Ocular Delivery: Innovations in Ocular Inserts, Contact Lenses, and Microneedles
1Department of Pharmaceutics, Amity University Uttar Pradesh Lucknow campus, Lucknow 226028, India
*Correspondence to: Dr. Nimisha Srivastava, Professor (Pharmaceutics), Department of Pharmaceutics, Amity Institute of Pharmacy, Amity University Uttar Pradesh Lucknow campus, Lucknow 226028, India, Mobile: +91-9453915980, E-mail: nsrivastava3@lko.amity.edu
Received: July 11 2025; Revised: August 29 2025; Accepted: December 20 2025; Published Online: April 1 2026
Cite this paper:
Samanta S, Srivastava N. Ocular Delivery: Innovations in Ocular Inserts, Contact Lenses, and Microneedles. BIO Integration 2026; 7: 1–25.
DOI: 10.15212/bioi-2025-0128. Available at: https://bio-integration.org/
Download citation
© 2026 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Ocular drug delivery systems are essential for treating various eye conditions. Ocular conventional drug delivery techniques, such as eye drops (topical administration), often face challenges, like rapid drainage and low bioavailability. To overcome these challenges, scientists have developed ocular inserts with sustained delivery systems. Biocompatible materials, such as hydrogels, polymers, and biodegradable nanoparticles, have been investigated for insert manufacturing. These materials provide controlled release, improved retention time in the outer surface of the eye, and enhanced penetration of active pharmaceutical ingredients passing through the corneal barrier. Innovations in contact lens technology have made it possible to develop drug-loaded lenses that can deliver drugs in a sustained manner directly to the ocular surface by enhancing drug retention time and therapeutic efficacy. Microneedle-based ocular delivery, a relatively new methodology, has made progress by open-hollow and biodegradable microneedles that permit minimally invasive penetration to the sclera or cornea. Microneedle-based ocular delivery provides high bioavailability with prolonged release of drugs. The introduction of smart polymers, nanotechnology, and 3D printing with these systems has enhanced accuracy, patient comfort, and therapeutic efficacy. Together, these advances represent an evolution from current topical ocular treatment options to long-acting, patient-comfort ocular therapies with high efficacy and accuracy.
Keywords
Contact lenses; glaucoma; hydrogels; intravitreal injection; microneedles.
Introduction
Ocular drug delivery systems deliver active pharmaceutical agents to the eye to treat various diseases or disorders. Ocular drug delivery represents one of the most challenging, yet indispensable interests in pharmaceutical research [1]. The main objective of ocular drug delivery systems is to treat diseases and disorders in a localized manner. Several drug delivery systems have a unique feature in which drugs are delivered in a site-specific manner, but due to the complex physiology and anatomy of the eye, ocular drug delivery is difficult [2–4].
The eye is a unique organ in the body with a complex anatomic structure and physiology. The eye contains various biological barriers that perform different independent functions and make it highly resistant to foreign objects [5]. The cornea and lens are two parts of the eye that do not have a blood supply. The strong connections between the corneal epithelium and the mucosal surface protect the interior components and tissues of the eye from the outside world. The stroma contains hydrophilic cells which act as a barrier to hydrophobic drugs. The main challenge for ocular drug delivery is to pass through these protective barriers and ensure that the drug reaches the intraocular tissues to achieve a therapeutic effect. Most of the applied drugs are washed out by lacrimal fluid and tear secretions. Indeed, <5% of a drug enters the deeper layer of the eye. For this reason, researchers try to deliver ocular drugs to the specific target tissue at a specific therapeutic dose [6].
The bioavailability of drugs administered through the ocular route depends on physicochemical properties of the drug and physiologic factors. The physiologic factors are protein binding, drug metabolism, and lacrimal drainage [7]. Topical application of drugs is mainly used to treat various eye diseases, like eye flu, dryness, redness, and conjunctival infections. Greater than 70% of over-the-counter ophthalmic dosage forms are in the form of eye drops. Anti-inflammatory medications, antibacterial medications, and angiogenesis inhibitors are most likely utilized to treat different kinds of local infections in the eyes. Recent advanced ocular drug delivery systems are improving drug bioavailability, residence time, and drug penetration. Advanced ocular drug delivery systems also minimize toxicity with some modifications, including novel formulations, like nanoparticles, liposomes, hydrogels, and in situ gels that release the active ingredients more accurately into the target ocular tissues. These dosage forms are commonly used for treatment of anterior and posterior segments of the eye. Moreover, ocular inserts, implants, and contact lenses with drug reservoirs are new strategies designed as alternatives to conventional methods. For example, diclofenac sodium is an anti-inflammatory drug that is used to prepare diclofenac sodium ocular inserts. Gene therapy, exosomes, and self-nano emulsifying drug delivery systems (SNEDDS) have been introduced in current treatments, which illustrates the technologic advances in ocular drug delivery.
Approximately 2.2 billion people are affected by visual impairment, according to the World Health Organization (WHO). Polymeric nanoparticles efficiently target conditions, such as age-related macular degeneration, cytomegalovirus (CMV) retinitis, diabetic retinopathy, posterior uveitis, and retinitis pigmentosa in the posterior portion of the eye. These nanoparticles can be used in the form of eye drops in place of semisolid ointments to reduce discomfort and blurred vision in the extra outer part of the eye [8]. Currently, the therapeutic potential of biodegradable polymers for ocular delivery are being investigated in in vitro and in vivo studies. Notably, these drug-loaded biodegradable formulations have various limitations, such as difficulty in drug loading, high cost, ocular irritation, and stability issues [9]. Stem cell therapy is one of the important treatments for ocular problems in which damaged ocular tissues are regenerated. Personalized ocular delivery systems, which treat ocular diseases in individual patients according to gene structure, gene types, lifestyle, and environment factors, are also being developed. The main aim of personalised medicine is to reduce the toxicity and side effects of pharmaceuticals [10].
In this review we focused on recent advances in ocular drug delivery system. First, the anatomy of the eye is reviewed and main challenges of ocular drug delivery systems are introduced. Then, the process to overcome the different barriers to ocular drug delivery systems are discussed. The present review provides a comprehensive overview of ocular inserts, ocular lenses, and ocular microneedles.
Merits of ocular drug delivery systems
- Drug delivery systems provide direct delivery of drugs to the eye which helps to achieve high drug concentration at the targeted site.
- Traditional routes of drug delivery face challenges due to the presence of various barriers but ocular delivery systems can bypass these barriers and enhance bioavailability.
- Drug delivery systems have local therapeutic actions, which does not allow any drug to reach the systemic circulation. Drug delivery systems reduce side effects in other parts of the body.
- Drug delivery systems provide controlled and sustained release of drugs, which reduces dosing frequency.
- Ocular drug delivery methods, like encapsulation of nanoparticles and liposomes, protect medication from environmental factors [11].
- Some drug delivery systems are prepared to deliver genetic materials, like DNA and RNA, to treat genetic eye disorders.
- Drug delivery systems are easy to self-administer.
- Drug delivery systems increase the residence time of drug in the eye.
- Drug delivery systems provide better housing of delivery systems [12].
Limitations of conventional ocular drug delivery systems
Ocular delivery systems have been limited by the following limitations, which are:
- The eye has natural defence systems, such as tears, blinking, nasolacrimal drainage, and enzymatic degradation, which significantly limits the retention and absorption (approximately 5% drug can reach the target site only) of drugs on the ocular surface. [11].
- Frequent dosing results in patient non-compliance, especially in chronic conditions, like glaucoma [12]. To overcome these challenges, recent innovations, like nanotechnology and polymer-based systems, have been developed but these systems also face significant challenges. The actual use of nanotechnology-based delivery in the hospital setting is limited by concerns over safety, scalability, and regulatory aspects [5], while polymeric systems (hydrogels and microneedles) face challenges in manufacturing complexity and patient tolerability [13].
- Intravitreal injections provide direct delivery to the posterior segment but are invasive, painful, and carry risks of complications, like infections and retinal detachment [14].
- Emerging technologies, like smart contact lenses and biodegradable implants, promise controlled drug release. However, widespread adoption is constrained by high costs, regulatory requirements, and limited long-term safety data [15].
Anatomy of the eye
The eye is a complex organ made up of various sensitive tissues. The anatomy of the eye is an obstacle to drug delivery systems because some parts impede drug absorption and distribution [16]. The anatomic structure of the eyeball is divided into two parts:
- anterior segment (cornea, conjunctiva, iris, ciliary body, aqueous humor, and lens); and
- posterior segment (sclera, choroid, retina, and vitreous body).
Cornea
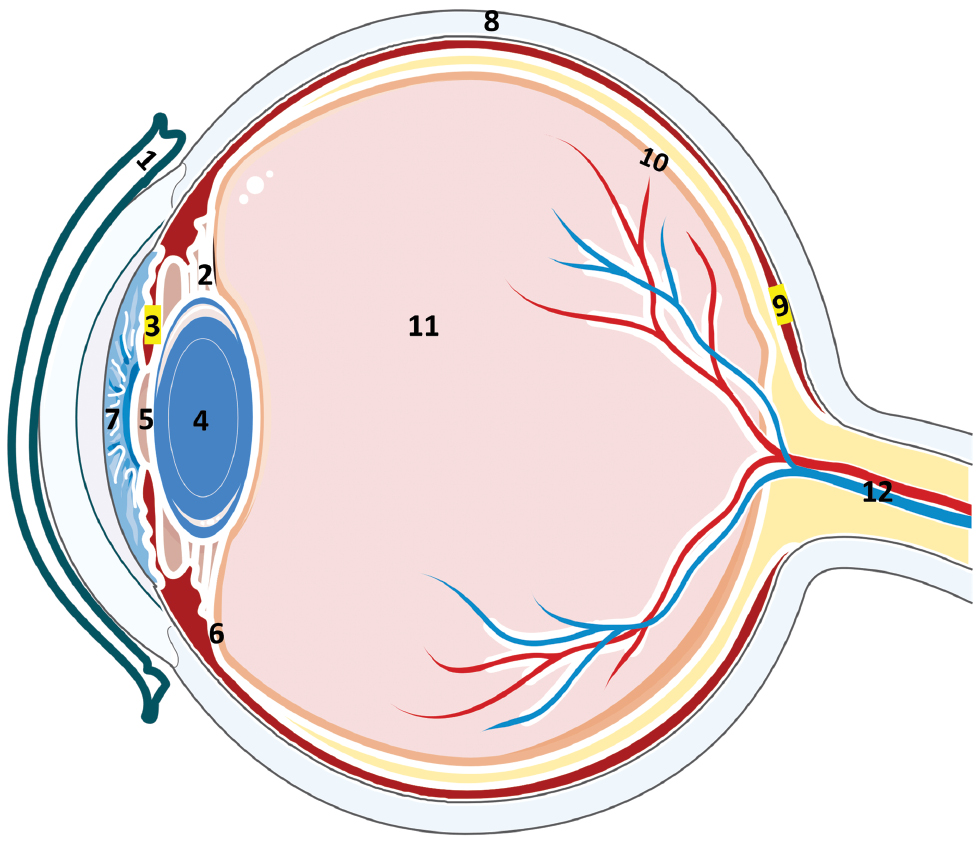
The cornea is a clear, transparent, outer layer of the eye that covers the iris (the colored part of the eye), pupil (the opening in the center of this layer), and anterior chamber (Figure 1) [17]. The cornea is avascular with the following five layers: epithelium; Bowman’s membrane; stroma; Descemet’s membrane; and endothelium. The corneal epithelium contains tight junctions in the surface layer [18]. CYP450 and a drug efflux pump is present in the epithelial cell layer, which reduces the bioavailability of drugs. Gap junctions are also present in the aqueous layer, which act as a leakage barrier. Gap junctions are lipophilic in nature and do not allow penetration of hydrophilic drugs. Gap junctions are the biggest obstacle of drug penetration [19].
Figure 1 Schematic presentation of the eye (1. conjunctiva, 2. ciliary body, 3. iris, 4. lens, 5. pupil, 6. suspensory ligament, 7. aqueous humor, 8. sclera, 9. choroid, 10. retina, 11. vitreous humor, and 12. optic nerve).
Conjunctiva
The conjunctiva is a thin, vascularized membrane that covers the sclera and lines the inside of the eyelids (Figure 1). The conjunctiva is divided into three main parts (bulbar, forniceal, and palpebral). In addition, the fourth part is the marginal conjunctiva. The conjunctival cell layer consists of stratified, non-keratinized epithelial cells [20]. Conjunctival cells are connected by desmosomes at the epithelial surface and linked by intercellular junctions, which disrupts drug transport in the deeper layer. Goblet cells are also found as apocrine cells, which are larger than epithelial cells [21].
Aqueous humor
The aqueous humor is watery fluid in the anterior chamber of the eye and via the pupillary aperture to the posterior chambers. The aqueous humor lies between the cornea and lens (Figure 1). The aqueous humor functions in nutrient transportation and maintains the intra-ocular pressure (IOP) throughout the eye [22]. The aqueous humor is produced by the ciliary body. The aqueous humor mainly consists of water and electrolytes, like sodium, potassium, various metabolites, glucose, and proteins [23, 24].
Lens
The lens is a vital component of the eye. The lens is a transparent and biconvex in structure posterior to the iris and pupil (Figure 1). The lens focuses light entering the eye, which is transmitted towards the retina. The lens is made up of tightly packed elongated cells containing crystalline protein. The primary function of the lens is to refract light rays. The lens acts as a filter protecting against translation of drugs from the aqueous humor into the vitreous humor [25–27].
Sclera
The sclera is a hydrated and white portion of the eye (Figure 1). The sclera consists of fibrous, thick connective tissue. The sclera also contains collagen fibers, which gives strength to the sclera. The sclera is divided into three parts (episcleral, stroma, and lamina fusca). The main function of the sclera is to provide a protective barrier to the inner parts of the eye and help maintain the proper shape of the eye [26].
