts without extractable data, duplicate reports without additional eligible outcomes, or studies with no extractable or derivable data for any prespecified outcome were excluded. Missingness was not defined by a fixed percentage of loss to follow-up but by the absence of usable outcome-level summary data required for quantitative synthesis. The most complete report was used when multiple reports described the same trial population and additional reports were only reviewed for supplementary outcome or intervention information.
Study selection and data extraction
Three reviewers (ZLL, WJJ, and LQ) independently screened titles and abstracts to identify potentially eligible studies. Then, two reviewers (ZQY and PM) independently assessed full-text articles for final inclusion. Disagreements at any stage were resolved by discussion with a third senior reviewer.
Two reviewers (ZZK and XXY) independently extracted data using a standardized, pre-piloted data extraction form. The extracted data included the following: (1) study characteristics, including first author, publication year, country, study design, and sample size; (2) participant characteristics, including baseline 25(OH)D concentration, age range, and inclusion/exclusion criteria; (3) intervention and comparator details, including vitamin D dose, frequency, timing of initiation, duration, co-interventions, and control conditions; and (4) outcome data, including number of events and total participants for binary outcomes, and mean, standard deviation, and sample size for continuous outcomes.
The means and standard deviations were extracted when available for continuous outcomes. Outcomes were converted to means and standard deviations using established statistical methods when reported as the median with interquartile ranges or ranges. Data were extracted as the number of events and number of participants analyzed in each group for binary outcomes. Participants lost to follow-up were excluded from outcome-specific denominators unless the original study reported intention-to-treat data. Calculated values were included if missing summary statistics could be derived from other reported information. Studies reporting at least one prespecified outcome with usable data were retained and included only in the corresponding outcome-specific meta-analyses.
Risk of bias, publication bias, and certainty of evidence assessment
Two independent reviewers (WJJ and HJY) assessed risk of bias of included RCTs using Cochrane risk-of-bias tool. Assessment covered random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias. Each domain was rated as low risk, unclear risk, or high risk of bias. Disagreements were resolved by consensus or consultation with a third reviewer.
Two reviewers (ZZK and ZLL) independently assessed certainty of evidence for each outcome using Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. Evidence certainty was evaluated across domains of risk of bias, inconsistency, indirectness, imprecision, and publication bias. Certainty of evidence was rated as high, moderate, low, or very low.
Publication bias and small-study effects were assessed for the primary outcome (preterm birth) by visual inspection of a funnel plot. Funnel plots were not formally interpreted for other outcomes because of limited numbers of studies or limited interpretability.
Data synthesis and statistical analysis
All meta-analyses were performed using Review Manager 5.4 (Cochrane Collaboration, Copenhagen, Denmark). Pooled relative risks (RRs) with 95% confidence intervals (CIs) were calculated for primary overall analysis and other binary outcomes. Pooled standardized mean differences (SMDs) with 95% CIs were calculated for continuous outcomes. All statistical tests were two-sided and P values < 0.05 were considered statistically significant. Forest plots were used to display study-specific and pooled effect estimates.
Only trials reporting extractable data for that specific outcome were included in corresponding meta-analysis for each outcome. Therefore, the number of included trials and participants differed across outcomes. A random-effects model using the DerSimonian-Laird method was applied as the primary analytical model to account for potential between-study heterogeneity. Statistical heterogeneity was quantified using an I2 statistic with I2 values of 0–25%, 26–50%, 51–75%, and > 75% interpreted as negligible, moderate, substantial, and considerable heterogeneity, respectively. Cochran’s Q test and τ2 were also considered when interpreting between-study heterogeneity.
Prespecified subgroup analyses were performed for the primary outcome (preterm birth) according to baseline 25(OH)D status (< 30 nmol/L vs. ≥ 30 nmol/L), daily vitamin D supplementation dose (< 2000 IU/day, 2000–4000 IU/day, and ≥ 4000 IU/day), and gestational age at supplementation initiation (first trimester vs. second trimester). For these subgroup analyses, odds ratios (ORs) with 95% CIs were estimated using Mantel-Haenszel fixed-effect models. ORs were used as a standard effect measure for binary outcomes and are suitable for stratified comparisons across subgroups, particularly when the number of trials and events differed across strata. OR-based subgroup analyses were used to explore whether the association differed across predefined subgroups and were interpreted alongside rather than in place of the primary RR-based overall analysis. Tests for subgroup differences were used to evaluate whether pooled estimates differed across strata.
Sensitivity analyses were performed to examine robustness of pooled effect estimates. These included sequential exclusion of studies rated as high overall risk of bias, use of a fixed-effect model as an alternative to primary random-effects model, and exclusion of a single large trial conducted among women living with HIV that appeared to drive main subgroup signal.
Results
Search results and characteristics of the included studies
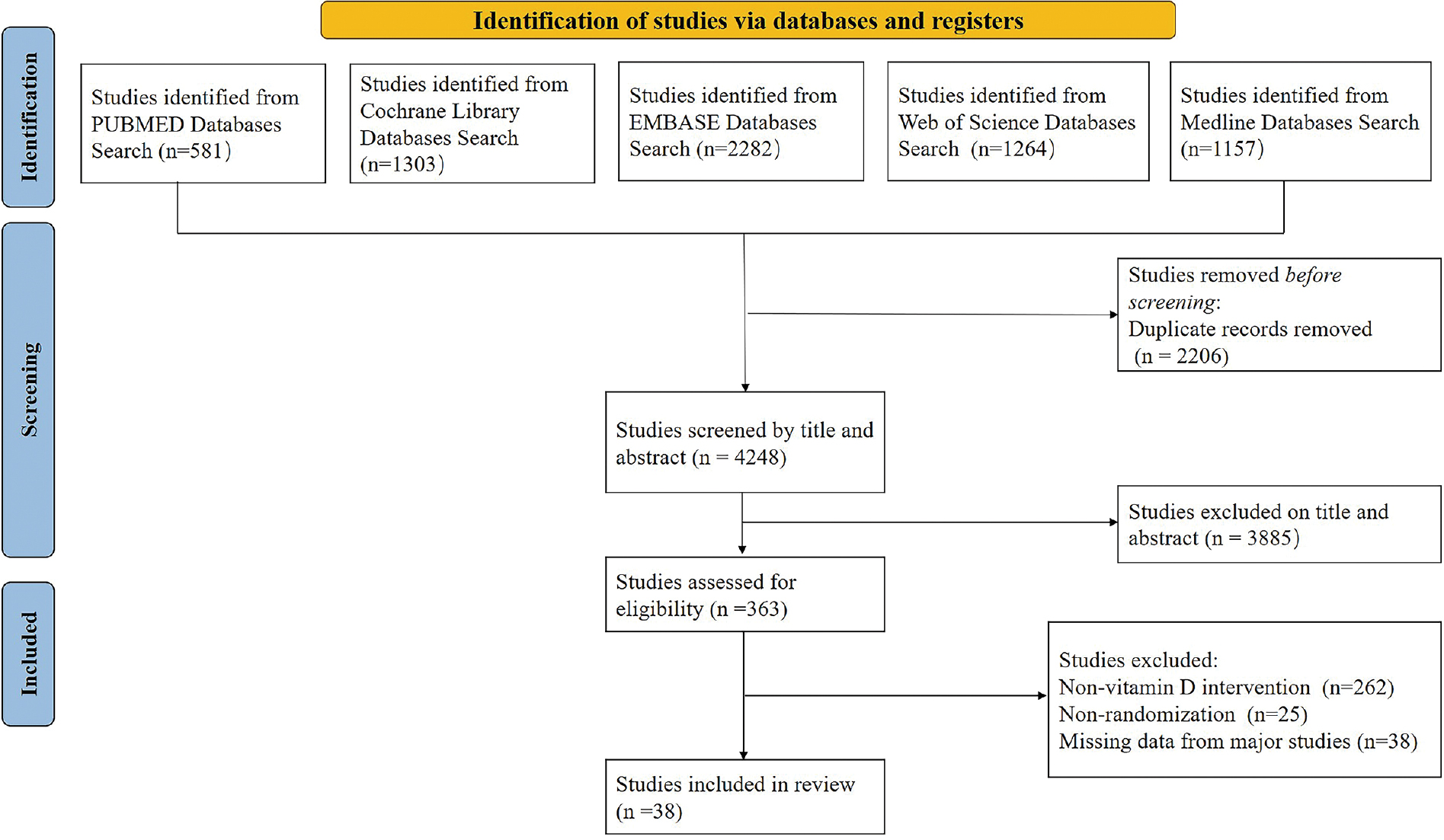
A total of 6454 records were identified and screened based on a predefined search strategy. After title and abstract screening, 363 full-text articles were assessed for eligibility and 38 RCTs were ultimately included in the systematic review and meta-analysis. The main reasons for exclusion were non-vitamin D intervention (n = 262), non-randomized design (n = 25), and absence of extractable or derivable data for any prespecified outcome (n = 38; Figure 1).