Vitreous humor
There is a gel-like substance that fills the eyeball behind the lens. The vitreous humor is located posterior to the lens and anterior to the retina (Figure 1). It is mainly composed of water, collagen fibers, hyaluronic acid, and various proteins [27].
Retina
The retina is a multi-layered structure that includes the photoreceptors (rods and cones) and is necessary for vision. The retina converts the light into neural signals that the brain interprets as images. Cone and rod cells make up this structure. Cone cells are responsible for vision in bright light, while rod cells are used for vision in low light. The retina contains a photoreceptor layer, bipolar cells, ganglion cells, and pigment epithelium cells [28].
Choroid
The choroid is a vascular layer lying between the retina and sclera (Figure 1) that provides nutrients to the retina. The choroid is made up of blood vessels, connective tissues, and pigment cells (melanocytes). Melanin is present in high amounts, which helps absorb more light. The choroid contains three layers (outer, middle, and inner). The choroid supplies essential oxygen to the outer layer [29].
Ocular barriers
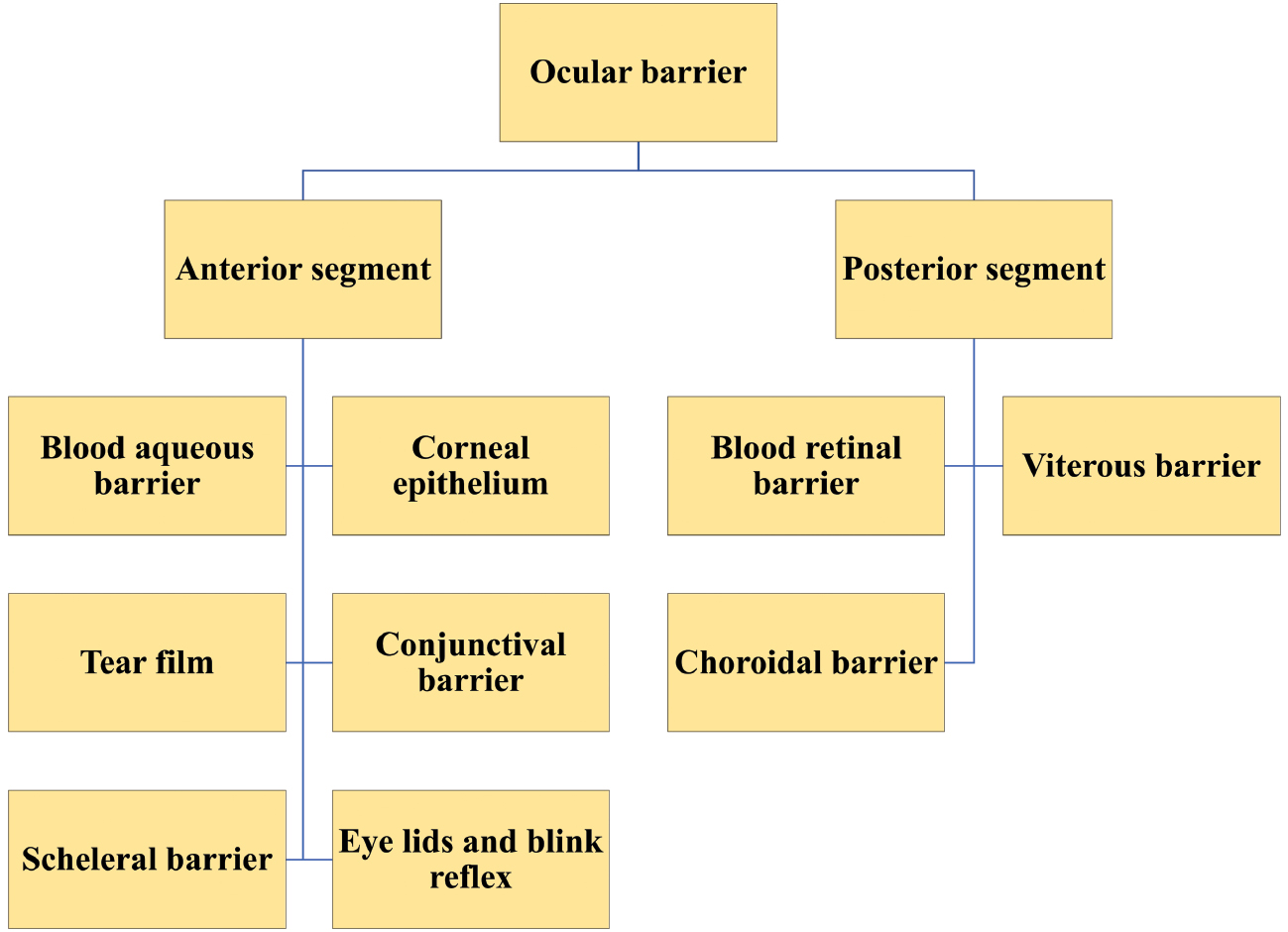
There are various types of barriers (Figure 2) present in the eye which protect the internal structures of the eye and does not allow foreign particles into the deep layers of the eye. These barriers are discussed below.
Figure 2 Classifications of barriers in ocular system (blood aqueous barrier, corneal epithelium barrier, tear film, conjunctival barrier, scleral barrier, blood retinal barrier, vitreous barrier, and choroidal barrier).
Corneal epithelial barrier
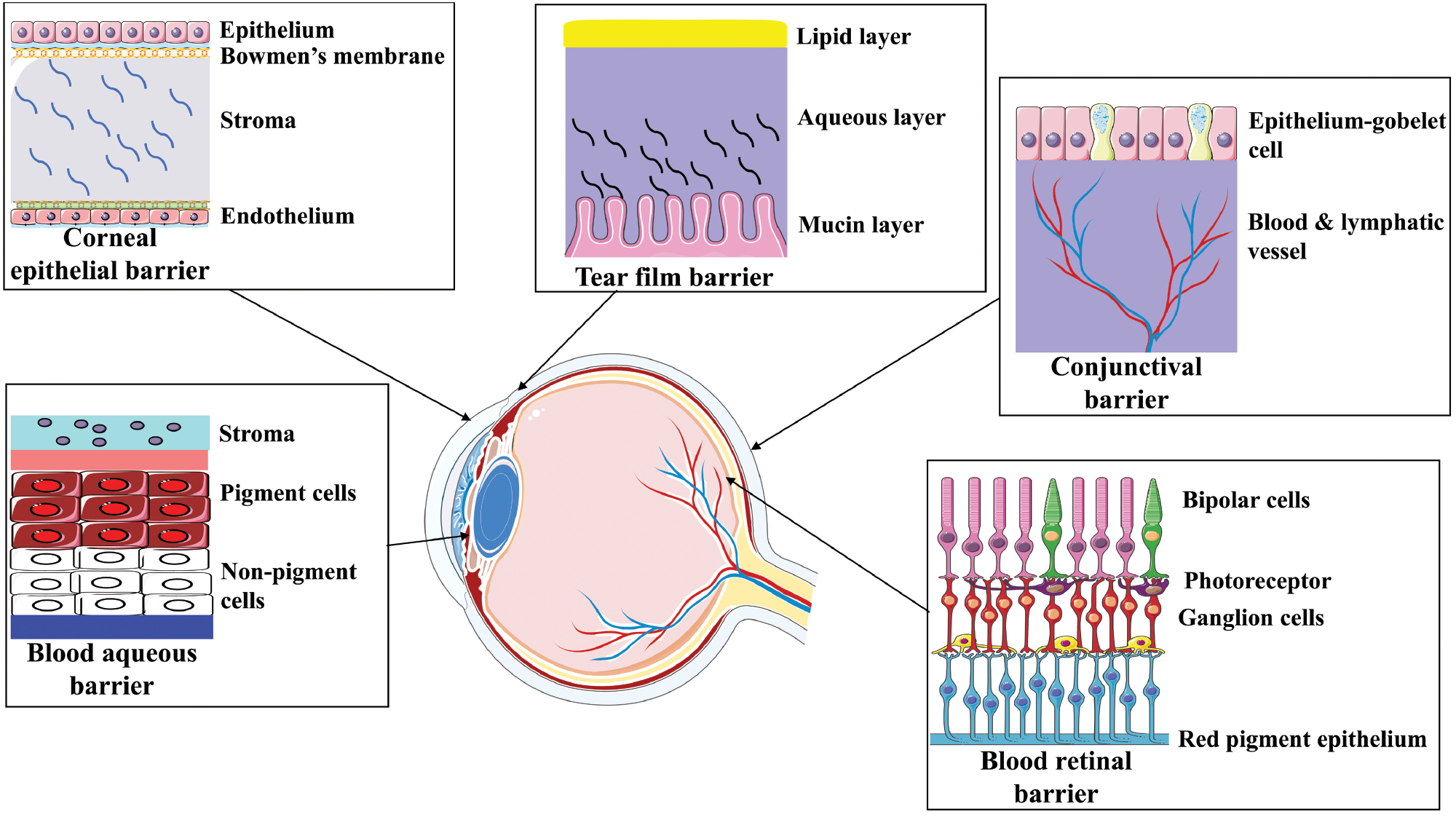
The corneal epithelial barrier is the outermost layer of the cornea. The corneal epithelial barrier acts as a primary barrier that prevents the entry of foreign particles and maintains a sterile environment in the anterior segment of the eye. The corneal epithelial barrier prevents approximately 90% of drugs with a molecular weight >500 Da from penetrating deep layers of the cornea. This barrier is composed of tight junctions formed by occludin and claudin at the epithelial surface, which shows high resistance against permeation of drugs. This barrier has a sandwich construction with three layers (epithelium-lipid, stroma-aqueous, and endothelium-lipid) [30, 31]. This construction also serves as an obstacle of hydrophilic drugs that cannot cross through the epithelium layer. Lipophilic drugs cannot cross the stroma layer. For example, fluorescein remains on the surface of the epithelium but penetrates the stroma layer. The epithelium layer is negatively charged, so nucleic acid, which has a negative charge, cannot cross easily [32, 33].
Conjunctival-scleral barrier
The conjunctival-scleral barrier is a non-corneal pathway that includes the sclera and conjunctiva (Figure 3). The conjunctiva is a mucous layer located on the outer part of the cornea in the posterior region. The conjuctiva is 17 times larger than the cornea and is therefore more suitable for drug absorption than the cornea. The conjunctival-scleral barrier consists of tight junctions (claudins, occludin, JAM-A, and tricellulin). This barrier admits compounds with molecular weights of 20–40 kDa. A drug can be eliminated by rapid vascular drainage after administration by this route [34, 35]. After clearance of the drug from the conjunctiva, A drug crossed the sclera to reach the anterior segment via the trans-scleral route after administration by this route [36]. The conjunctival-scleral barrier has a greater surface area and a comparatively high permeability compared to the cornea. The size of the drug molecule has a greater impact on the capacity to penetrate the sclera than lipophilicity [37].
Figure 3 Schematic representation of ocular barriers; specifically, anatomic and physiologic structures in drug penetration in anterior and posterior segments of the eye (corneal barrier, tear epithelium barrier, blood aqueous barrier, blood retinal barrier, and conjunctival barrier).
Blood-aqueous barrier (BAB)
The BAB is a combination of a non-pigmented ciliary body and the iris endothelium (Figure 3). The BAB serves as a barrier that prevent solutes from entering the intraocular space [38]. The ciliary body, which is present from the iris root-to- the retina, forms a ring around the globe. The ciliary body has two major components (pars plicata and pars plana). The pars plicata is present in the anterior part and the pars plana is located between the retina and pars plicata. Due to the fenestrated and leaky nature of choroidal capillaries, the ciliary body is highly vascularized [39]. The physicochemical characteristics of the drug molecules influence osmotic pressure, which allows medications to pass through the BAB. Smaller, lipophilic medications can pass through the BAB faster than larger, hydrophilic medications. For example, pilocarpine is eliminated more rapidly than inulin [31]. Ocular drug delivery remains challenging due to the specialized tissue barriers that can provide an impact of therapeutic effectiveness. The BAB mainly consists of non-pigmented epithelium, the ciliary body, and the capillary endothelium. The protein concentration is low in the aqueous humor (AH) with only a small portion of plasma protein [40]. Plasma proteins that pass through the capillaries of the ciliary body are unable to enter the posterior chamber because plasma proteins are blocked by the non-pigmented epithelium of the ciliary body. Similarly, these proteins cannot access the anterior chamber due to the tight junctions present in the iris capillary endothelium [32]. Non-pigmented epithelium cells act as physical barrier more than pigmented cells because tight junctions are present between the cells [39].
Blood-retina barrier (BRB)
Consequently, the BRB is the most important barrier in the back of the eye. The outer BRB is composed of tight junctions of retinal pigment epithelial cells, while the inner BRB is produced by tight junctions of endothelial cells and retinal capillaries (Figure 3) [36]. Muller cells, astrocytes, and pericytes cells, which are present in the retinal barrier, have a critical role in maintenance of the retinal barrier and regulation of nutrient uptake by cells in the BRB [41]. The BRB is formed when retinal glia and pericytes interact with the endothelium. The BRB regulates the flow of metabolites and waste products between the vascular lumen and the neural retina. Pericytes secrets angiopoietin 1 and induce tight junctions to support endothelial cells [42]. Water, plasma components, and other dangerous substances cannot get through this barrier and penetrate the retina. In contrast, the BRB can also stop medication molecules to enter the intraocular space. Thus, preservation of the eye as a favored location for typical visual function depends on the BRB. Adult human retinal pigment epithelium (RPE) has tight connections (approximately 40 Ω•cm2), making the RPE a low-resistance epithelium [34].
Eyelids and tear film
The eyelids act as a physical barrier which prevent bacterial agents, foreign bodies, and other external particles from entering the eye (Figure 3). The reflex blink has a significant role in elimination of applied eye drops in the outermost layer of the eye epithelium [43]. The optimum pH for eye formulations should be 6.5–7.8. Another range of eye formulations may cause immediate discomfort. Because of the physicochemical characteristics of the outermost layer of the eye epithelium and the fact that the outermost layer of the eye epithelium contains proteins and enzymes that are antibacterial and anti-inflammatory, the tear film acts as a barrier [44]. The outermost layer of the eye epithelium has three separate layers (the inner mucin layer, which is released by the mucous glands and conjunctival glandular cells, the middle aqueous layer, which is secreted by the lacrimal glands, and the outer lipid layer, which is created by the meibomian glands). The lipid layer helps reduce tear evaporation, thereby maintaining the osmolarity [33, 34].
Challenges of ocular drug delivery systems
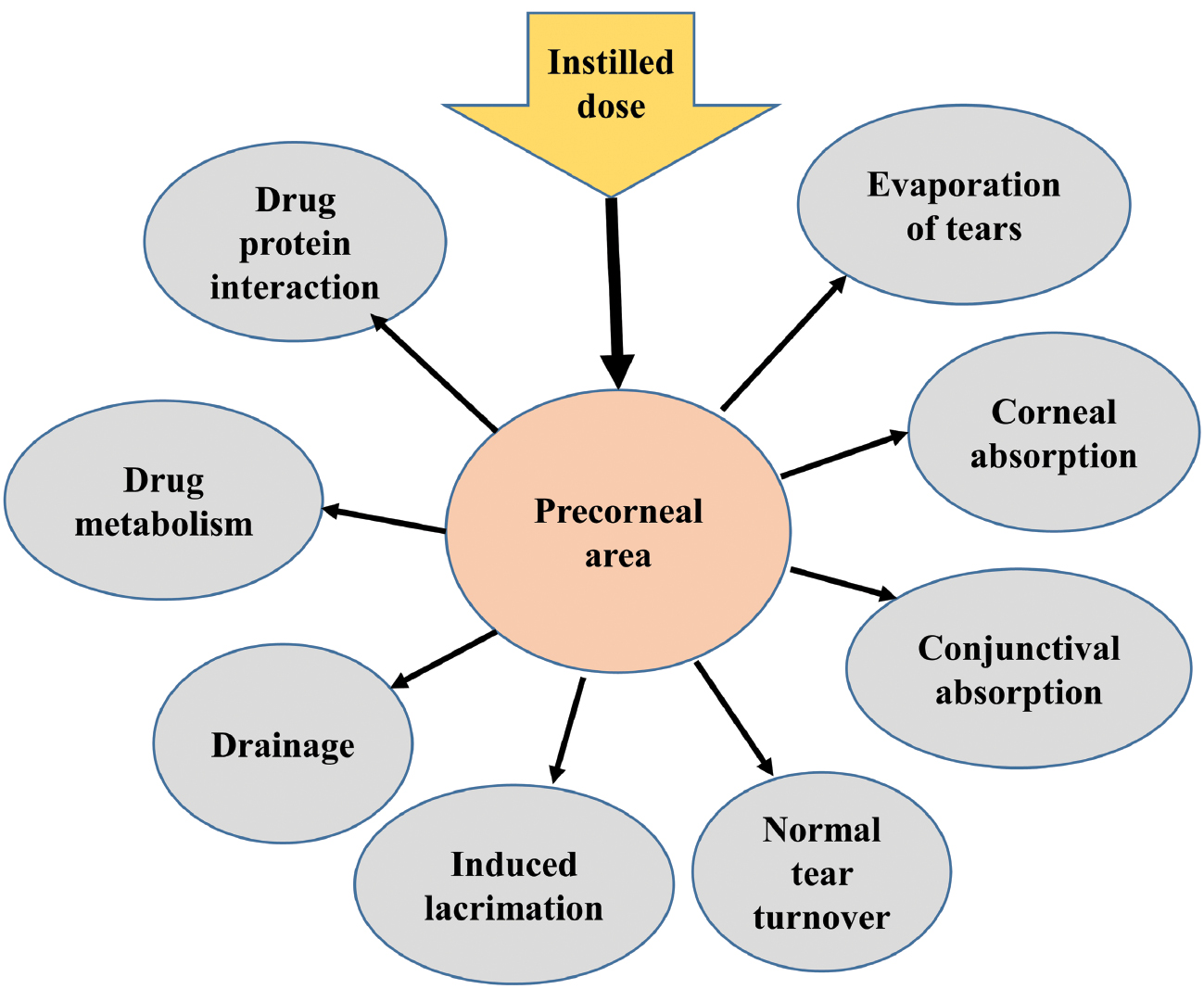
The major challenges in ocular delivery systems are delivery in the anterior part and another delivery in the posterior part of the ocular cavity [12]. After application of drug in the anterior segment of eye the drug must first pass through the tear film and conjunctiva, which are the first barriers in the pathway and slow the rate of penetration of the active component in the eye. Poor drug bioavailability in most ocular formulations is caused by pre-corneal loss of factors (Figure 4). [45]. The BRB prevents ocular medications administered topically in the posterior segment of the eye. The BRB is permeable to more lipophilic molecules, so only these lipophilic drugs can enter the posterior portion of the eye. The repeated use of highly concentrated medication solutions may result in harmful side effects and ocular surface cellular damage [45].
Figure 4 Precorneal factors influencing loss of optically applied dosage forms.
Route of administration in the eye
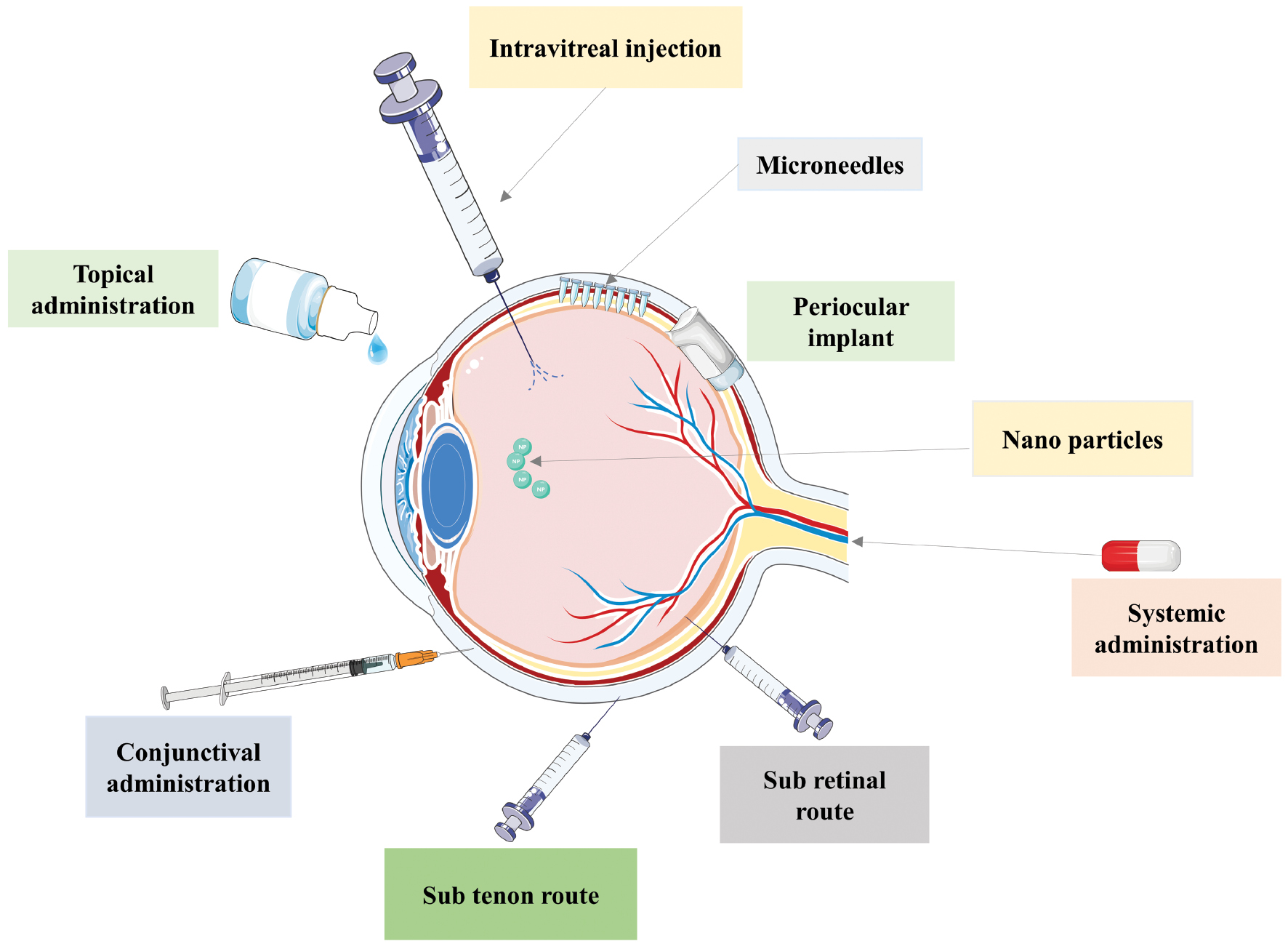
There are different administration routes (Figure 5) available for ophthalmic drug delivery systems. Drugs can be administered by any of the below routes.
Figure 5 Schematic illustration of ocular administration routes in the anterior and posterior segments of the eye (topical administration, conjunctival administration, sub tenon, sub-retinal administration, systemic administration, periocular implant, nano particles, and microneedles).
Topical administration
Topical drug administration is the most frequently used route of administration. Eye drops, ointments, and pastes are mainly used in this approach because the preparations can be easily administered to the patient [46].
Systemic administration
Systemic administration is one of the suitable administration routes that allows drug delivery to the posterior segment of the eye but also faces significant challenges due to the presence of the BRB and BAB, which blocks the penetration of drug molecules. As a result, a high dose is required to achieve the target therapeutic effects [47, 48].
Intravitreal administration
Ocular drugs are directly injected into the vitreous humor using a 30 G needle in this approach, which enhances drug absorption compared to topical or systemic methods. While intravitreal administration achieves high drug levels in the retina, intravitreal administration also presents several technical challenges, such as intravitreal hemorrhage, endophthalmitis, and injury to the lens [48].
Periocular implants
Periocular implants are usually placed on the surface of the eye in areas, like the conjunctiva, retrobulba, and peribulba spaces. These implants deliver medications directly to the vitreous, retina, and choroid via the trans-scleral route [23]. These routes largely provide a good way to treat retinal disorders. The challenges associated with these routes are the barriers, such as the RPE, choroid, and sclera, and blood and lymph in the surrounding tissues [49].
Subconjunctival
The subconjunctival injection route is commonly used for delivering drugs to the anterior part of the eye to achieve higher drug concentrations compared to topical and other applications. The most freqentu use of this method is to treat retinal disorders. Blood flow and tear production can lead to decreased bioavailability, limiting the effectiveness of the treatment [50].
Suprachoroidal
This route involves drug delivery using microneedles into the supracervical space. The applied pressure helps spread the formulation throughout the suprachoroidal space during the injection. This approach has been studied to deliver drugs into the eye via surgical techniques using microneedles. The suprachoroidal approach provides long-term treatment by targeting the retina and choroid directly at the injection site. There are several challenges present in the suprachoroidal route, such as the risk of choroidal detachment and suprachoroidal haemorrhage. These challenges have made it difficult to implement the suprachoroidal approach in practice [50].
Sub-tenon
This route involves drug delivery using an injection technique that delivers medication into the space between the tenon capsule, a protective membrane, and the sclera (the white of the eye). This method is generally considered to be safer than intravitreal injections because microneedles are not used. The subtenon route remains an important option for uveitis specialists, especially in cases in which intravitreal administration may not be feasible or requires special consideration. Like other intra- or peri-ocular steroid injections, subtenon or subconjunctival delivery can still lead to cataract progression and ocular hypertension [49, 50].
Strategies to overcome eye barriers
To overcome barriers in ocular drug delivery systems is difficult due to the unique challenges present in the eye, like various barriers. Below are some strategies to overcome eye barriers.
Enhancement formulations with carriers
- Nano-carriers: Nanoparticles are used in formulations to improve drug solubility, stability, and bioavailability due to the small size of the drug. Nano-carriers, like liposomes, niosomes, and phytosomes, provide protection to the drugs from environmental and biological factors [11, 51].
- Polymeric micelles: Polymeric micelles are tiny, specialized carriers that facilitate drug absorption and remain active in the specific site for a longer time. This feature means patients can benefit from more effective treatments with several doses [4].
- Hydrogels: Hydrogels provide sustained release and improve contact time and prolong action at the ocular surface [52].
Improving bioavailability
- Permeation enhancers: Permeation enhancers are added to achieve easier penetration in the deeper layer of the eye so the drug can work better and faster [53].
- Liposomes: Liposomal medications are mainly used to enhance drug bioavailability. These liposomal medications are mainly tiny bubbles which keep the drug at a specific site to provide full therapeutic action of the active pharmaceutical ingredient (API) [54].
Targeted delivery systems
- Prodrugs: Prodrugs are inactive in nature but when administrated, bind to the specific site and produce therapeutic actions. The proper design of a prodrug is necessary in targeted delivery.
- Tissue-specific ligands: Ligands that target specific receptors and bind to ocular tissues are used for more effective therapeutic action locally [55].
Innovative delivery methods
- Intraocular implants: Sustained-release implants release drug slowly that provide long-term drug delivery directly to the site of action.
- Microneedle arrays: Microneedle technology delivers medications that produce minimal discomfort. These tiny needles gently pierce the outer layer of the eye and inject the medicine [5].
Prolong retention time
- Viscosity modifiers: Viscosity-enhancing agents are added to increase the retention time of eye drops on the ocular surface [11].
- Mucoadhesive agents: Mucoadhesive polymers are used that prolong the contact time of the drug with the eye [53].
Controlled release mechanisms
- Biodegradable polymers: Biodegradable drug delivery systems have been developed using biodegradable polymers that release the drug at controlled rates over time.
- Stimuli-responsive systems: Stimuli-responsive systems are devices that can release medications in reaction to stimuli, such as temperature or pH. These are intelligent drug delivery devices [56].