Figure 1 PRISMA flow diagram of study selection for meta-analysis. Flow diagram showing process of literature searching, screening, eligibility assessment, and final inclusion of randomized controlled trials.
The characteristics of included trials are summarized in Table 1. A total of 38 RCTs involving 17,392 pregnant women were included. Among these studies, 17 were placebo-controlled, 11 compared two different vitamin D doses, and 10 compared multiple vitamin D doses. Most trials enrolled generally healthy pregnant women, whereas one large trial was conducted among HIV-positive pregnant women. Twenty-five trials were published in or after 2016 (Table 1).
Table 1 Summary of Studies Included
| Study | Region | Study Design | Sample Size | Interventions | Timing of Vitamin D Supplementation (Gestational Weeks) |
|---|---|---|---|---|---|
| Ali et al. 2019 [32] | Saudi Arabia | Randomized controlled trial | 164 | 400 IU/d vs. 4000 IU/d | 13 weeks |
| Litonjua et al. 2020 [33] | United States of America | Randomized double-blind placebo-controlled trial | 806 | 400 IU/d vs. 4400 IU/d | 10–18 weeks |
| Litonjua et al. 2016 [34] | United States of America | Randomized, double-blind, placebo-controlled trial | 881 | 400 IU/d vs. 4400 IU/d | 10–18 weeks |
| Chawes et al. 2016 [35] | Denmark | Double-blind, single-center, randomized clinical trial | 623 | 400 IU/d vs. 2800 IU/d | 24 weeks |
| Hollis et al. 2011 [36] | United States of America | Single center, randomized, controlled, double-blinded study | 516 | 400 IU/d vs. 2000 IU/d vs. 4000 IU/d | 12–16 weeks |
| Grant et al. 2014 [37] | New Zealand | Randomized, double-blind, placebo-controlled trial | 404 | Placebo vs. 1000 IU/d vs. 2000 IU/d | 27 weeks |
| Wagner et al. 2013 [38] | United States of America | Randomized controlled trial | 504 | 400 IU/d vs. 2000 IU/d vs. 4000 IU/d | 12–16 weeks |
| Sudfeld et al. 2022 [25] | Tanzania | Randomized, triple-blind, placebo-controlled trial | 2167 (HIV-positive pregnant women) | Placebo vs. 3000 IU/d | 12–27 weeks |
| Wall et al. 2016 [39] | Auckland, New Zealand | Randomized, double-blinded, placebo-controlled trial | 75 | Placebo vs. 1000 IU/d vs. 2000 IU/d | 27 weeks |
| Yap et al. 2014 [40] | Australia | Double-blind randomized controlled trial | 203 | 400 IU/d vs. 5000 IU/d | < 20 weeks |
| Cooper et al. 2016 [41] | UK | Multicenter, double-blind, randomized placebo-controlled trial | 965 | Placebo vs. 1000 IU/d | 14–17 weeks |
| Enkhmaa et al. 2019 [42] | Mongolia | Randomized, controlled, double-blind trial | 512 | 600 IU/d vs. 2000 IU/d vs. 4000 IU/d | 12–16 weeks |
| Roth et al. 2013 [43] | Bangladesh | Randomized double-blind placebo-controlled trial | 147 | Placebo vs. 5000 IU/d | 26–29 weeks |
| Roth et al. 2018 [28] | Bangladesh | Randomized, double-blind, placebo-controlled trial | 1298 | Placebo vs. 600 IU/d vs. 2400 IU/d vs. 4000 IU/d | 17–24 weeks |
| Roth et al. 2013 [44] | Bangladesh | Randomized controlled trial | 147 | Placebo vs. 5000 IU/d | 26 and < 30 weeks |
| Curtis et al. 2021 [45] | UK | Randomized, double-blind, placebo-controlled trial | 965 | Placebo vs. 1000 IU/d | 14 weeks |
| Hornsby et al. 2018 [46] | United States of America | Multicenter, randomized, double-blind, placebo-controlled clinical trial | 876 | 400 IU/d vs. 4400 IU/d | 10–18 weeks |
| Mutlu et al. 2014 [47] | Turkey | Randomized controlled trial | 51 | 600 IU/d vs. 1200 IU/d vs. 2000 IU/d | 13–32 weeks |
| Xiaomang et al. 2021 [48] | China | Randomized controlled trial | 450 | 400 IU/d vs. 1500 IU/d vs. 4000 IU/d | 13 weeks |
| March et al. 2015 [49] | Canada | Double-blind randomized controlled trial | 249 | 400 IU/d vs. 1000 IU/d vs. 2000 IU/d | 13–24 weeks |
| O’Callaghan et al. 2022 [50] | Dhaka, Bangladesh | Double-blind, dose-ranging trial | 1300 | Placebo vs. 600 IU/d vs. 2400 IU/d vs. 4000 IU/d | 17–24 weeks |
| Sass et al. 2020 [51] | Denmark | Randomized double-blind placebo-controlled trial | 623 | 400 IU/d vs. 2800 IU/d | 24 weeks |
| Chen et al. 2020 [52] | United States of America | Randomized controlled trial | 92 | Placebo vs. 4000 IU/d | 10–14 weeks |
| Karamali et al. 2015 [53] | Iran | Randomized double-blind placebo-controlled trial | 60 | Placebo vs. 3571 IU/d | 20 weeks |
| Valizadeh et al. 2016 [54] | Iran | Randomized controlled trial | 84 | Placebo vs. 14,286 IU/d | 12 and 32 weeks |
| Razavi et al. 2017 [55] | Iran | Randomized, double-blind, placebo-controlled trial | 120 | Placebo vs. 3571 IU/d | 24–28 weeks |
| Hjelmsø et al. 2020 [56] | Denmark | Nested, factorial, double-blind, placebo-controlled, randomized trial | 736 | 400 IU/d vs. 2800 IU/d | 24 weeks |
| Zerofsky et al. 2016 [57] | United States of America | Randomized controlled trial | 57 | 400 IU/d vs. 2000 IU/d | < 20 weeks |
| Hossain et al. 2014 [58] | Pakistan | Randomized controlled trial | 175 | Placebo vs. 4000 IU/d | 20 weeks |
| Alhomaid et al. 2021 [59] | Northern Ireland | 2-arm parallel double-blind randomized trial | 240 | 400 IU/d vs. 800 IU/d | 12 weeks |
| Corcoy et al. 2020 [60] | Spain | Multicenter randomized controlled trial | 140 | Placebo vs. 1600 IU/d | 20 weeks |
| El-Heis et al. 2022 [61] | UK | Multicenter, double-blind, randomized, placebo-controlled trial | 703 | Placebo vs. 1000 IU/d | 14 weeks |
| Sahoo et al. 2017 [62] | India | Randomized double-blind placebo-controlled trial | 300 | Placebo vs. 1071 IU/d vs. 2143 IU/d | 14–20 weeks |
| Morris et al. 2021 [63] | Bangladesh | Randomized double-blind placebo-controlled trial | 1174 | Placebo vs. 600 IU/d vs. 2400 IU/d vs. 4000 IU/d | 17–24 weeks |
| Naushee et al. 2021 [64] | Pakistan | Double-blinded, randomized controlled trial | 350 | 400 IU/d vs. 2000 IU/d vs. 4000 IU/d | 12–16 weeks |
| Motamed et al. 2019 [65] | Iran | Randomized controlled trial | 73 | 1000 IU/d vs. 2000 IU/d | First trimester |
| Goldring et al. 2013 [66] | United Kingdom | Randomized controlled trial | 158 | Placebo vs. 800 IU/d vs. 200,000 IU | 27 weeks |
| Asemi and Esmaillzadeh 2015 [67] | Iran | Double blind randomized controlled clinical trial | 45 | Placebo vs. 4762 IU/d | 24–28 weeks |
Risk of bias and publication bias assessment
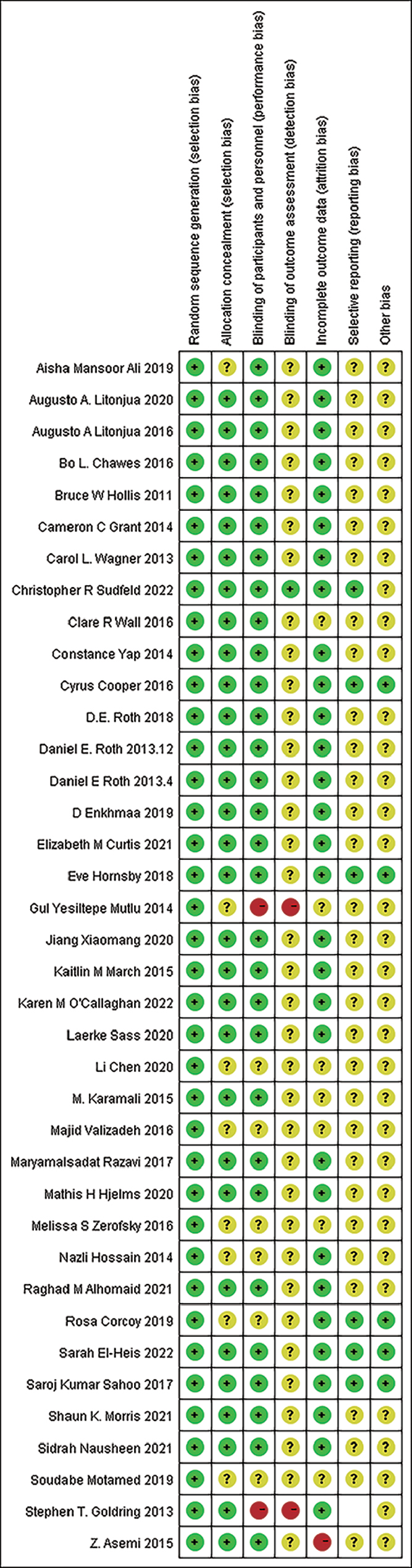
The risk of bias assessment is shown in Figure 2. All studies included were randomized trials. Three trials were judged to be at high overall risk of bias, whereas most trials were assessed as having a low or moderate risk of bias. Thirty trials used double-blind designs and 30 trials reported allocation concealment methods. However, reporting of selective outcome reporting was incomplete in several studies, which may have introduced uncertainty in interpretation of the pooled estimates.