Patient compliance strategies
- User-friendly formulations: Formulations have been prepared that patients can use, such as gels or ointments, that require less frequent application.
- Education and training: Education and training are provided to patients regarding the importance of adherence and correct administration techniques of the ocular dosage form, such as pastes, ointments, and eye drops [53].
Regulatory and research support
- Collaboration with regulatory bodies: Patient treatment is developed and more safety is achieved by complying with the regulatory authorities.
Clinical trials and feedback
- Clinical trials: Clinical trials are conducted focusing on user experience to collect data on ease of use, effectiveness, and patient preferences.
- Feedback mechanism: Channels for patient feedback are established to recorrect and improve drug delivery systems after trials [57].
By using these strategies, researchers and developers can enhance the effectiveness of ocular drug delivery systems and improve patient outcomes.
Recent developments in ocular drug delivery systems
Recent developments in ocular drug delivery systems have focused on improved efficacy and patient compliance. Some notable advancements include ocular inserts, nanoparticle hydrogels, smart polymers, microneedle patches, contact lenses, implantable devices, and ocular injections. Below is a detailed overview of ocular inserts, contact lenses, and microneedles in this section of the review.
Ocular inserts
In the 19th century squares of dry filter paper impregnated with dry solutions, such as atropine sulphate or pilocarpine hydrochloride, were used as the first solid medication (the forerunners of today’s insoluble inserts) [58].
Merits of ocular inserts
- Ocular inserts offer sustained and controlled release of medications to the site of action, e.g., ketorolac ocular inserts with a microsphere carrier platform (Table 1).
- Drug bioavailability is increased by increasing the corneal residency period.
- The therapeutic performance of a drug can be improved to provide comfort and better patient compliance.
- Ocular inserts have a longer shelf life compared to aqueous solutions.
- Protective barriers, like drainage, lacrimation, and conjunctival absorption, are avoided [58, 59].
Table 1 Summary of Recent Experimental Studies on Ocular Inserts
| Sl. No. | Model Drug | Dosage Form | Carrier Platform/Type Of Insert | Result | References |
|---|---|---|---|---|---|
| 1. | Triamcinolone acetonide | Ocular insert | Nanofiber carrier | Decrease particle size, systemic absorption, and side effects. | [11] |
| 2. | Ketorolac | Ocular insert | Microsphere | Prolonged drug release | [11] |
| 3. | Tenoxicam | Ocular insert | Nanostructured formulation | Superior drug diffusion, ex vivo and in vivo permeation | [11] |
| 4. | Pilocarpine | Ocular insert | Niosome, hydrogel | Enhanced bioavailability and extended release | [112, 113] |
| 5. | Timolol maleate | Ocular insert | Ocular films | Improved ocular retention and reduced frequency of dosing | [114] |
| 6. | Dexamethasone | Ocular insert | Intra-canicular insert | Controlled release with reduced side effects | [115] |
| 7. | Fluorescein acetanide | Ocular insert | Intravitreal Insert | Enhanced visibility and extended diagnostic effectiveness | [116] |
| 8. | Diclofenac sodium | Ocular insert | Nanoparticle system | Controlled anti-inflammatory effect and reduced systemic absorption | [117] |
| 9. | Loteprednol etabonate | Ocular insert | Microsphere formulation | Prolonged therapeutic action with lower incidence of side effects | [118] |
| 10. | Chloramphenicol | Ocular insert | Hydrogel | Broad-spectrum antibiotic used in eye infections | [119] |
| 11. | Ciprofloxacin | Ocular insert | Polymeric film | Increased stability and prolonged antibacterial effect | [120] |
| 12. | Brimonidine | Ocular insert | Polymeric film | Controlled release | [121] |
| 13. | Valacyclovir | Ocular insert | Lipid-based system | Enhanced corneal penetration and prolonged antiviral activity | [122] |
| 14. | Prednisolone | Ocular insert | Thermo-sensitive gel | Sustained release with reduced intraocular pressure | [123] |
| 15. | Ketorolac tromethamine | Ocular insert | In situ gelling insert | Prolonged anti-inflammatory effects with minimized side effects | [124, 125] |
| 16. | Moxifloxacin | Ocular insert | Liposome | Increased ocular bioavailability and reduced dosing frequency | [125, 126] |
| 17. | Acyclovir | Ocular insert | Polymeric film | Controlled drug delivery | [127] |
| 18. | Brinzolamide | Ocular insert | Hydrogel | Improved solubility and sustained carbonic anhydrase inhibition | [128] |
| 19. | Bimatoprost | Ocular insert | Polymeric film | Enhanced bioavailability and prolonged intraocular pressure (IOP) lowering effects | [129] |
| 20. | Timolol maleate | Ocular insert | Nano-emulsion | Improved penetration and sustained release | [130] |
| 21. | Cyclosporine A | Ocular insert | Nano-micelle polymeric insert | Controlled release with reduced immune response | [131] |
| 22. | Amino acid-based peptides | Ocular insert | Biodegradable film | Targeted delivery for retinal diseases | [132] |
| 23. | Indomethacin | Ocular insert | PVA insert | Prolonged antibacterial effect with reduced toxicity | [133] |
| 24. | Dorzolamide | Ocular insert | Chitosen hydroxyl ethyl cellulose insert | Sustained release of drugs for glaucoma treatment | [134] |
| 25. | Pilocarpine nitrate | Ocular insert | Hydrating gel | Prolonged tear film stability and ocular comfort | [135] |
| 26. | Azithromycin | Ocular insert | Nanoparticles | Enhanced penetration and sustained antibacterial activity | [136] |
| 27. | Norfloxacin | Ocular insert | Polymeric film | Controlled release for bacterial infections with minimal side effects | [137] |
| 28. | Betaxolol | Ocular insert | Microsphere formulation | Prolonged effect on corneal healing and repair | [138] |
| 29. | Epinephrine | Ocular insert | Biodegradable polymer | Sustained effect for glaucoma management | [139] |
| 30. | Gentamicin | Ocular insert | Nanoparticle delivery | Increased stability and prolonged antibacterial effect | [140] |
| 31. | Levobunolol | Ocular insert | Thermo-sensitive gel | Reduced side effects with controlled release | [141] |
Limitations of ocular inserts
- Ocular inserts may undergo sporadic and unintentional loss during sleeping or while massaging the eyes. In addition, visual disturbances and difficulty with proper ocular implant placement further limit patient acceptability.
- One major drawback of ocular inserts is the solid structure, which causes the patient to sense the insert as a foreign object in the eye.
- Once inserted, the release rate is often fixed, which may not be ideal for all patients, especially if dose adjustment is needed [59].
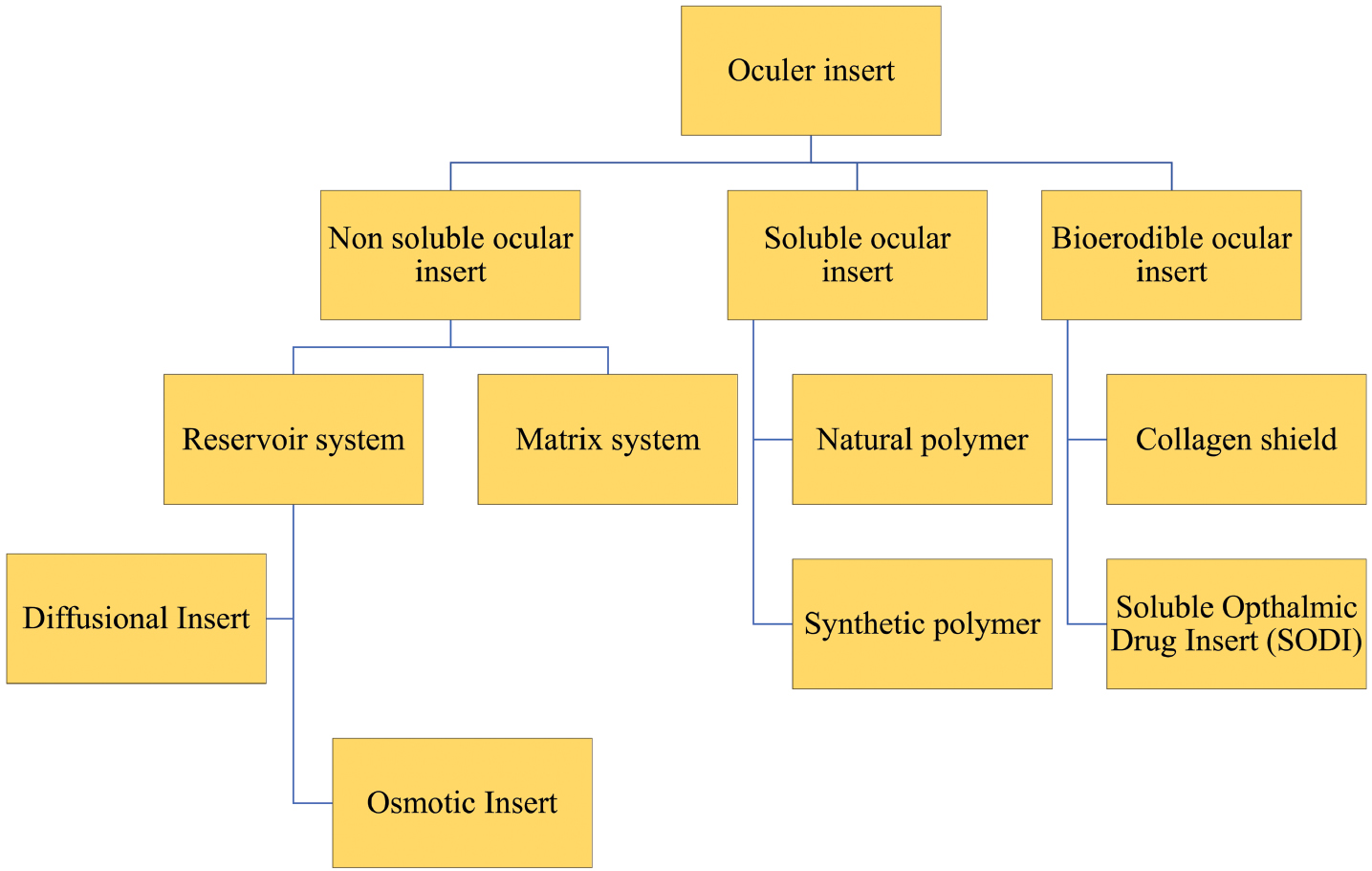
Classification
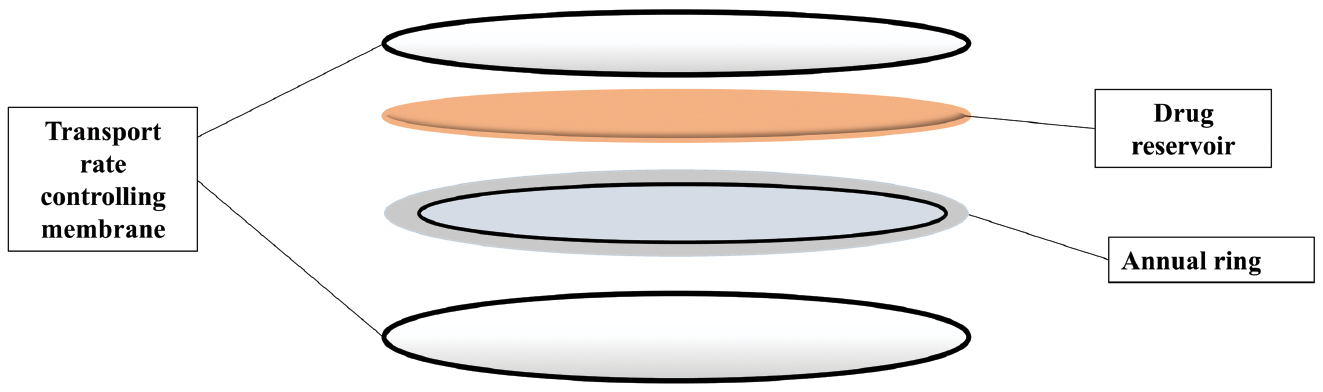
It can be classified as: Ocular insert drug release mechanisms can be classified into diffusion, osmosis, and bioerosion (Figure 6).
Figure 6 Structural representation of ocular inserts with drug reservoir, annual ring, and transparent rate controlling membrane.
Ocular insert drug release mechanism
- Diffusion: The drug is released externally through the membrane at a controlled rate (Figure 7). It has been shown that when a drug is dispersed within a solid, non-erodible body consisting of pores, the drug is released through pores by diffusion. The solid dispersed medication is distributed to dissolve gradually into the matrix; this slow immersion of the aqueous solution provides controlled drug release [58]. True dissolution in these soluble devices mostly occurs by the swelling of the polymer. The active substance in these swelling-controlled devices is evenly distributed throughout a glassy polymer. Because glassy polymer proteins are densely cross-linked, there is little or no diffusion in the dry matrix of the polymer. After the insert containing the drug is placed in the eye, water from tear fluid will be able to swell and ultimately relax the polymer chains, allowing for drug diffusion. The rates of matrix dissolution and matrix swelling are influenced by the chemical structure of the polymer. Linear amorphous polymers dissolve faster compared to cross-linked or partially crystalline polymers [59].
- Osmosis: The ocular insert is comprised of an elastic membrane that is embedded into the structure and acts as a barrier between two compartments (Figure 7). The first compartment is a liquid containing a solute, which is unable to permeate through the semi-permeable membrane. The second compartment is a gel or liquid drug containing-compartment, where the elastic membrane only surrounds the second partition. An ethanol port exists within the impermeable structure of the insert. The insert structure is such that when it submerged in water, one side of fills with water, which causes pressure to build up. This pressure enables the drugs to come out from one port. The introduction of water into the first chamber allows the elastic foil to be stretched. With the introduction of pressure in the second chamber, some ethanol is forced into the polymer matrix, which enables the embedded drug to diffuse out [59, 60].
- Bioerosion: The drug is contained within the polymer matrix that holds shape. When dried, the shape is fixed, which allows the drug to be dispersed throughout the surface of the structure. The drug-filled matrix containing insert enables drug polymers to slowly dissolve and release throughout the drug coated with polymer. When tear fluid come in contact during drug release, the matrix begins to weaken at a slow rate, which prevents burst effects. The drug release mechanism of erodible (E-type) devices relies on chemical or enzymatic hydrolytic reactions that cause the polymer to dissolve or break down into smaller, water-soluble molecules. If the medication has low water solubility and the devices retain a constant surface geometry, these polymers increase hydrophilicity and the drug is released by zero-order release kinetics [61, 62].
Figure 7 Types of ocular inserts (non-soluble inserts: diffusion system, osmotic system, and hydrophilic contact lens; soluble inserts: natural and synthetic polymers; bio-erodible inserts: non-erodible and erodible).
Recent advances in ocular inserts
- Hydrogel-based ocular insert systems for hydrophobic drugs: Hydrophobic drug delivery to the eye has been improved by systems that are hydrogel-based, which increases the solubility of hydrophobic drugs. Hydrogels overcome several anatomic and physiologic barriers, which provide effective absorption of drugs and make the therapy long-lasting. For example, the pilocarpine hydrogel-based ocular insert increases bioavailability by enhancing residence time (Table 1) [4].
- Nanofiber-based ocular insert: A nanofiber-based ocular insert has been developed with electrospinning technology. A nanofiber-based ocular insert increases the drug contact time, control, and extended release of the drug. For example, triamcinolone acetonide-containing ocular insert reduces systemic absorption and side effects (Table 1) [63].
- Ocular delivery of CRISPR/Cas genome editing components: The genome editing method CRISPR/Cas components can be targeted directly to the eye to treat disease in short time. This new approach has the potential to treat not only inherited but also multifactorial eye disorders [64].
- Biodegradable and non-biodegradable ocular inserts: Researchers have developed contact lenses that are mucoadhesive, which can release the drug mixture (moxifloxacin and dexamethasone). These contact lenses improve the bioavailability and ensure sustained drug release for the cure of ocular infections [65, 66].
- Development of magnetically actuated glaucoma drainage devices: There is a novel glaucoma drainage implant that employs magnetic actuation in the postoperative regulation of intraocular pressure. This minimally invasive device leads to personalizing treatments and better postoperative results, such as the BIM ring® (Table 2) [67].
Table 2 Overview of Marketed Ocular Insert-Based Drug Delivery Products
| Country | Ocular Insert | Manufacturing Company | Purpose | Approved Indications | Technology Platforms | Reference |
|---|---|---|---|---|---|---|
| USA | Ocusert® | Alza Corporation | Developed for delivering pilocarpine to treat glaucoma | Reduction of intraocular pressure in glaucoma patients | Diffusion-controlled membrane system | [142] |
| USA | Dextenza® OTX-CSI |
Ocular Therapeutix, USA | Post-surgical ocular inflammation and pain | Pain and inflammation following ophthalmic surgery | Hydrogel-based intra-canalicular insert releasing dexamethasone | [58] |
| Lacrisert® | Bausch and Lomb, USA | Treatment of dry eye syndrome | Moderate-to-severe dry eye, kerato conjunctivitis | Hydroxypropyl cellulose-based slow-dissolving insert | [11] | |
| Russia | BIM ring® | LLC NCK-Progress, Russia | Glaucoma | Reduction of intraocular pressure | Drug-eluting ring insert | [106] |
| France | Mydriasert® | Laboratories Théa, France | Diagnosis (pupil dilator) | Mydriasis for diagnostic and pre-surgical use | Reservoir insert releasing tropicamide & phenylephrine | [106] |
| Spain | Mydriasert® | Laboratories Théa, France | Diagnosis (pupil dilator) | Mydriasis for diagnostic and pre-surgical use | Reservoir insert releasing tropicamide & phenylephrine | [106] |
| Sweden | Mydriasert® | Laboratoires Théa, France | Diagnosis (pupil dilator) | Mydriasis for diagnostic and pre-surgical use | Reservoir insert releasing tropicamide & phenylephrine | [106] |
| Finland | Mydriasert® | Laboratoires Théa, France | Diagnosis (pupil dilator) | Mydriasis for diagnostic and pre-surgical use | Reservoir insert releasing tropicamide & phenylephrine | [106] |
| Canada | Dextenza® | Ocular Therapeutix, USA | Post-surgical ocular inflammation and pain | Pain and inflammation following ophthalmic surgery | Hydrogel-based intra-canalicular insert releasing dexamethasone | [143] |
Patent information of the ocular insert
The development of ocular inserts has focused on numerous patents (Table 3). Patented technologies often address challenges, like controlled drug release, extended retention time in the eye, and compatibility with sensitive ocular tissues. Innovations include biodegradable polymers, osmotic systems, and sustained-release mechanisms.
Table 3 Summary of Patents Related to Ocular Insert Technologies [144]
| Sl.No. | Patent Number | Title | Patent Information |
|---|---|---|---|
| 1. | Wo2024180472a1 | Ocular insert | Dissolvable ocular insert that releases lubricants and drugs into the eye for extended time |
| 2. | Wo2024180453a1 | Dissolvable polymeric eye inserts with a non-ionic cellulose derivative | When inserted into eye may absorb tears and dissolve and slowly release lubricants into tear film |
| 3. | Us20240207174a1 | Dissolvable polymeric eye inserts | Eye insert release humectants and drugs into the eye |
| 4. | Us 10,835,416 b2 | Ocular insert apparatus and methods | Comprised of a retention structure sized for placement under the eyelids and along at least a portion of the conjunctival sac |
| 5. | Us 10, 042, 183 b2 | Ophthalmic device molds formed from water-soluble vinyl alcohol copolymer, ophthalmic devices molded therein, and related methods | Ophthalmic device molds made from at least one water-soluble vinyl alcohol copolymer; ophthalmic devices, such as ocular inserts |
| 6. | Us 9, 849, 085 b2 | Devices for sustained release medication delivery, applications, and production techniques | The technique involves carefully giving a mammalian creature in need of such therapy; a sustained release medication delivery device |
| 7. | Wo2017137934a1 | Non-invasive ocular drug delivery insert technology | This ocular insert allows releasing of at least one drug under suitable concentration levels during suitable periods of time |
Contact lens
Contact lenses are devices made up of hard or soft polymers that are designed to fit in cornea and correct refractive problems. Either hydrophilic or hydrophobic or both polymers are used to make contact lenses [68]. Hydrogel contact lenses are better at absorbing aqueous solutions, so contact lenses appear to be an effective way to deliver medications to the eye [69]. Contact lenses are present so close to the cornea that contact lenses have higher drug bioavailability than other non-invasive ophthalmic treatments, like eye drops or ointments. In addition, contact lenses offer a notable dose advantage over topical eye drops [62]. Drug-loaded contact lenses are recently a novel way to improve corneal permeability and ophthalmic drug bioavailability [70].
By using contact lenses as drug delivery platforms the efficacy of a drug has been improved when compared to boosting ocular bioavailability alone; patient adherence and prolonged drug release time is improved to conventional dosage forms. Conventional dosage forms deliver only 1%–5% of the drug to the targeted tissues where contact lens increases bioavailability up to 35%–50% with reduced systemic side effects [71]. For example, dexamethasone-containing contact lenses deliver 200 times more drug to the eye than conventional drops. Drug-loaded contact lenses provide high patient compliance compared to topical drops. Up to 29% of glaucoma patients struggle to self-administer drops properly in which drug-eluting contact lenses remove the dose instillation process and reduce dose frequency [72] eg., MediPrintTM contact lens is used to treat glaucoma (Table 4). Traditional soaking methods release most of the drugs within 1–3 h. To overcome this limitation, various advanced techniques, like molecular imprinting, drug-loaded nanocarriers, and vitamin E diffusion barriers have been developed that release drug over hours or even weeks in a controlled manner. We suggest that drug delivery using contact lenses enhances efficacy compared to the drug alone [73].
Table 4 Overview of Marketed Contact Lens based Drug Delivery Products
| Sl. No. | Product Name | Company | Application | References |
|---|---|---|---|---|
| 1. | Acuvue Theravision with Ketotifen | Johnson & Johnson Vision | Drug-eluting contact lens for delivering antihistamines to treat allergic eye conditions | [145] |
| 2. | MediPrint™ | Leo lens pharma | Treatment of prostaglandin and glaucoma | [146] |
| 3. | OcuMedic Therapeutic Lenses | OcuMedic, Inc. | Contact lenses designed for post-surgical recovery and drug delivery to the ocular surface | [147] |
| 4. | Medidur™ | pSivida Corp | Used to treat posterior uveitis | [148] |
Merits of contact lenses
- Contact lenses provide a controlled and sustained release of drug to the site of action. Contact lenses enhance therapeutic efficacy compared to conventional eye drops, which have low bioavailability due to continuous tear drainage [73].
- Contact lenses ensure better drug absorption to the cornea and reduces drug wastage [74].
- Contact lenses provide better patient compliance.
- The main advantage of contact lenses include correcting vision and delivery of drug at the same time.
- Contact lenses provides protection to the ocular surface [75].
- Contact lenses minimize the systemic absorption and reduces the risk of side effects [76].
Limitations of contact lenses
- Contact lenses have limited drug loading capacity. The quantity of drug that may be delivered through a contact lens is often limited, which limits utility for more serious conditions [77].
- Extended wear or the elution of some drugs from contact lenses may induce irritation or adverse responses in sensitive patients [78].
- The drug-loaded contact lenses are more expensive and require sophisticated manufacturing techniques, making drug-loaded contact lenses less accessible [79].
- Some drugs may interact with the lens material, which may lead to suboptimal release or degradation [80].
- Storage and use of drug-loaded lenses can be complicated as sterility and stability have to be ensured [81].
Mechanism of drug release
Release of drug from contact lenses mostly involves physical and chemical phenomena, which is often associated with the characteristics of lens materials, drug characteristics, and the surrounding environment. The mechanisms involved are detailed below.
- Diffusion
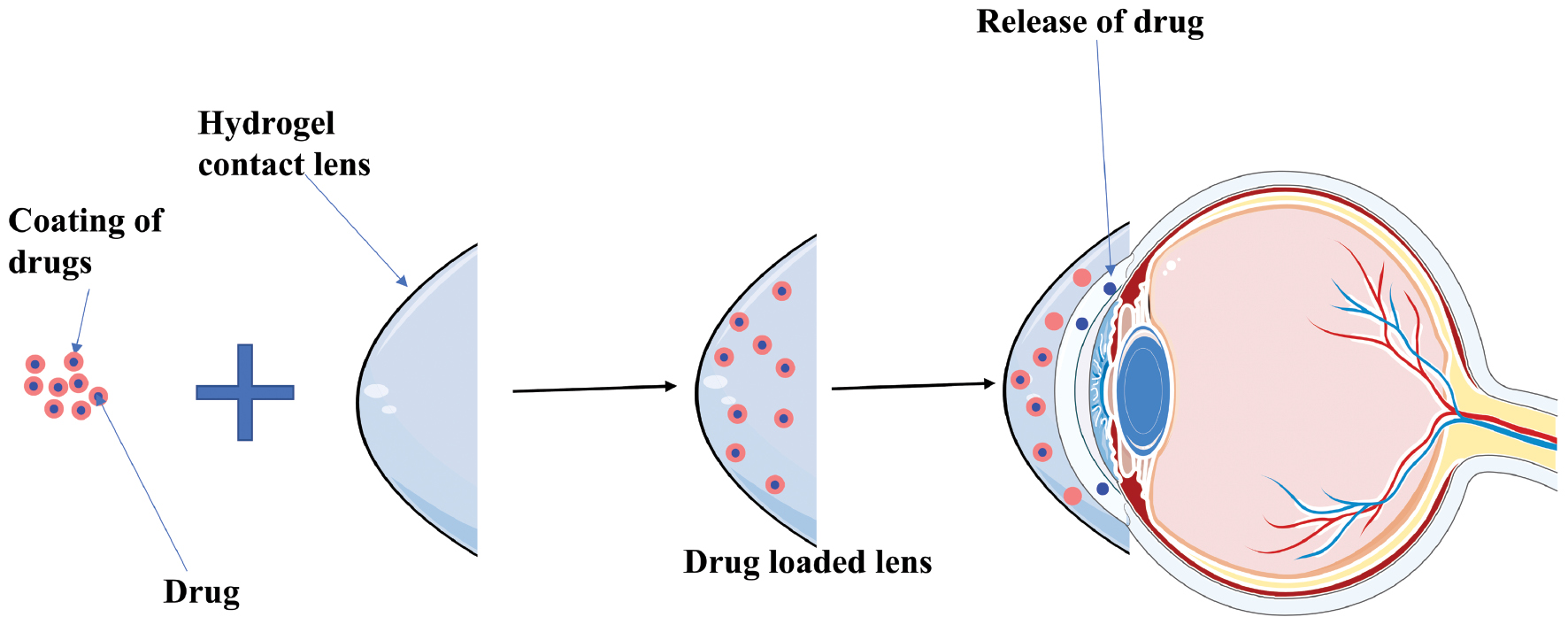
Drugs are incorporated into the contact lens matrix during manufacturing. When the contact lens comes into contact with tear fluid, the drug diffuses out of the lens material into the tear film and onto the eye (Figure 8). The diffusion rate depends on the porosity of the lens material, hydrophilicity, and the size of the drug molecule.
For example, hydrogels allow the drug to diffuse out as the hydrogels swell in the aqueous tear environment [82]. - Swelling-controlled release
Contact lenses, especially hydrogels, absorb water from the tear film and swell. Swelling increases pore size that lets the drug out. This mechanism is especially relevant for hydrophilic drugs [83]. - Erosion-controlled release
Drugs are released as the polymer matrix progressively erodes in biodegradable lenses.