Figure 2 Summary of risk of bias for each included study. Risk of bias was assessed according to Cochrane Collaboration tool. Green dots (+) indicate low risk of bias, red dots (−) indicate high risk of bias, and yellow dots (?) indicate unclear risk of bias.
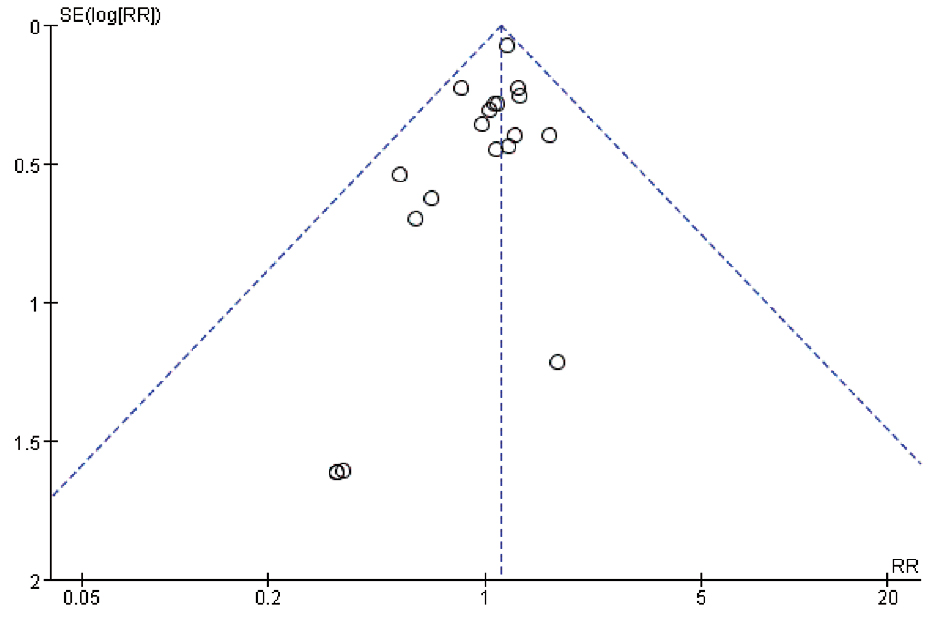
The funnel plot for the primary outcome (preterm birth) was visually symmetric, suggesting no obvious evidence of publication bias or small-study effects (Figure 3).
Figure 3 Funnel plot for preterm birth to assess potential publication bias. The funnel plot was visually inspected to assess potential publication bias and small-study effects for preterm birth. No obvious funnel plot asymmetry was observed but visual inspection alone cannot exclude publication bias.
Effects on primary outcome
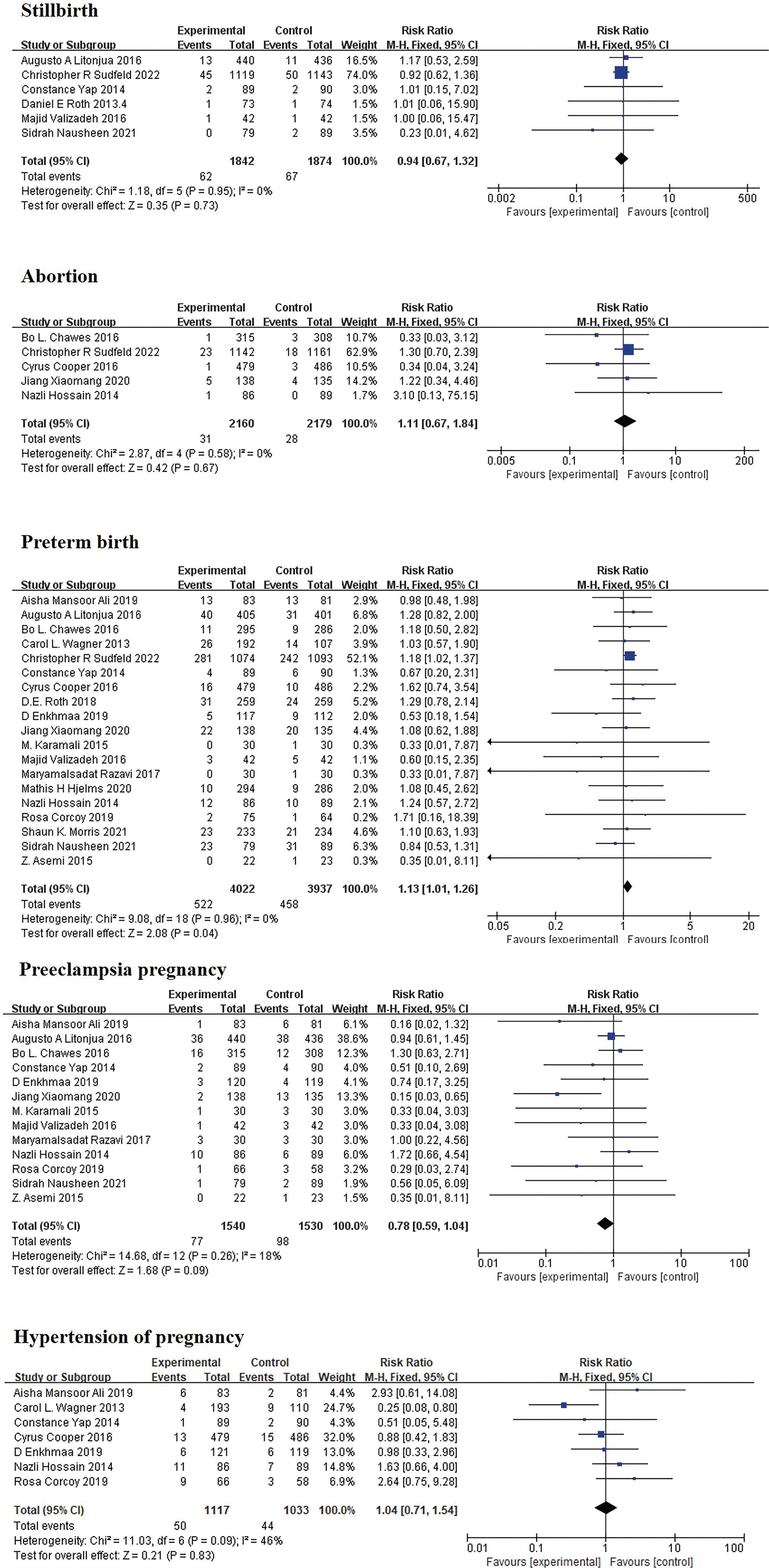
Nineteen of the 38 included RCTs reported extractable data on preterm births and were included in the primary meta-analysis involving 7959 pregnant women. The remaining 19 trials did not report preterm births and were therefore not included in this outcome-specific analysis. Overall, prenatal vitamin D supplementation was associated with a borderline increase in preterm birth risk compared to control conditions (RR = 1.13; 95% CI, 1.01–1.26; P = 0.04; I2 = 0%; Figure 4). The between-study heterogeneity was negligible for this outcome (τ2 = 0.00; Cochran’s Q = 9.08; df = 18; P = 0.96; I2 = 0%).
Figure 4 Forest plot from meta-analysis examining effect of vitamin D supplementation during pregnancy on maternal outcomes. Forest plots show the effect of vitamin D supplementation on stillbirth, abortion, preterm birth, preeclampsia, and hypertension of pregnancy. The results are presented as a risk ratio (RR) and 95% confidence interval (CI).