This process is less common for contact lenses but is being explored for advanced drug delivery systems [84]. - Ion-exchange mechanism
Lenses are made of ionically charged polymers that attract oppositely charged drugs. The drug is released through ion exchange with the tear fluid.
For example, cationic drugs bound to negatively charged hydrogel lenses are displaced by positively charged ions in tears, thus releasing the cationic drugs.
Figure 8 Structural representation of drug-loaded contact lenses and mechanism of action of drug release from the lens-to-the cornea.
Recent advances in contact lenses
Contact lenses have come a long way since being invented, starting from simple vision correction devices to sophisticated devices that could revolutionize eye care. Some of the recent advances in contact lenses are described below [85].
- Silicone hydrogel lenses: Silicone hydrogel lenses are advanced compared to traditional hydrogels because silicone hydrogel lenses allow better oxygen permeability. Therefore, more oxygen will come to the cornea and decreased probability of hypoxia complications and increased comfort of wearing [86]. Modern silicone hydrogel contact lenses have a surface treatment or contain hydrophilic materials that improve wettability to minimize dryness and discomfort. For example, resveratrol contact lens provide antioxidant and anti-inflammatory effects (Table 5) [87].
- Multifocal and presbyopia-correcting lenses: Multifocal and presbyopia-correcting lenses address the age-related decline in near vision. The wearer will be able to see clearly at both near and far distances with multifocal and presbyopia-correcting lenses. Recent developments in lens design involves materials that have been associated with better visual acuity and fewer visual disturbances compared to multifocal lenses [88].
- Smart contact lenses: Smart contact lenses are under development. Such lenses are equipped with in-built sensors and technologies to assist in monitoring health parameters and deliver medication [89]. One of the promising applications is smart contact lenses, which can be designed to monitor glucose levels continuously in tears, providing real-time data for diabetes management [90].
- Toric lenses for astigmatism: Toric lenses are designed to specifically correct astigmatism, a condition arising from an irregular shape in the cornea, among other causes. Modern toric lenses are designed using advanced stabilization technologies to enable proper lens orientation on the eye, thus optimizing visual correction [91].
- Nanotechnology: Nanotechnology has been used to introduce nanomaterials into contact lenses, improving characteristics, such as wettability, oxygen permeability, and protection against UV. The traditional contact lenses will sometimes dry out, thereby causing discomfort and reduced vision. Incorporating nanomaterials in the lens surface can give a hydrophilic or water-loving coating, which enhances moisture retention property of the lens, hence making contact lenses comfortable and minimizing dryness. The cornea requires oxygen to remain healthy. Traditional contact lenses restrict oxygen flow, thus causing discomfort and complications. Nanomaterials can be embedded within the lens material to create microscopic channels that allow more oxygen to penetrate and ensure proper oxygenation of the cornea, such as brimonidine noisome-based contact lens (Table 5) [92].
Table 5 Summary of Recent Experimental Studies on Ocular Contact Lens
| Sl. No. | Model Drug | Dosage Form | Carrier Platform | Result | References |
|---|---|---|---|---|---|
| 1. | Timolol | Contact lens | Gold nanoparticles | Encouraged outcomes in animal model to treat glaucoma | [149] |
| 2. | Flurbiprofen | Contact lens | Nanoaggregates | Sustained release of the drug | [150] |
| 3. | Phomopsidione | Contact lens | Nanoparticles | Sustained release of drug for 48 h | [151] |
| 4. | Brimonidine | Soft contact lens | Niosome | Reduced intraocular pressure and treat glaucoma | [152] |
| 5. | Latanoprost | Soft contact lens | Nano-emulsion | Sustained release for glaucoma | [153] |
| 6. | Cyclosporine A | Soft contact lens | Nanoparticles | Treatment of dry eye | [154] |
| 7. | Resveratrol | Contact lens | Hydrogel | Anti-inflammatory and antioxidant effects | [155] |
| 8. | Diclofenac | Contact lens | Nanocapsules | Treatment of ocular inflammation | [156] |
| 9. | Ketorolac | Soft contact lens | Drug –bandage lens | Pain relief | [157] |
| 10. | Ciprofloxacin | Soft contact lens | Nanoparticles | Treatment of bacterial keratitis | [158] |
| 11. | Gentamicin | Soft contact lens | Nanoparticles | Treatment of bacterial conjunctivitis | [159] |
| 12. | Voriconazole | Soft contact lens | Nanoparticles | Treatment of fungal keratitis | [160] |
| 13. | Erythromycin | Soft contact lens | Nanoparticles | Treatment of bacterial blepharitis | [161] |
| 14. | Pilocarpine | Soft contact lens | Nanoparticles | Treatment of glaucoma | [162] |
| 15. | Travoprost | Soft contact lens | Microemulsion | Reduced intraocular pressure | [163] |
| 16. | Bimatoprost | Soft contact lens | Nanocapsules | Treatment of glaucoma | [164] |
| 17. | Dorzolamide | Soft contact lens | Nanoparticles | Used in the eye to treat open-angle glaucoma and high pressure in the eye | [165] |
| 18. | Brinzolamide | Soft contact lens | Nanoemulsion | Reduced intraocular pressure | [166] |
| 19. | Timolol + Brimonidine | Soft contact lens | Nanoparticles | Treatment of glaucoma | [167] |
| 20. | Bimatoprost + Timolol | Soft contact lens | Nanoparticles | Used to treat glaucoma and ocular hypertension | [168] |
| 21. | Dorzolamide + Timolol | Soft contact lens | Nanoparticles | Pressure in the eye lowered by decreasing the production of natural fluids in the eye | [169] |
These advances in contact lens technology have significantly improved the quality of vision correction and the overall experience for millions of wearers worldwide.
Microneedles
Dr. Ernst Kromayer provided the earliest known proof of microneedle use in 1905 when he proposed using motorized dental burs to cure hyperpigmentation and scarring. There was an increase in interest in the delivery of medications by microneedle platforms in the 1960s.
Microneedles are increasingly showing promise as a delivery device to provide precise, less invasive, and localized pharmaceutical administration for ocular illnesses [93]. Administering microneedles to delicate organs, like the eye, can be difficult. To effectively deliver drugs to the eye using microneedles, a number of challenges must be addressed, including the restricted surface area for drug deposition, sensitivity to pressure changes, and variability in the biomechanical properties of ocular tissues. Using conventional hypodermic needles for drug delivery to the intraocular part of the eye is very difficult because of associated pain, irritation, and discomfort [94].
Merits of microneedles
- As possible drug delivery systems, microneedle arrays have many benefits, including minimum invasiveness, the capacity to bypass the human body’s external barriers that reduce the effectiveness of topical formulations, and ease of administration without expert assistance. Poor bioavailability is typically one of the most significant issues that arises when administering drugs to the eyes [94, 95].
- Some types of microneedles, including dissolving microneedles, can be engineered to have a sustained delivery of large molecules, including biologics in ocular tissues. This attribute may allow reduced frequency of administrations for chronic ocular conditions [96].
- Due to the small size, microneedles cause the least discomfort, which may lead to the improvement of needle phobia and patient compliance, especially when administered intravitreal injections. Use of microneedles reduce needle stick injuries and provide safety [96].
- A drug can also be delivered specifically to a chosen ocular site, such as the suprachoroidal space, therefore providing targeted therapy with possibly fewer systemic exposures and side effects [96].
- It provides localized action and reduces tissue trauma compared to conventional hypodermic needles [97].
Limitations of microneedles
- Dissolving microneedles have low mechanical strength, which complicates tissue penetration. Some of the polymers used in fabrication are hygroscopic, reducing the physical stability of the final product [96].
- Small size limits the capacity of microneedles for drug loading and hence might require multiple injections to reach therapeutic levels, especially in the case of chronic ocular diseases.
- Hollow microneedles are more brittle because of the material and small size. The risk of blockage and breakage is more likely to occur during insertion, which would compromise the safety and efficacy of the drug delivery system.
- Fixing microneedle patches onto the ocular surface is not easy. Microneedle patches intended for sustained drug delivery may lose efficacy if the microneedle patches fall off from the application site [97].
- The invasive nature of microneedles is likely to cause irritation and discomfort, which may impact patient compliance. For successful adherence to treatment regimens, ensuring patient comfort with microneedle-based ocular therapy is critical [97]
Types of microneedles in ocular delivery system
Different criteria can be used to classify microneedles, which come under vaccine delivery and diagnostics. Microneedle categorizations are mainly dependent on geometry, the base material used to fabricate the systems, fabrication technology, and drug-loading technique for targeted delivery of intended drugs [97]. The different types of microneedles are as follows: solid microneedles; solid-coated microneedles; dissolving microneedles; hollow microneedles; and hydrogel-forming microneedles.
Of these types of microneedles, solid-coated, dissolving, and hollow microneedles are frequently used for ocular therapy according to recent trends.
- Solid-coated microneedles: Coated microneedles are designed on the “coat-and-poke” principle, where therapeutic agents are loaded onto the tips of solid microneedles, then inserted into the target ocular tissue (Table 6). Coated microneedles dissolve quickly after application to directly deliver the drug upon insertion. This method overcomes the structural barriers in the eye, enables efficient delivery, and significantly reduces the dose compared to traditional methods of drug administration. Solid-coated microneedles create micron-sized channels for easier and more effective drug delivery in a controlled manner in the sclera and cornea tissue. The needles are removed after dissolution of the coating and leave the pores for drug penetration. These coated microneedles frequently are made of non-biodegradable materials, such as stainless steel and silicon probes that provide excellent mechanical properties. Coated microneedles also have limitations. The needle imposes a limited drug-loading capacity and hence may require frequent administration with limited sustained-release ability (only limited by the surface area of the needle). Moreover, an uneven distribution of coatings or improper coating materials can also cause the release of drugs to be inconsistent and ineffective in targeting chronic ocular diseases. In addition, the process of coating can leave needle tips less sharp, which reduces the ability to penetrate and deliver [98].
- Dissolving microneedles: Dissolving microneedles are fabricated by incorporating drug molecules into biodegradable and biocompatible polymers, such as polyvinyl alcohol (PVA), polyvinyl pyrrolidone (PVP), and hyaluronic acid (Table 6). These polymeric microneedles rapidly dissolve in the presence of tear fluid in a few minutes and release the therapeutic agents into the target site. While carrying the drug directly to the eye, administration of dissolving microneedles is quite simple (patient-friendly). Typically only gentle thumb pressure is required on top of eye surface to place contact lens. Indeed, dissolving microneedles have been used in lens-based contact lenses to improve drug penetration as a familiar mode of treatment delivery for patients. This method has been shown to deliver small molecules, such as pilocarpine to the anterior segment of the eye. The major benefit of dissolving microneedles is biocompatibility and biodegradability. Because the microneedles degrade in situ there are no biohazardous sharps to dispose of, which can leave fragments of a solid microneedle behind in the eye in the case of breakage [99].
- Hollow microneedles: Hollow microneedles are micro-scale needles that are used to inject liquid formulations into the skin, similar to conventional hypodermic needles. Normally hollow microneedles are made of stainless steel, silicon, glass, or biodegradable polymers (Table 6). Hollow microneedles are much smaller than traditional hypodermic needles, ranging from 27–35 gauge (outer diameter) and 150 μm in length compared to conventional needles size (usually 26–30 gauge and ≥ 2 mm in length). The smaller size also enables localized and minimally invasive ocular delivery, increasing patient comfort and possibly improving treatment compliance. For ocular applications, hollow microneedles are configured to contain and maintain the drug formulation inside the lumen of the needle, providing direct delivery into ocular tissues upon insertion. It is very useful to have these systems in place with nanoparticles and microparticulate formulations, which mediate target-infused release. Hollow microneedles have also been used in post-ocular therapy for transdermal delivery (e.g., insulin and vaccines) [96]. Hollow microneedles are fabricated using various methods, such as the micropipette puller technique, where a borosilicate glass micropipette tube is stretched and formed to develop the hollow wish. Although borosilicate tubes could be applied in experimental settings but the poor resistance would make hollow microneedles subject to easy breakage. Thus, hollow microneedles are inappropriate for regular clinical use. Materials, like stainless steel and some biodegradable polymers, are used for stronger material and safety [100].
Table 6 Summary and Comparative Overview of Microneedle Types and Applications in Targeted Ocular Drug Delivery
| Sl.No. | Microneedle Types | Characteristics | Specific Applications | Recent Approaches | References |
|---|---|---|---|---|---|
| 1. | Solid (uncoated) microneedles | Sharp solid MNs fabricated from metals or silicon that create micro channels upon insertion; typically followed by topical drug application over pores. | Enhancing permeability of drug patches by forming micro pores in the cornea or sclera | Enhanced delivery of anti-glaucoma drugs (e.g., timolol) and imaging agents into sclera for diagnostics | [93] |
| 2. | Coated microneedles | Solid needles coated with drug formulations that dissolve immediately upon insertion (“coat-and-poke”); limited by surface-area drug loading | Fast deposition of small molecules (pilocarpine and fluorescein) and macromolecules (proteins and DNA) into ocular tissues with high bioavailability | Delivery of anti-VEGF biologics and corticosteroids for macular degeneration and uveitis | [170] |
| 3. | Dissolving microneedles | Made from biodegradable polymers (PVA, PVP, and hyaluronic acid); dissolve within minutes in aqueous environment; leave no sharp waste; limited drug load and patch curvature issues | Patient-friendly delivery—e.g., contact lens-based MNs—for small molecules (like pilocarpine); sustained release via formulation tuning | Nanoparticle-loaded dissolving MNs for sustained delivery of latanoprost in glaucoma models | [107] |
| 4. | Hollow microneedles | Miniaturized hollow needles (150 μm+, 27–35 gauge) fabricated from glass, metals, or polymers; costly and brittle with risk of blockage or breakage | Direct injection of liquid formulations, including nanoparticles/microparticles into ocular tissues; also used in transdermal vaccines/insulin | Suprachoroidal delivery of gene therapy vectors and long-acting anti-inflammatory drugs | [97] |
| 5. | Hydrogel-forming microneedles | Swellable, crosslinked hydrogel MNs (e.g., chitosan, hyaluronic acid, and PVA); absorb interstitial fluid, forming a drug-laden gel network for sustained release | Controlled and sustained ocular drug release; potential replacement for frequent intravitreal injections | Extended release of antibiotics for corneal infections using hydrogel MN patches | [171] |
Recent microneedle advances
Recent advances in microneedle technology have greatly improved ocular drug delivery, providing a precise, minimally invasive treatment for a range of eye diseases.