Exploratory subgroup analyses of preterm birth were presented as ORs using Mantel-Haenszel fixed-effect models (Figure 5). No significant association was detected among participants with a baseline 25(OH)D < 30 nmol/L in the subgroup analysis stratified by baseline 25(OH)D status (OR = 1.02; 95% CI, 0.80–1.30). In contrast, an increased preterm birth signal was noted among participants with a baseline 25(OH)D ≥ 30 nmol/L (OR = 1.25; 95% CI, 1.05–1.48). However, this subgroup result was derived entirely from one large RCT conducted among HIV-positive pregnant women and should therefore be interpreted with caution (Figure 5B).
Figure 5 Subgroup analysis of effect of vitamin D supplementation during pregnancy on preterm birth. (A) Subgroup analyses stratified by dosage of vitamin D; (B) Subgroup analyses stratified by 25-hydroxyvitamin D level; (C) Subgroup analyses stratified by timing of vitamin D supplementation. The results are presented as odds ratios (ORs) and 95% confidence intervals (CIs) using Mantel-Haenszel fixed-effect models.
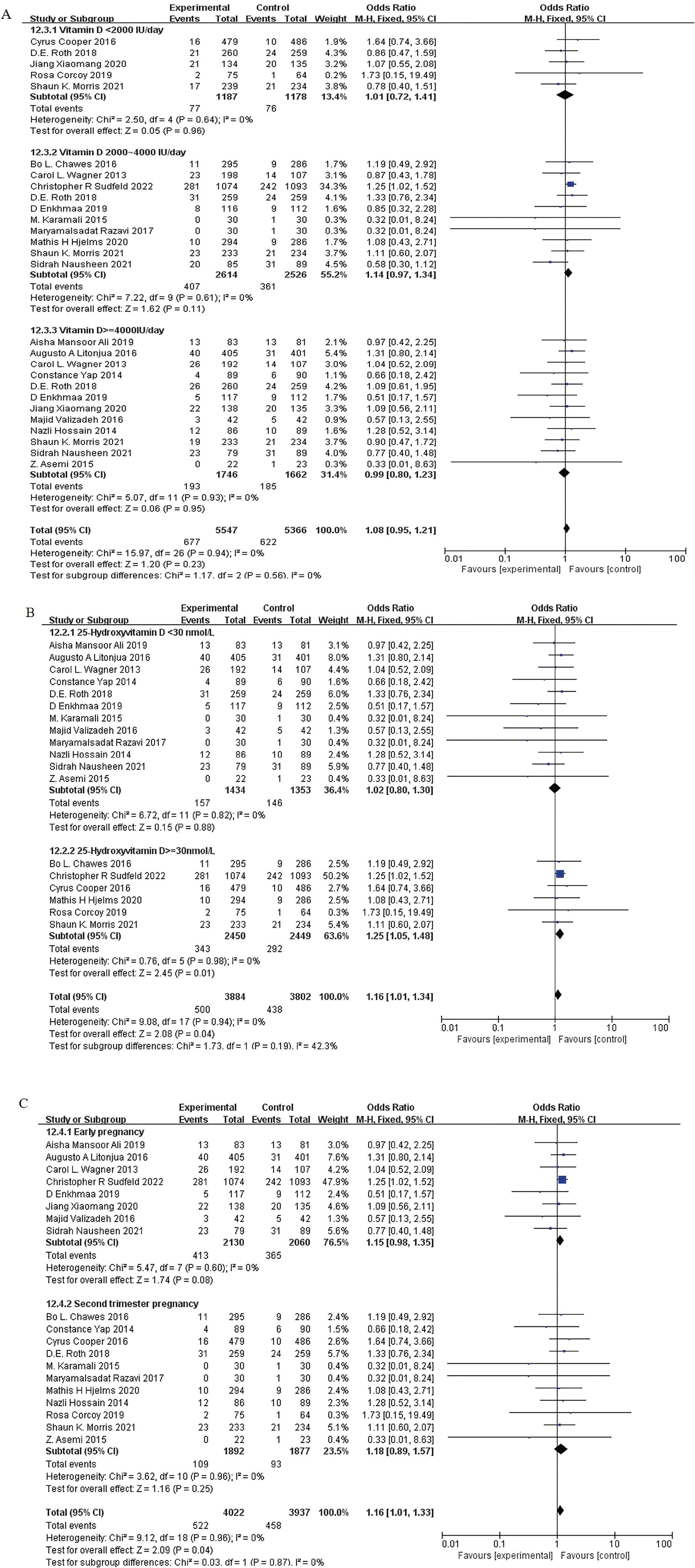
Subgroup analyses by supplementation dose showed no significant association in the < 2000 IU/d subgroup (OR = 1.01; 95% CI, 0.72–1.41; I2 = 0%), the 2000–4000 IU/d subgroup (OR = 1.14; 95% CI, 0.97–1.34; I2 = 0%), or the ≥ 4000 IU/d subgroup (OR = 0.99; 95% CI, 0.80–1.23; I2 = 0%; Figure 5A). Similarly, the subgroup analyses by timing of supplementation initiation had no significant association when supplementation was initiated in the first trimester (OR = 1.15; 95% CI, 0.98–1.35; I2 = 0%) or second trimester (OR = 1.18; 95% CI, 0.89–1.57; I2 = 0%; Figure 5C). Tests for subgroup differences were not statistically significant for supplementation dose, baseline 25(OH)D status, or timing of initiation.
Effects on secondary maternal outcomes
Vitamin D supplementation had no statistically significant effect on the following maternal secondary outcomes: stillbirth (RR = 0.94; 95% CI, 0.67–1.32; I2 = 0%); spontaneous abortion (RR = 1.11; 95% CI, 0.67–1.84; I2 = 0%); preeclampsia (RR = 0.78; 95% CI, 0.59–1.04; I2 = 18%); or gestational hypertension (RR = 1.04; 95% CI, 0.71–1.54; I2 = 46%; Figure 4). Statistical heterogeneity was moderate for gestational hypertension and negligible or low for other maternal outcomes.
Effects on secondary neonatal outcomes
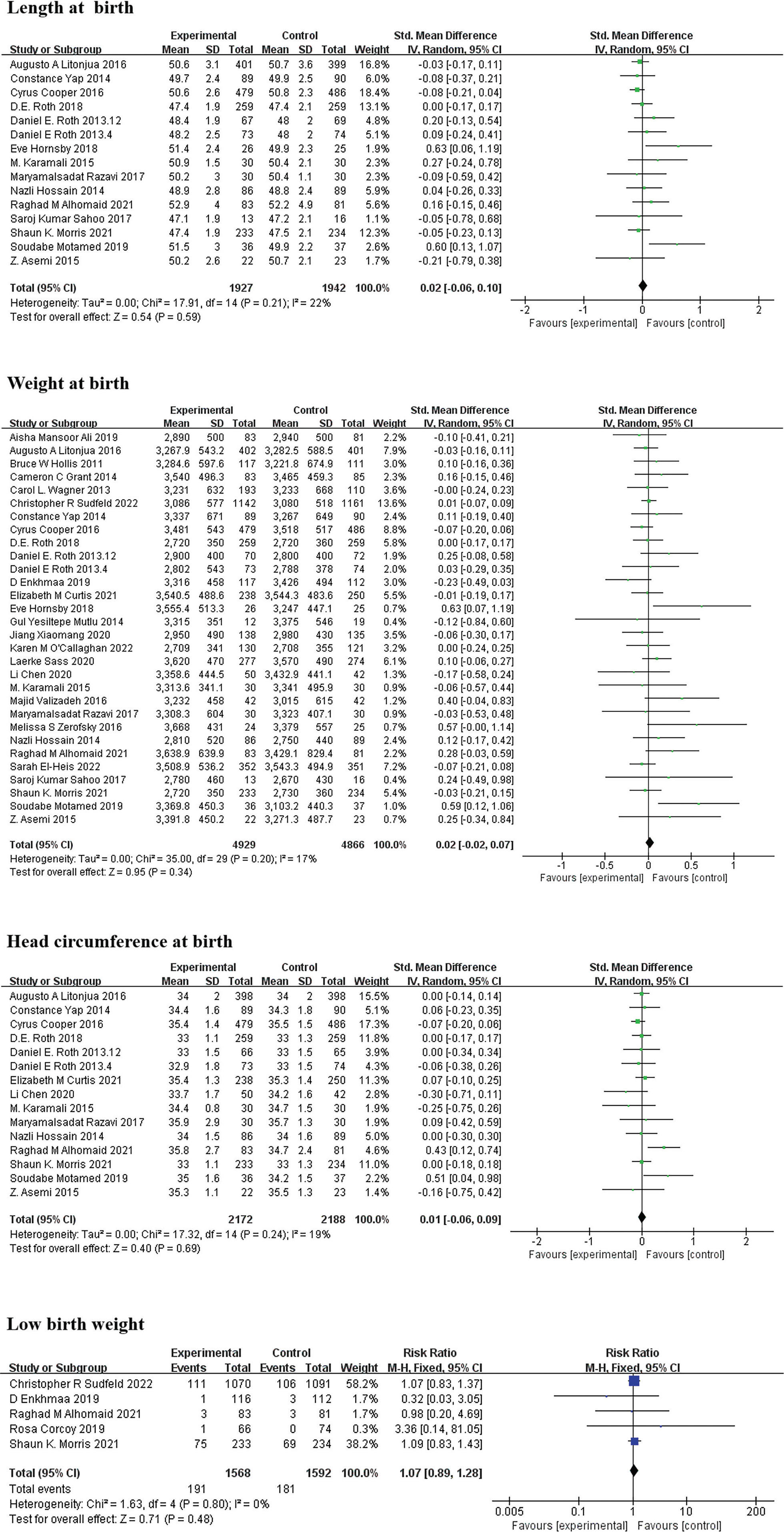
No significant differences were detected between vitamin D supplementation and control groups for the following neonatal outcomes: birth length (SMD = 0.02; 95% CI = -0.06, 0.10; I2 = 22%); birth weight (SMD = 0.02; 95% CI = -0.02, 0.07; I2 = 17%); head circumference at birth (SMD = 0.01; 95% CI = -0.06, 0.09; I2 = 19%); and low birth weight (RR = 1.07; 95% CI, 0.89–1.28; I2 = 0%; Figure 6).
Figure 6 Forest plots examining effects of prenatal vitamin D supplementation on neonatal anthropometric outcomes. (A) Length at birth; (B) Weight at birth; (C) Head circumference at birth; (D) Low birth weight. The continuous outcomes are presented as standardized mean differences (SMDs) and 95% confidence intervals (CIs); binary outcomes are presented as risk ratios (RRs) and 95% CIs.
Discussion
Prenatal vitamin D supplementation was not associated with a reduction in preterm birth or in assessed maternal and neonatal secondary outcomes in this systematic review and meta-analysis of 38 RCTs involving 17,392 pregnant women. Nineteen RCTs involving 7959 participants reported extractable data on preterm birth (the primary outcome). Primary RR-based overall analysis revealed a borderline increase in preterm birth risk but the magnitude of the association was modest, the CI was close to a null value, and the between-study heterogeneity was negligible. Importantly, the OR-based subgroup signal noted in participants with a baseline 25(OH)D ≥ 30 nmol/L was derived entirely from a single large RCT conducted among HIV-positive pregnant women, whereas no significant association was detected among participants with a baseline 25(OH)D < 30 nmol/L or in subgroups stratified by supplementation dose or timing of initiation. These findings indicate that the apparent subgroup signal should be interpreted cautiously and should not be generalized to healthy pregnant women or interpreted as evidence of causality.
Preterm birth remains a major cause of neonatal morbidity and mortality, and the etiology is complex and multifactorial, involving maternal, fetal, placental, infectious, inflammatory, anatomic, and socioeconomic factors [20]. Vitamin D has been investigated as a potentially modifiable factor because of its roles in immune regulation, placental function, and calcium homeostasis during pregnancy [10, 21]. Observational studies have reported associations between low maternal 25(OH)D concentrations and adverse pregnancy outcomes, including preterm birth, preeclampsia, and fetal growth impairment [22]. However, observational associations are vulnerable to residual confounding and cannot determine whether vitamin D supplementation alone prevents preterm birth. Consistent with this distinction, previous randomized evidence and recent evidence syntheses have generally reported neutral or inconsistent effects of prenatal vitamin D supplementation on preterm birth in general pregnant women [23]. Our findings are broadly consistent with this randomized evidence because no protective effect on preterm birth was noted overall or among participants with a baseline 25(OH)D < 30 nmol/L.
A key feature of the present analysis was stratification by baseline maternal 25(OH)D status. Baseline nutrient status is biologically and clinically relevant because response to supplementation may differ between individuals below and above the prespecified 30 nmol/L threshold, which is a central concept in precision nutrition [24]. Vitamin D supplementation was not significantly associated with preterm birth risk in the subgroup with a baseline 25(OH)D < 30 nmol/L. This finding does not exclude the possible benefits in more narrowly defined deficient populations but indicates that the currently available RCT data do not provide clear evidence that supplementation reduces preterm birth among women classified as vitamin D deficient using this threshold. The OR-based pooled estimate suggested an increased preterm birth signal in the subgroup with a baseline 25(OH)D ≥ 30 nmol/L. However, this result was based entirely on one large trial among women living with HIV and therefore may reflect population-specific factors rather than a general effect of vitamin D supplementation in pregnant women with a baseline 25(OH)D ≥ 30 nmol/L [25]. Women living with HIV may differ from general obstetric populations in immune status, infection burden, antiretroviral therapy exposure, nutritional status, and baseline risk of adverse pregnancy outcomes [26, 27]. Accordingly, this subgroup finding should be considered hypothesis-generating rather than definitive.
Absence of a clear dose-response pattern further supports cautious interpretation of the apparent subgroup signal. No significant association with preterm birth was noted in any OR-based supplementation-dose subgroup, including < 2000 IU/d, 2000–4000 IU/d, or ≥ 4000 IU/d. Similarly, supplementation initiated in the first or second trimester was not significantly associated with preterm birth risk. If vitamin D supplementation had a strong and consistent causal effect on preterm birth, a clearer pattern by dose or timing might be expected. A discrepancy between the baseline 25(OH)D subgroup results and dose-stratified results suggests that the association is unlikely to be explained by supplementation dose alone. Instead, the discrepancy may reflect baseline status, population characteristics, trial-specific factors, or chance. Therefore, the present findings cannot support dose-based recommendations for preterm birth prevention.
Vitamin D supplementation had no statistically significant effect on maternal secondary outcomes (stillbirth, spontaneous abortion, preeclampsia, or gestational hypertension). Previous mechanistic evidence suggests that vitamin D may influence immune and inflammatory regulation, endothelial-related angiogenic pathways, and placental function, all of which are implicated in the pathophysiology of preeclampsia [9]. Nevertheless, the present pooled RCT evidence did not demonstrate a significant clinical benefit for these maternal outcomes. The direction of effect for preeclampsia was toward a potential benefit but the CI crossed the null value. Therefore, this result should be interpreted as inconclusive rather than as evidence of a protective effect. Future trials may need to evaluate whether effects differ among participants with severe vitamin D deficiency, low calcium intake, high baseline risk of preeclampsia, or other clinically relevant subgroups.
Vitamin D supplementation was not associated with significant differences in neonatal outcomes (birth length, birth weight, head circumference at birth, or low birth weight). This finding is consistent with several randomized studies reporting limited, neutral, or inconsistent effects of prenatal vitamin D supplementation on fetal growth and infant anthropometric outcomes [28, 29]. Although vitamin D may affect skeletal development and neonatal vitamin D status, available trial evidence does not indicate a meaningful effect on birth-size outcomes assessed in this meta-analysis. These findings suggest that routine prenatal vitamin D supplementation should not be expected to substantially improve neonatal anthropometric indicators in unselected pregnant women.
Several biological mechanisms may explain why baseline vitamin D status could modify responses to supplementation but these mechanisms remain speculative in relation to clinical outcomes observed in this meta-analysis. Vitamin D may support maternal-fetal immune tolerance through VDR-mediated immunomodulatory mechanisms, including regulation of cytokine production, inflammatory responses, and T-cell tolerance. Vitamin D may also influence placental function through effects on trophoblast invasion and angiogenic pathways involving sFlt-1 and VEGF, which are relevant to placental development, fetal growth, and pregnancy maintenance [9]. In addition, vitamin D contributes to calcium homeostasis and may influence uterine myometrial contractile profiles through regulation of inflammation-related and contraction-associated pathways [30, 31]. These pathways provide biological plausibility for studying vitamin D status in pregnancy but do not prove that supplementation prevents or causes preterm birth. Specifically, the potential harm signal noted among participants with a baseline 25(OH)D ≥ 30 nmol/L should not be attributed to over-supplementation or hypercalcemia without direct supporting biomarker evidence. Future RCTs should incorporate mechanistic biomarkers, such as achieved 25(OH)D concentrations, calcium status, inflammatory markers, VDR-related measures, and placental function indicators, to clarify whether these pathways mediate clinical outcomes.
The clinical implications of this study should be conservative. Current evidence does not support universal vitamin D supplementation specifically for prevention of preterm birth. At the same time, the present findings do not justify contraindicating vitamin D supplementation in pregnant women who require vitamin D supplementation for deficiency correction or bone-health-related indications. A more appropriate interpretation is that the baseline 25(OH)D status may be important for individualized interpretation of supplementation effects but current trial evidence is insufficient to define clear subgroup-specific clinical recommendations. No consistent benefit was observed for women with a baseline 25(OH)D ≥ 30 nmol/L and a possible increase in preterm birth risk was limited to a single population-specific trial. Thus, decisions about prenatal vitamin D supplementation may consider baseline 25(OH)D status when clinically indicated and in accordance with local guidelines, together with clinical context, dietary intake, sun exposure, calcium status, and safety monitoring, rather than assuming universal benefit for preterm birth prevention.