- Minimally invasive for ocular delivery: Bypassing the barriers, like the tear film and conjunctiva, microneedles can transport medications straight into ocular tissues, such as the cornea, sclera, or retina. By directing the medication to the eye, all of the systemic adverse effects linked to traditional administration methods are reduced [97]. Recent advances in microneedle fabrication techniques, materials, dimensions, delivery routes, and therapeutic applications for ocular drug delivery are summarized in Table 7. Several microneedle-based products for ocular drug delivery have reached clinical development or commercialization, targeting both anterior and posterior segment diseases. An overview of marketed and advanced microneedle products is provided in Table 8.
- Enhanced drug delivery systems: Microneedles allow targeted delivery of drugs into ocular tissues, which enhances the therapeutic outcome. Microneedles can penetrate through barriers, such as the cornea and sclera, to ensure effective drug administration [101].
- Polysaccharide-containing microneedles: Polysaccharides are vital structural components of the eye that have a crucial role in maintaining the normal physiologic state [102]. Polysaccharide-based microneedle systems are said to be studied for the development of ocular drug delivery because these biocompatible materials may improve the profile of drug release and reduce adverse effects. Polysaccharides, for example, hyaluronic acid, offer structural support and hydration to the cornea, and therefore maintain the cornea as a transparent, refracting tissue. Polysaccharides with collagen make a matrix that gives elasticity and toughness to the sclera and protects the eye against outer pressure and injury [103, 104].
- Autonomous insertion: Innovations in autonomous microneedle insertion techniques have improved precision in delivering drugs to specific intraocular sites, enhancing treatment efficacy and safety. Access of the suprachoroidal space by microneedles to the back of the eye continues to allow targeted delivery. This method has proven efficacy in treating posterior segment diseases [105].
Table 7 Summary of Different Materials and Fabrication Techniques for Ocular Microneedles
| Sl. No. | Materials | Fabrication Technique | Materials Properties | Dimension | Volume | Target Location | Applications | Clinical Implications | References |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Glass | Micro-pulling process | Biocompatible, smooth surface | 700-800 μm, 25° bevel angle | 10-35 μl | Sclera | Distribution of solution and nanoparticles in sclera | Enhanced drug distribution without tissue damage | [172] |
| 2. | Glass | UV lithography | Transparent, mechanically robust | 300 μm long array of MNs | 10-35 μl | Sclera | Delivery of rose bengal dye in porcine sclera | Precise dosing for anterior segment therapies | [173] |
| 3. | Glass | Thermal technique | High accuracy in nanoparticle delivery | 750 μm | 50 μl | Suprachoroidal spaces | Delivery of nano- (20 and 200 nm) and micro-particles (2 and 10 μm) | Improved posterior drug targeting | [174] |
| 4. | Metal | Laser cutting | High tensile strength, corrosion-resistant | 400, 500, and 600 μm, 27, 29, and 30 G | <10 μL | Sclera | Delivery of sunitinib-loaded Cs-g-PNIPAAm hydrogel | Sustained drug release with minimal tissue disruption | [94] |
| 5. | Metal | CNC machining | Customizable bevel angles, strong materials | <1 mm, 30 and 33 G | 200 μL | Scs | Gravity-mediated targeting of perfluorodecalin encapsulated with fluorescein-tagged polystyrene nanoparticles to SCS | Effective treatment for macular edema | [100] |
| 6. | Metal | Precision casting | Robust and flexible for repetitive use | 750 μm long, 33 G | 50 μL | Scs | Distribution of nanoparticles (200 nm) in SCS | Reduced complications in posterior delivery | [175] |
| 7. | Metal | Electrochemical etching | High biocompatibility, sharp edges | 700 μm long, 30 G | 50 μL | Scs | Trans scleral/sub retinal delivery of adeno-associated virus (AAV8) vectors | Gene therapy delivery with enhanced targeting | [176] |
| 8. | Metal | Microfabrication | Adjustable flow rates, resilient | 750 μm long, 33 G | 50 μL | Scs | Distribution of viscous non-Newtonian solutions in SCS | Delivery of rheologically challenging solutions | [177] |
| 9. | Metal | Laser ablation | Thermo-sensitive, adaptive designs | 750 μm long, 27, 29, and 30 G | 30, 50, and 100 μL | Sclera | Delivery of thermo-responsive depot-forming hydrogels | Long-term drug depot for chronic conditions | [20] |
| 10. | Metal | CNC machining | Lightweight, biocompatible | 750 μm, 30 G | 10–20 μL | Supraciliary route | Distribution of brimonidine-loaded microspheres (20–45 μm) in various supranasal and temporal locations | Improved intraocular pressure reduction | [178] |
Table 8 Overview of Marketed Microneedle Products for Ocular Drug Delivery Products
| Sl. No. | Product Name | Company | Application | References |
|---|---|---|---|---|
| 1. | SCS Microinjector™ | Clearside Biomedical | Delivering drugs to the suprachoroidal space for retinal and choroidal diseases | [179] |
| 2. | Microneedle array | Re-Vana Therapeutics | Sustained drug delivery for diseases, like glaucoma and macular degeneration | [98] |
| 3. | Eyedropper microneedles | Georgia Tech | Delivering drugs directly into the cornea or conjunctiva | [180] |
| 4. | NanoJect™ | Microdermics | Minimally invasive delivery of ophthalmic drugs to anterior or posterior segments | [181] |
| 5. | EyeMN™ | Ophthalmic Innovations | Painless delivery of drugs for retinal diseases and uveitis | [182] |
Clinical translation bottlenecks
The clinical translation of ocular drug delivery systems, such as ocular inserts, contact lenses, and microneedles, face several tailbacks. Sometimes it is difficult to recruit and maintain the active participation of patients because it may lead to increased risks of irritation, infections, or tissue damage or blurred vision. These effects may reduce patient compliance and adherence to the therapy. Regulatory aspects are another challenge that requires long-term safety and efficacy for drug device combination products. Technical challenges include large-scale production, which maintains the sterility and stability for the shelf life of the product. All these challenges slow the journey of these new delivery systems from research labs to real patient use [106, 107].
Regulatory perspectives
Ophthalmic formulations are considered a class of complex products challenging in chemistry, manufacturing, and control by the US Food and Drug Administration (FDA). The extended-release oral medicines for ocular disease were issued by the US FDA in 1997 [108]. The WHO, the FDA, and the European Medicines Agency (EMA) are prominent and highly respected regulatory bodies, but according to the Federal Food, Drug & Cosmetic Act (FD & C Act [1938]), the FDA only has legal authority to regulate medical devices in the US [109].
Regulatory strategies for ocular inserts ensures its safe, effective, and easy use for patients. The FDA requires ocular inserts to be sterile under 21 CFR 200.50 and to pass biocompatibility tests (ISO 10993-1) to ensure ocular inserts will not cause irritation or allergic reactions. Stability testing, as per ICH Q1A-Q1E, must confirm that the product maintains quality over time and a quality-by-design (QbD) approach under ICH Q8 (R2) helps fine-tune the formulation and manufacturing to consistently deliver safe, high-quality inserts [108]. Title 21 CFR, Parts 800-1299, contains information about medical devices as well as products that generate radiation. The Premarket Notification (510K) Guidance Document for Class II Daily Wear Contact Lenses was published by US regulatory authorities in 1994. In the US contact lenses have been regulated by the FDA since the 1960s with soft hydrogels. Following the 1976 Medical Device Amendment, extended-wear lenses became Class III devices, which require pre-market authorization. Daily-wear and RGP lenses were classified as Class II in 1994 with all contact lenses falling under Class II by 1997. Both are low-risk and need Institutional Review Board approval [110]. The first regulatory policy for microneedle-products was issued in 2017 to guide industries on such products under section 201(h) of the federal FD&C Act, 21 U.S.C. § 321(h). The guidance outlines the regulatory pathway for marketing these devices for aesthetic use [111].
Methodology of data collections
This comprehensive review search was conducted on recent advances in ocular delivery systems with a focus on ocular inserts, contact lenses, and microneedles. The databases and search engines used included Google Scholar, PubMed, NCBI, NIH, Taylor & Francis, and the Wiley Online Library. The search covered publications from 2003–2025 by using combinations of keywords, such as “ocular delivery systems,” “ocular inserts,” “drug delivery contact lenses,” “ocular microneedles,” “sustained release,” and “recent advancements.” Reference lists of selected articles were also screened to identify additional relevant publications. Data from the included studies were synthesized to highlight current progress, key innovations, and gaps for future research and the images were drawn using Biorender.com.
Conclusion
The recent advances in ocular inserts, contact lenses, and microneedles have shown significance translational value and promise for sustained drug release, site-specific delivery, and enhanced patient compliance over conventional therapy. These innovations represent a potential kinetic middle ground from basic laboratory research to clinical outcome improvements by improving bioavailability, decreasing dosing frequency, and minimally invasive administrations. The major challenges with these systems are large-scale manufacturing, long-term biocompatibility, patient compliance, and adherence. Increase integration of diagnostic, monitoring, or adjunct therapeutic functions in these devices would likely require better effectiveness.
Future perspectives
The future trends would aim at combining current advances in ocular drug delivery systems with modern day smart drug delivery system. The delivery systems in our body should be able to discriminate and respond to real time physiologic signals, like intraocular pressure, composition of tears, or a state of disease progression for timely drug release. This will allow for an individualized therapeutic approach, enabling drug type, dose, and delivery route to be matched with genetic profiling as well as patient-specific disease biomarkers to achieve the best benefit-risk profile. In addition, next-generation delivery platforms, such as biotechnical ocular inserts, nanocarrier-based microneedles, and multi-functional contact lenses are projected to bring together the benefits of sustained release, targeted delivery and diagnostics all in one system offering high efficacy patient-centric ocular disease management.
Funding
No funding or sponsorship was received for this study.
Acknowledgements
The authors would like to thank Amity Institute of Pharmacy, Amity University Uttar Pradesh, and Lucknow Campus for providing the library facilities for review work.
Conflict of interest
The authors declare that there are no conflicts of interest.
Consent for publication
Not applicable.
List of abbreviations
| SNEDDS | self-nano emulsifying drug delivery systems |
| IOP | intraocular pressure |
| BAB | blood-aqueous barrier |
| BRB | blood-retinal barrier |
| RPE | retinal pigment epithelium |
| HA | hyaluronic acid |
| SCS | suprachoroidal space |
| WHO | World Health Organization |
| FDA | Food & Drug Administration |
| EMA | European Medicine Agency |
| IRB | Institutional Review Board |
Graphical abstract

Highlights
- A brief discussion of the anatomy and physiology of the eye, including ocular barriers, is presented.
- Recent advances in ocular inserts for sustained and targeted drug delivery are reviewed. Innovative drug-eluting contact lenses for improving ocular bioavailability are discussed. Progress in microneedle-based systems for minimally invasive ocular delivery is highlighted.
- Challenges, clinical potential, and future perspectives of advanced ocular drug delivery systems are summarized.
In brief
Recent advances in ocular drug delivery systems (ocular barriers, drug carriers and inserts, contact lenses, and microneedle advances for enhanced delivery).
References
- Patel A, Cholkar K, Agrahari V, Mitra AK. Ocular drug delivery systems: an overview. World J Pharmacol 2013;2(2):47-67. [PMID: 25590022 DOI: 10.5497/wjp.v2.i2.47]
- Mudgil M, Gupta N, Nagpal M, Pawar P. Nanotechnology: a new approach for ocular drug delivery system. Int J Pharm Pharm Sci 2012;4(2):105-12.