This study had several strengths. First, only RCTs were included, which reduced confounding compared to observational evidence. Second, the review included 38 RCTs and incorporated recent trials, which provided an updated synthesis of prenatal vitamin D supplementation evidence. Third, we conducted prespecified subgroup analyses by baseline 25(OH)D status, supplementation dose, and timing of initiation, which allowed exploration of potential effect modification. Fourth, the primary outcome had negligible statistical heterogeneity and the funnel plot for preterm birth did not suggest obvious publication bias. Together, these features improve transparency and interpretability of pooled estimates.
Several limitations should also be acknowledged. First, the effective evidence base for primary outcome was limited. Only 19 of the 38 included RCTs reported extractable data on preterm birth and the database search was conducted up to April 2023. Although recent evidence remains mixed and does not consistently demonstrate a clear reduction in preterm birth, a fully updated systematic search and quantitative synthesis will be needed to confirm currency and robustness of present findings. Second, the apparent increased risk among participants with a baseline 25(OH)D ≥ 30 nmol/L was driven entirely by one large trial conducted among HIV-positive pregnant women, which limited generalizability to healthy pregnant women. Third, some included trials lacked placebo controls or used low-dose vitamin D as a comparator, which may have attenuated between-group differences and selective outcome reporting was incompletely described in several studies. Fourth, the subgroup analyses were limited by dichotomization of baseline 25(OH)D status, limited number of trials and events within some strata, and use of aggregate published data rather than individual participant data. These factors limited our ability to evaluate more granular 25(OH)D categories and to adjust for participant-level factors, such as achieved 25(OH)D concentration, calcium intake, body mass index, ethnicity, season, sun exposure, comorbidities, and adherence. Finally, preterm birth was analyzed as a single outcome and we could not distinguish spontaneous, medically indicated, inflammatory, infectious, or placental subtypes of preterm birth, which may have different relationships with vitamin D biology [2].
Future research should prioritize large, well-designed RCTs in diverse but clearly defined populations of pregnant women. Trials should stratify or randomize participants according to baseline 25(OH)D status, measure achieved 25(OH)D concentrations during follow-up, and report safety outcomes, including hypercalcemia and other adverse events. Future studies should also distinguish spontaneous from medically indicated preterm birth and consider mechanistic biomarkers related to immune regulation, placental function, calcium metabolism, and inflammation. Individual participant data meta-analyses of existing RCTs would be particularly valuable because such meta-analyses could evaluate dose-response relationships, baseline-status modification, achieved vitamin D levels, and clinically relevant subgroups more precisely than aggregate-data analyses. Such evidence is needed before definitive precision-nutrition recommendations for prenatal vitamin D supplementation can be made.
Conclusions
Prenatal vitamin D supplementation showed no evidence of reducing preterm birth risk or improving assessed maternal and neonatal outcomes in this systematic review and meta-analysis of 38 RCTs involving 17,392 pregnant women. Although a borderline increase in preterm birth risk was noted in the primary overall analysis and an OR-based subgroup signal was noted among participants with a baseline 25(OH)D ≥ 30 nmol/L, this signal was largely driven by a single large trial among women living with HIV and should not be interpreted as causal evidence or generalized to healthy pregnant women. Current evidence does not support universal vitamin D supplementation specifically for prevention of preterm birth. Baseline 25(OH)D status may be important for interpreting supplementation effects but current aggregate trial evidence remains insufficient to support definitive stratified clinical recommendations. Future large-scale RCTs in diverse healthy pregnant women and individual participant data meta-analyses are needed to clarify whether baseline vitamin D status modifies effect of supplementation on pregnancy outcomes.
Abbreviations
RCTs, randomized controlled trials; 25(OH)D, 25-hydroxyvitamin D; RR, risk ratio; CI, confidence interval; HIV, human immunodeficiency virus; 1,25(OH)2D3, 1,25-dihydroxyvitamin D3; VDR, vitamin D receptor; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PROSPERO, International Prospective Register of Systematic Reviews; PICOS, population, intervention, comparison, outcome, and study design; MeSH, Medical Subject Headings; GRADE, Grading of Recommendations Assessment, Development and Evaluation; SMD, standardized mean difference; OR, odds ratio.
Data availability statement
All data analyzed in this study were extracted from previously published articles cited in the References. The extracted datasets used for the current systematic review and meta-analysis are available from the corresponding author upon reasonable request.
Ethics statement
No direct interactions with human or animal subjects were involved. Therefore, ethical approval and informed consent were not required.
Author contributions
Lulu Zuo, Jiaojiao Wang, and Qiong Lu conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript. Xinyan Xie and Mei Peng designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript. Zhaokai Zhou critically reviewed and revised the manuscript. Qiyue Zheng conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors were grateful for the support from the National Key R&D Program of China (Grant Nos. 2020YFC2009000 and 2020YFC2009001), the Hunan Provincial Department of Finance Grant (2022-151, 2021-139, 2020-83, 2019-93, and 2018-92), Hunan Provincial Development and Reform Commission of Innovative Research Program (2021-212-23), Hunan Innovative Province Construction Special Project (2021ZK4025), and Natural Science Foundation of Hunan Province (2024JJ5494 and 2024JJ9203), the Scientific Research Program of Hunan Provincial Health Commission under Grant (D202303106778), and the Natural Science Foundation of Changsha (kq2208340).
Acknowledgment
Not applicable.
Conflict of interest
The authors declare that there are no conflicts of interest.
Supplementary materials
Supplementary Material can be downloaded from https://bio-integration.org/wp-content/uploads/2026/07/bioi20250224_Supplemental.zip.
Graphical abstract
Highlights
- Prenatal vitamin D supplementation was evaluated using randomized controlled trial evidence.
- The review focused on preterm birth and maternal-neonatal secondary outcomes.
- Subgroup interpretation considered baseline 25(OH)D status, dose, and timing of initiation.
- Current evidence does not support universal vitamin D supplementation specifically for preterm birth prevention.
- Individualized interpretation should consider baseline vitamin D status, clinical context, and local guidelines.
Brief statement
This systematic review and meta-analysis evaluates randomized evidence on prenatal vitamin D supplementation in relation to preterm birth and maternal-neonatal outcomes, emphasizing cautious interpretation according to baseline 25(OH)D status, supplementation dose, and timing of initiation.
References
- WHO: recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet Gynecol Scand 1977;56(3):247-53. [PMID: 560099]
- Villar J, Cavoretto PI, Barros FC, Romero R, Papageorghiou AT, et al. Etiologically based functional taxonomy of the preterm birth syndrome. Clin Perinatol 2024;51(2):475-95. [PMID: 38705653 DOI: 10.1016/j.clp.2024.02.014]
- Tingleff T, Räisänen S, Vikanes Å, Sandvik L, Sugulle M, et al. Different pathways for preterm birth between singleton and twin pregnancies: a population-based registry study of 481 176 nulliparous women. Br J Obstet Gynaecol 2023;130(4):387-95. [PMID: 36372962 DOI: 10.1111/1471-0528.17344]
- Chawanpaiboon S, Vogel JP, Moller AB, Lumbiganon P, Petzold M, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health 2019;7(1):e37-46. [PMID: 30389451 DOI: 10.1016/S2214-109X(18)30451-0]
- Deng K, Liang J, Mu Y, Liu Z, Wang Y, et al. Preterm births in China between 2012 and 2018: an observational study of more than 9 million women. Lancet Glob Health 2021;9(9):e1226-41. [PMID: 34416213 DOI: 10.1016/S2214-109X(21)00298-9]
- Bérard A, Le Tiec M, De Vera MA. Study of the costs and morbidities of late-preterm birth. Arch Dis Child Fetal Neonatal Ed 2012;97(5):F329-34.
- Korvenranta E, Lehtonen L, Rautava L, Häkkinen U, Andersson S, et al. Impact of very preterm birth on health care costs at five years of age. Pediatrics 2010;125(5):e1109-14. [PMID: 20368320 DOI: 10.1542/peds.2009-2882]
- Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet 2008;371(9606):75-84. [PMID: 18177778 DOI: 10.1016/S0140-6736(08)60074-4]
- Karras SN, Wagner CL, Castracane VD. Understanding vitamin D metabolism in pregnancy: from physiology to pathophysiology and clinical outcomes. Metabolism 2018;86:112-23. [PMID: 29066285 DOI: 10.1016/j.metabol.2017.10.001]
- Cyprian F, Lefkou E, Varoudi K, Girardi G. Immunomodulatory effects of vitamin D in pregnancy and beyond. Front Immunol 2019;10:2739. [PMID: 31824513 DOI: 10.3389/fimmu.2019.02739]
- Roth DE. Vitamin D supplementation during pregnancy: safety considerations in the design and interpretation of clinical trials. J Perinatol 2011;31(7):449-59. [PMID: 21252966 DOI: 10.1038/jp.2010.203]
- Bouillon R, Manousaki D, Rosen C, Trajanoska K, Rivadeneira F, et al. The health effects of vitamin D supplementation: evidence from human studies. Nat Rev Endocrinol 2022;18(2):96-110. [PMID: 34815552 DOI: 10.1038/s41574-021-00593-z]
- De-Regil LM, Palacios C, Lombardo LK, Pena-Rosas JP. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst Rev 2016;(1):CD008873. [PMID: 26765344 DOI: 10.1002/14651858.CD008873.pub3]
- Aglipay M, Birken CS, Parkin PC, Loeb MB, Thorpe K, et al. Effect of high-dose vs standard-dose wintertime vitamin D supplementation on viral upper respiratory tract infections in young healthy children. J Am Med Assoc 2017;318(3):245-54. [PMID: 28719693 DOI: 10.1001/jama.2017.8708]
- Ganmaa D, Uyanga B, Zhou X, Gantsetseg G, Delgerekh B, et al. Vitamin D supplements for prevention of tuberculosis infection and disease. N Engl J Med 2020;383(4):359-68. [PMID: 32706534 DOI: 10.1056/NEJMoa1915176]
- Zeisel SH. Precision (personalized) nutrition: understanding metabolic heterogeneity. Annu Rev Food Sci Technol 2020;11:71-92. [PMID: 31928426 DOI: 10.1146/annurev-food-032519-051736]
- Roth DE, Leung M, Mesfin E, Qamar H, Watterworth J, et al. Vitamin D supplementation during pregnancy: state of the evidence from a systematic review of randomised trials. Br Med J 2017;359:j5237. [PMID: 29187358 DOI: 10.1136/bmj.j5237]
- Mansur JL, Oliveri B, Giacoia E, Fusaro D, Costanzo PR. Vitamin D: before, during and after pregnancy: effect on neonates and children. Nutrients 2022;14(9):1900. [PMID: 35565867 DOI: 10.3390/nu14091900]
- Palacios C, Kostiuk LL, Cuthbert A, Weeks J. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst Rev 2024;7(7):CD008873. [PMID: 39077939 DOI: 10.1002/14651858.CD008873.pub5]
- Dudley DJ, Ennen CS. The vexing problem of preterm birth prevention. J Am Med Assoc 2023;330(4):323-5. [PMID: 37490098 DOI: 10.1001/jama.2023.7244]
- Demay MB, Pittas AG, Bikle DD, Diab DL, Kiely ME, et al. Vitamin D for the prevention of disease: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2024;109(8):1907-47. [PMID: 38828931 DOI: 10.1210/clinem/dgae290]
- Tous M, Villalobos M, Iglesias-Vazquez L, Fernandez-Barres S, Arija V. Vitamin D status during pregnancy and offspring outcomes: a systematic review and meta-analysis of observational studies. Eur J Clin Nutr 2020;74(1):36-53. [PMID: 30683894 DOI: 10.1038/s41430-018-0373-x]
- Kiely ME, Wagner CL, Roth DE. Vitamin D in pregnancy: where we are and where we should go. J Steroid Biochem Mol Biol 2020;201:105669. [PMID: 32302652 DOI: 10.1016/j.jsbmb.2020.105669]
- Mavar M, Sorić T, Bagarić E, Sarić A, Matek Sarić M. The power of vitamin D: is the future in precision nutrition through personalized supplementation plans? Nutrients 2024;16(8):1176. [PMID: 38674867 DOI: 10.3390/nu16081176]
- Sudfeld CR, Manji KP, Muhihi A, Duggan CP, Aboud S, et al. Vitamin D3 supplementation during pregnancy and lactation for women living with HIV in Tanzania: a randomized controlled trial. PLoS Med 2022;19(4):e1003973. [PMID: 35427363 DOI: 10.1371/journal.pmed.1003973]
- Selph SS, Bougatsos C, Dana T, Grusing S, Chou R. Screening for HIV infection in pregnant women: updated evidence report and systematic review for the US Preventive Services Task Force. J Am Med Assoc 2019;321(23):2349-60. [PMID: 31184704 DOI: 10.1001/jama.2019.2593]
- Harris K, Yudin MH. HIV infection in pregnant women: a 2020 update. Prenat Diagn 2020;40(13):1715-21. [PMID: 33405240 DOI: 10.1002/pd.5769]
- Roth DE, Morris SK, Zlotkin S, Gernand AD, Ahmed T, et al. Vitamin D supplementation in pregnancy and lactation and infant growth. N Engl J Med 2018;379(6):535-46. [PMID: 30089075 DOI: 10.1056/NEJMoa1800927]
- Vaziri F, Dabbaghmanesh MH, Samsami A, Nasiri S, Shirazi PT. Vitamin D supplementation during pregnancy on infant anthropometric measurements and bone mass of mother-infant pairs: A randomized placebo clinical trial. Early Hum Dev 2016;103:61-8. [PMID: 27513714 DOI: 10.1016/j.earlhumdev.2016.07.011]
- Thota C, Laknaur A, Farmer T, Ladson G, Al-Hendy A, et al. Vitamin D regulates contractile profile in human uterine myometrial cells via NF-κB pathway. Am J Obstet Gynecol 2014;210(4):347.e1-10. [PMID: 24262718 DOI: 10.1016/j.ajog.2013.11.027]
- Sanborn BM. Hormones and calcium: mechanisms controlling uterine smooth muscle contractile activity. The Litchfield Lecture. Exp Physiol 2001;86(2):223-37. [PMID: 11429639 DOI: 10.1113/eph8602179]
- Ali AM, Alobaid A, Malhis TN, Khattab AF. Effect of vitamin D3 supplementation in pregnancy on risk of pre-eclampsia – randomized controlled trial. Clin Nutr 2019;38(2):557-63. [PMID: 29550150 DOI: 10.1016/j.clnu.2018.02.023]
- Litonjua AA, Carey VJ, Laranjo N, Stubbs BJ, Mirzakhani H, et al. Six-year follow-up of a trial of antenatal vitamin D for asthma reduction. N Engl J Med 2020;382(6):525-33. [PMID: 32023372 DOI: 10.1056/NEJMoa1906137]
- Litonjua AA, Carey VJ, Laranjo N, Harshfield BJ, McElrath TF, et al. Effect of prenatal supplementation with vitamin D on asthma or recurrent wheezing in offspring by age 3 years: the VDAART Randomized Clinical Trial. J Am Med Assoc 2016;315(4):362-70. [PMID: 26813209 DOI: 10.1001/jama.2015.18589]
- Chawes BL, Bonnelykke K, Stokholm J, Vissing NH, Bjarnadottir E, et al. Effect of vitamin D-3 supplementation during pregnancy on risk of persistent wheeze in the offspring: a randomized clinical trial. J Am Med Assoc 2016;315(4):353-61. [PMID: 26813208 DOI: 10.1001/jama.2015.18318]
- Hollis BW, Johnson D, Hulsey TC, Ebeling M, Wagner CL. Vitamin D supplementation during pregnancy: double-blind, randomized clinical trial of safety and effectiveness. J Bone Miner Res 2011;26(10):2341-57. [PMID: 21706518 DOI: 10.1002/jbmr.463]
- Grant CC, Stewart AW, Scragg R, Milne T, Rowden J, et al. Vitamin D during pregnancy and infancy and infant serum 25-hydroxyvitamin D concentration. Pediatrics 2014;133(1):E143-53. [PMID: 24344104 DOI: 10.1542/peds.2013-2602]
- Wagner CL, McNeil R, Hamilton SA, Winkler J, Cook CR, et al. A randomized trial of vitamin D supplementation in 2 community health center networks in South Carolina. Am J Obstet Gynecol 2013;208(2):137.e1-13. [PMID: 23131462 DOI: 10.1016/j.ajog.2012.10.888]
- Wall CR, Stewart AW, Camargo CA, Jr, Scragg R, Mitchell EA, et al. Vitamin D activity of breast milk in women randomly assigned to vitamin D3 supplementation during pregnancy. Am J Clin Nutr 2016;103(2):382-8. [PMID: 26702121 DOI: 10.3945/ajcn.115.114603]
- Yap C, Cheung NW, Gunton JE, Athayde N, Munns CF, et al. Vitamin D supplementation and the effects on glucose metabolism during pregnancy: a randomized controlled trial. Diabetes Care 2014;37(7):1837-44. [PMID: 24760259 DOI: 10.2337/dc14-0155]
- Cooper C, Harvey NC, Bishop NJ, Kennedy S, Papageorghiou AT, et al. Maternal gestational vitamin D supplementation and off spring bone health (MAVIDOS): a multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol 2016;4(5):393-402. [PMID: 26944421 DOI: 10.1016/S2213-8587(16)00044-9]
- Enkhmaa D, Tanz L, Ganmaa D, Enkhtur S, Oyun-Erdene B, et al. Randomized trial of three doses of vitamin D to reduce deficiency in pregnant Mongolian women. EBioMedicine 2019;39:510-9. [PMID: 30552064 DOI: 10.1016/j.ebiom.2018.11.060]
- Roth DE, Perumal N, Al Mahmud A, Baqui AH. Maternal vitamin D3 supplementation during the third trimester of pregnancy: effects on infant growth in a longitudinal follow-up study in Bangladesh. J Pediatr 2013;163(6):1605-11.e3. [PMID: 23998516 DOI: 10.1016/j.jpeds.2013.07.030]
- Roth DE, Al Mahmud A, Raqib R, Akhtar E, Perumal N, et al. Randomized placebo-controlled trial of high-dose prenatal third-trimester vitamin D3 supplementation in Bangladesh: the AViDD trial. Nutr J 2013;12:47. [PMID: 23587190 DOI: 10.1186/1475-2891-12-47]
- Curtis EM, Parsons C, Maslin K, D’Angelo S, Moon RJ, et al. Bone turnover in pregnancy, measured by urinary CTX, is influenced by vitamin D supplementation and is associated with maternal bone health: findings from the Maternal Vitamin D Osteoporosis Study (MAVIDOS) trial. Am J Clin Nutr 2021;114(5):1600-11. [PMID: 34297067 DOI: 10.1093/ajcn/nqab264]
- Hornsby E, Pfeffer PE, Laranjo N, Cruikshank W, Tuzova M, et al. Vitamin D supplementation during pregnancy: Effect on the neonatal immune system in a randomized controlled trial. J Allergy Clin Immunol 2018;141(1):269-78.e1. [PMID: 28552588 DOI: 10.1016/j.jaci.2017.02.039]
- Mutlu GY, Ozsu E, Kalaca S, Yuksel A, Pehlevan Y, et al. Evaluation of vitamin D supplementation doses during pregnancy in a population at high risk for deficiency. Horm Res Paediatr 2014;81(6):402-8. [PMID: 24714660 DOI: 10.1159/000358833]
- Xiaomang J, Yanling W. Effect of vitamin D3 supplementation during pregnancy on high risk factors – a randomized controlled trial. J Perinat Med 2021;49(4):480-4. [PMID: 33554587 DOI: 10.1515/jpm-2020-0318]
- March KM, Chen NN, Karakochuk CD, Shand AW, Innis SM, et al. Maternal vitamin D3 supplementation at 50 μg/d protects against low serum 25-hydroxyvitamin D in infants at 8 wk of age: a randomized controlled trial of 3 doses of vitamin D beginning in gestation and continued in lactation. Am J Clin Nutr 2015;102(2):402-10. [PMID: 26156737 DOI: 10.3945/ajcn.114.106385]
- O’Callaghan KM, Shanta SS, Fariha F, Harrington J, Mahmud AA, et al. Effect of maternal prenatal and postpartum vitamin D supplementation on offspring bone mass and muscle strength in early childhood: follow-up of a randomized controlled trial. Am J Clin Nutr 2022;115(3):770-80. [PMID: 34849536 DOI: 10.1093/ajcn/nqab396]
- Sass L, Vinding RK, Stokholm J, Bjarnadóttir E, Noergaard S, et al. High-dose vitamin D supplementation in pregnancy and neurodevelopment in childhood: a prespecified secondary analysis of a randomized clinical trial. JAMA Netw Open 2020;3(12):e2026018. [PMID: 33289844 DOI: 10.1001/jamanetworkopen.2020.26018]
- Chen L, Wagner CL, Dong Y, Wang X, Shary JR, et al. Effects of maternal vitamin D3 supplementation on offspring epigenetic clock of gestational age at birth: a post-hoc analysis of a randomized controlled trial. Epigenetics 2020;15(8):830-40. [PMID: 32089064 DOI: 10.1080/15592294.2020.1734148]
- Karamali M, Beihaghi E, Mohammadi AA, Asemi Z. Effects of high-dose vitamin D supplementation on metabolic status and pregnancy outcomes in pregnant women at risk for pre-eclampsia. Horm Metab Res 2015;47(12):867-72. [PMID: 25938886 DOI: 10.1055/s-0035-1548835]
- Valizadeh M, Piri Z, Mohammadian F, Kamali K, Amir Moghadami HR. The impact of vitamin D supplementation on post-partum glucose tolerance and insulin resistance in gestational diabetes: a randomized controlled trial. Int J Endocrinol Metab 2016;14(2):e34312. [PMID: 27679649 DOI: 10.5812/ijem.34312]
- Razavi M, Jamilian M, Samimi M, Afshar Ebrahimi F, Taghizadeh M, et al. The effects of vitamin D and omega-3 fatty acids co-supplementation on biomarkers of inflammation, oxidative stress and pregnancy outcomes in patients with gestational diabetes. Nutr Metab (Lond) 2017;14:80. [PMID: 29299042 DOI: 10.1186/s12986-017-0236-9]
- Hjelmsø MH, Shah SA, Thorsen J, Rasmussen M, Vestergaard G, et al. Prenatal dietary supplements influence the infant airway microbiota in a randomized factorial clinical trial. Nat Commun 2020;11(1):426. [DOI: 10.1038/s41467-020-14308-x]
- Zerofsky M, Jacoby B, Pedersen TL, Stephensen CB. Effects of a randomized, controlled trial of daily vitamin D3 supplementation during pregnancy on regulatory immunity and inflammation. FASEB J 2016;30(S1):296.7. [DOI: 10.1096/fasebj.30.1_supplement.296.7]
- Hossain N, Kanani FH, Ramzan S, Kausar R, Ayaz S, et al. Obstetric and neonatal outcomes of maternal vitamin D supplementation: results of an open-label, randomized controlled trial of antenatal vitamin D supplementation in Pakistani women. J Clin Endocrinol Metab 2014;99(7):2448-55. [PMID: 24646102 DOI: 10.1210/jc.2013-3491]
- Alhomaid RM, Mulhern MS, Strain J, Laird E, Healy M, et al. Maternal obesity and baseline vitamin D insufficiency alter the response to vitamin D supplementation: a double-blind, randomized trial in pregnant women. Am J Clin Nutr 2021;114(3):1208-18. [PMID: 33964855 DOI: 10.1093/ajcn/nqab112]
- Corcoy R, Mendoza LC, Simmons D, Desoye G, Adelantado JM, et al. The DALI vitamin D randomized controlled trial for gestational diabetes mellitus prevention: no major benefit shown besides vitamin D sufficiency. Clin Nutr 2020;39(3):976-84. [PMID: 31053513 DOI: 10.1016/j.clnu.2019.04.006]
- El-Heis S, D’Angelo S, Curtis EM, Healy E, Moon RJ, et al. Maternal antenatal vitamin D supplementation and offspring risk of atopic eczema in the first 4 years of life: evidence from a randomized controlled trial. Br J Dermatol 2022;187(5):659-66. [PMID: 35763390 DOI: 10.1111/bjd.21721]
- Sahoo SK, Katam KK, Das V, Agarwal A, Bhatia V. Maternal vitamin D supplementation in pregnancy and offspring outcomes: a double-blind randomized placebo-controlled trial. J Bone Miner Metab 2017;35(4):464-71. [PMID: 27628045 DOI: 10.1007/s00774-016-0777-4]
- Morris SK, Pell LG, Rahman MZ, Mahmud AA, Shi J, et al. Effects of maternal vitamin D supplementation during pregnancy and lactation on infant acute respiratory infections: follow-up of a randomized trial in Bangladesh. J Pediatric Infect Dis Soc 2021;10(9):901-9. [PMID: 34213544 DOI: 10.1093/jpids/piab032]
- Nausheen S, Habib A, Bhura M, Rizvi A, Shaheen F, et al. Impact evaluation of the efficacy of different doses of vitamin D supplementation during pregnancy on pregnancy and birth outcomes: a randomised, controlled, dose comparison trial in Pakistan. BMJ Nutr Prev Health 2021;4(2):425-34. [PMID: 35028513 DOI: 10.1136/bmjnph-2021-000304]
- Motamed S, Nikooyeh B, Kashanian M, Hollis BW, Neyestani TR. Efficacy of two different doses of oral vitamin D supplementation on inflammatory biomarkers and maternal and neonatal outcomes. Matern Child Nutr 2019;15(4):e12867. [PMID: 31250540 DOI: 10.1111/mcn.12867]
- Goldring ST, Griffiths CJ, Martineau AR, Robinson S, Yu C, et al. Prenatal vitamin D supplementation and child respiratory health: a randomised controlled trial. PLoS One 2013;8(6):e66627. [PMID: 23826104 DOI: 10.1371/journal.pone.0066627]
- Asemi Z, Esmaillzadeh A. The effect of multi mineral-vitamin D supplementation on pregnancy outcomes in pregnant women at risk for pre-eclampsia. Int J Prev Med 2015;6:62. [PMID: 26288706 DOI: 10.4103/2008-7802.160975]