- Singh M, Bharadwaj S, Lee KE, Kang SG. Therapeutic nanoemulsions in ophthalmic drug administration: concept in formulations and characterization techniques for ocular drug delivery. J Control Release 2020;328:895-916. [PMID: 33069743 DOI: 10.1016/j.jconrel.2020.10.025]
- Han H, Li S, Xu M, Zhong Y, Fan W, et al. Polymer- and lipid-based nanocarriers for ocular drug delivery: current status and future perspectives. Adv Drug Deliv Rev 2023;196:114770. [PMID: 36894134 DOI: 10.1016/j.addr.2023.114770]
- Liu LC, Chen YH, Lu DW. Overview of recent advances in nano-based ocular drug delivery. Int J Mol Sci 2023;24(20):15352. [PMID: 37895032 DOI: 10.3390/ijms242015352]
- Nishida T, Saika S. Cornea and sclera: anatomy and physiology. Cornea 2011;8:3-24. [DOI: 10.1016/B978-0-323-06387-6.00008-8]
- Assiri AA, Glover K, Mishra D, Waite D, Vora LK, et al. Block copolymer micelles as ocular drug delivery systems. Drug Discov Today 2024;29(8):104098. [PMID: 38997002 DOI: 10.1016/j.drudis.2024.104098]
- Tsung TH, Tsai YC, Lee HP, Chen YH, Lu DW. Biodegradable polymer-based drug-delivery systems for ocular diseases. Int J Mol Sci 2023;24(16):12976. [PMID: 37629157 DOI: 10.3390/ijms241612976]
- Gaudana R, Jwala J, Boddu SH, Mitra AK. Recent perspectives in ocular drug delivery. Pharm Res 2009;26(5):1197-216. [PMID: 18758924 DOI: 10.1007/s11095-008-9694-0]
- Ezike TC, Okpala US, Onoja UL, Nwike CP, Ezeako EC, et al. Advances in drug delivery systems, challenges and future directions. Heliyon 2023;9(6):e17488. [PMID: 37416680 DOI: 10.1016/j.heliyon.2023.e17488]
- Ahmed S, Amin MM, Sayed S. Ocular drug delivery: a comprehensive review. AAPS PharmSciTech 2023;24(2):66. [PMID: 36788150 DOI: 10.1208/s12249-023-02516-9]
- Raj VK, Mazumder R, Madhra M. Ocular drug delivery system: challenges and approaches. Int J App Pharm 2020;12(5):49-57. [DOI: 10.22159/ijap.2020v12i5.38762]
- Das S, Saha D, Majumdar S, Giri L. Imaging methods for the assessment of a complex hydrogel as an ocular drug delivery system for glaucoma treatment: opportunities and challenges in preclinical evaluation. Mol Pharm 2022;19(3):733-48. [PMID: 35179892 DOI: 10.1021/acs.molpharmaceut.1c00831]
- Gote V, Sikder S, Sicotte J, Pal D. Ocular drug delivery: present innovations and future challenges. J Pharmacol Exp Ther 2019;370(3):602-24. [PMID: 31072813 DOI: 10.1124/jpet.119.256933]
- Pelusi L, Mandatori D, Mastropasqua L, Agnifili L, Allegretti M, et al. Innovation in the development of synthetic and natural ocular drug delivery systems for eye diseases treatment: focusing on drug-loaded ocular inserts, contacts, and intraocular lenses. Pharmaceutics 2023;15(2):625. [PMID: 36839947 DOI: 10.3390/pharmaceutics15020625]
- Macha S, Hughes PM, Mitra AK. Overview of ocular drug delivery. In: Mitra AK, editor. Ophthalmic drug delivery systems. CRC Press; 2003. pp. 22-33. [DOI: 10.1201/9780203912072]
- Irsch K, Guyton DL. Anatomy of eyes. In: Li SZ, Jain A, editors. Encyclopedia of biometrics. Boston, MA: Springer; 2009. pp. 11-16. [DOI: 10.1007/978-0-387-73003-5_253]
- Kaplan HJ. Anatomy and function of the eye. Chem Immunol Allergy 2007;92:4-10. [PMID: 17264478 DOI: 10.1159/000099236]
- Mafee MF, Karimi A, Shah J, Rapoport M, Ansari SA. Anatomy and pathology of the eye: role of MR imaging and CT. Neuroimaging Clin N Am 2005;15(1):23-47. [PMID: 15927859 DOI: 10.1016/j.nic.2005.02.005]
- Cholkar K, Dasari SR, Pal D, Mitra AK. Eye: anatomy, physiology and barriers to drug delivery. In: Ocular transporters and receptors. Woodhead Publishing; 2013. pp. 1-36. [DOI: 10.1533/9781908818317.1]
- Zhu J, Zhang E, Del Rio-Tsonis K. Eye anatomy. Encyclopedia of Life Sciences; 2012. [DOI: 10.1002/9780470015902.a0000108.pub2]
- Nishida T, Saika S, Morishige N. Cornea and sclera: anatomy and physiology. In: Mannis MJ, Holland EJ, editors. Cornea: fundamentals, diagnosis and management. 4th ed. New York: Elsevier; 2017. pp. 1-22.
- Mulvey F. Eye anatomy, eye movements and vision. In: Gaze interaction and applications of eye tracking: advances in assistive technologies. IGI Global Scientific Publishing; 2012. pp. 10-20. [DOI: 10.4018/978-1-61350-098-9.ch002]
- Ansari MW, Nadeem A. Atlas of ocular anatomy. Cham: Springer; 2016. [DOI: 10.1007/978-3-319-42781-2]
- Bertelli E. Anatomy of the eye and human visual system. Padua, Italy: Piccin Nuova Libraria S.p.A; 2019.
- Boddu SH, Menees AL, Ray A, Mitra AK. A brief overview of ocular anatomy and physiology. In: Mitra AK, editor. Treatise on ocular drug delivery. Bentham Science; 2013. pp. 3-19. [DOI: 10.2174/97816080517551130101]
- Hughes MO. Anatomy of the anterior eye for ocularists. J Ophthalmic Prosthet 2004;8:25-35.
- Leclercq B, Mejlachowicz D, Behar-Cohen F. Ocular barriers and their influence on gene therapy products delivery. Pharmaceutics. 2022;14(5):998. [PMID: 35631584 DOI: 10.3390/pharmaceutics14050998]
- Redzic ZB, Segal MB. The structure of the choroid plexus and the physiology of the choroid plexus epithelium. Adv Drug Deliv Rev 2004;56(12):1695-716. [PMID: 15381330 DOI: 10.1016/j.addr.2004.07.005]
- Wang L, Zhang H. Ocular barriers as a double-edged sword: preventing and facilitating drug delivery to the retina. Drug Deliv Transl Res 2023;13(2):547-67. [PMID: 36129668 DOI: 10.1007/s13346-022-01231-5]
- Maulvi FA, Shetty KH, Desai DT, Shah DO, Willcox MDP. Recent advances in ophthalmic preparations: ocular barriers, dosage forms and routes of administration. Int J Pharm 2021;608:121105. [PMID: 34537269 DOI: 10.1016/j.ijpharm.2021.121105]
- Eghrari AO, Riazuddin SA, Gottsch JD. Overview of the cornea: structure, function, and development. Prog Mol Biol Transl Sci 2015;134:7-23. [PMID: 26310146 DOI: 10.1016/bs.pmbts.2015.04.001]
- Bernardes R, Dias J, Cunha-Vaz J. Mapping the human blood-retinal barrier function. IEEE Trans Biomed Eng 2004;52(1):106-16. [PMID: 15651569 DOI: 10.1109/TBME.2004.839801]
- Gote V, Ansong M, Pal D. Prodrugs and nanomicelles to overcome ocular barriers for drug penetration. Expert Opin Drug Metab Toxicol 2020;16(10):885-906. [PMID: 32729364 DOI: 10.1080/17425255.2020.1803278]
- Gunda S, Hariharan S, Mandava N, Mitra AK. Barriers in ocular drug delivery. In: Tombran-Tink J, Barnstable CJ, editors. Ocular transporters in ophthalmic diseases and drug delivery: ophthalmology research. New Jersey: Humana Totowa; 2008. pp. 399-413. [DOI: 10.1007/s11095-008-9694-0]
- Li S, Chen L, Fu Y. Nanotechnology-based ocular drug delivery systems: recent advances and future prospects. J Nanobiotechnol 2023;21(1):232. [DOI: 10.1186/s12951-023-01992-2]
- Chen MS, Hou PK, Tai TY, Lin BJ. Blood-ocular barriers. Tzu Chi Med J 2008;20(1):25-34. [DOI: 10.1016/S1016-3190(08)60004-X]
- Freddo TF. A contemporary concept of the blood–aqueous barrier. Progr Retin Eye Res 2013;32:181-95. [PMID: 23128417 DOI: 10.1016/j.preteyeres.2012.10.004]
- Lee J, Pelis RM. Drug transport by the blood–aqueous humor barrier of the eye. Drug Metab Dispos 2016;44(10):1675-81. [PMID: 26895982 DOI: 10.1124/dmd.116.069369]
- Coca-Prados M. The blood-aqueous barrier in health and disease. J Glaucoma 2014;23(suppl 1):S36-8. [DOI: 10.1097/IJG.0000000000000107]
- Cunha-Vaz J, Bernardes R, Lobo C. Blood-retinal barrier. Eur J Ophthalmol 2011;21(suppl 6):3-9. [PMID: 23264323 DOI: 10.5301/EJO.2010.6049]
- Runkle EA, Antonetti DA. The blood-retinal barrier: structure and functional significance. Methods Mol Biol 2011;686:133-48. [PMID: 21082369 DOI: 10.1007/978-1-60761-938-3_5]
- Wilson S, Ctori I, Shah R, Conway ML, Willis SJ, et al. An investigation of barriers and enablers to community eye care for children in England: a qualitative descriptive study. Ophthalmic Physiol Opt 2023;43(4):710-24. [PMID: 36881493 DOI: 10.1111/opo.13109]
- Raviola G. The structural basis of the blood-ocular barriers. Exp Eye Res 1977;25(suppl):27-63. [DOI: 10.1016/S0014-4835(77)80009-2]
- Patel PB, Shastri D, Shelat P, Shukla A. Ophthalmic drug delivery system: challenges and approaches. Syst Rev Pharm 2010;1(2):113. [DOI: 10.4103/0975-8453.75042]
- del Amo EM. Topical ophthalmic administration: can a drug instilled onto the ocular surface exert an effect at the back of the eye? Front Drug Deliv 2022;2:954771. [DOI: 10.3389/fddev.2022.954771]
- Jenita JJ, Rathore SS, Manjula D, Barnabas W. Packaging, container, and closure of ophthalmic products. In: Mehra NK, editor. Complex ophthalmic dosage forms: advances in biomedical applications and future perspectives. Singapore: Springer Nature Singapore; 2025. pp. 355-392. [DOI: 10.1007/978-981-96-6306-4_12]
- Tsung TH, Chen YH, Lu DW. Updates on biodegradable formulations for ocular drug delivery. Pharmaceutics 2023;15(3):734. [PMID: 36986595 DOI: 10.3390/pharmaceutics15030734]
- Kalantzis GK, Verity DH, Rose GE. Periocular implantation cysts: a late complication of ophthalmic surgery. Eye 2014;28(8):1004-7. [PMID: 24924444 DOI: 10.1038/eye.2014.111]
- Yetgin C, Demiröz FNT, Takka T. Ocular drug delivery routes: diseases overview and advanced administration methods. Fabad J Pharm Sci 2024;49(3):627-46. [DOI: 10.55262/fabadeczacilik.1496246]
- Bisht R, Mandal A, Jaiswal JK, Rupenthal ID. Nanocarrier mediated retinal drug delivery: overcoming ocular barriers to treat posterior eye diseases. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2018;10(2):e1473. [PMID: 28425224 DOI: 10.1002/wnan.1473]
- Thang NH, Chien TB, Cuong DX. Polymer-based hydrogels applied in drug delivery: an overview. Gels 2023;9(7):523. [PMID: 37504402 DOI: 10.3390/gels9070523]
- Viswanadhan Vasantha P, Sherafudeen SP, Rahamathulla M, Mathew ST, Murali S, Alshehri S, et al. Combination of cellulose derivatives and chitosan-based polymers to investigate the effect of permeation enhancers added to in situ nasal gels for the controlled release of loratadine and chlorpheniramine. Polymers 2023;15(5):1206. [DOI: 10.3390/polym15051206]
- Allen TM, Cullis PR. Liposomal drug delivery systems: from concept to clinical applications. Adv Drug Deliv Rev 2013;65(1):36-48. [PMID: 23036225 DOI: 10.1016/j.addr.2012.09.037]
- Taskar P, Tatke A, Majumdar S. Advances in the use of prodrugs for drug delivery to the eye. Expert Opin Drug Deliv 2017;14(1):49-63. [PMID: 27441817 DOI: 10.1080/17425247.2016.1208649]
- Mahlumba P, Choonara YE, Kumar P, Du Toit LC, Pillay V. Stimuli-responsive polymeric systems for controlled protein and peptide delivery: future implications for ocular delivery. Molecules 2016;21(8):1002. [PMID: 27483234 DOI: 10.3390/molecules21081002]
- Kuno N, Fujii S. Recent advances in ocular drug delivery systems. Polymers 2011;3(1):193-221. [DOI: 10.3390/polym3010193]
- Devhadrao NV, Siddhaia M. Review on ocular insert drug delivery system. J Drug Deliv Ther. 2018;8(5-S):115-21. [DOI: 10.22270/jddt.v8i5-s.1991]
- Sahane NK, Banarjee SK, Gaikwad DD, Jadhav SL, Throat RM. Ocular inserts: a review. Drug Invent Today 2010;2(1):57-64.
- Turaeva A, Bakhrushina E, Zhalyalova D, Korochkina T, Stepanova O, et al. Ocular inserets as a modern therapy trend in opthalmopathology. Int J App Pharm 2023;15(6):45-52. [DOI: 10.22159/ijap.2023v15i6.49037]
- Kumar BP, Harish G, Bhowmik D. Ocular inserts: a novel controlled drug delivery system. Pharma Innovation 2013;1(12):16. [DOI: 10.4018/978-1-61350-353-9.ch001]
- Farkas E, Abboud H, Nagy N, Hofmeister B, Ostorházi E, et al. Formulation and development of nanofiber-based ophthalmic insert for the treatment of bacterial conjunctivitis. Int J Mol Sci 2024;25(17):9228. [PMID: 39273175 DOI: 10.3390/ijms25179228]
- Bertens CJF, Martino C, van Osch MC, Lataster A, Dias AJAA, et al. Design of the ocular coil, a new device for non-invasive drug delivery. Eur J Pharm Biopharm 2020;150:120-30. [DOI: 10.1016/j.ejpb.2020.03.010]
- Yu W, Wu Z. Ocular delivery of CRISPR/Cas genome editing components for treatment of eye diseases. Adv Drug Deliv Rev 2021;168:181-95. [PMID: 32603815 DOI: 10.1016/j.addr.2020.06.011]
- Gade SK, Nirmal J, Garg P, Venuganti VVK. Corneal delivery of moxifloxacin and dexamethasone combination using drug-eluting mucoadhesive contact lens to treat ocular infections. Int J Pharm 2020;591:120023. [PMID: 33127488 DOI: 10.1016/j.ijpharm.2020.120023]
- García-Estrada P, García-Bon MA, López-Naranjo EJ, Basaldúa-Pérez DN, Santos A, et al. Polymeric implants for the treatment of intraocular eye diseases: trends in biodegradable and non-biodegradable materials. Pharmaceutics 2021;13(5):701. [PMID: 34065798 DOI: 10.3390/pharmaceutics13050701]
- Pereira ICF, van Mechelen RJS, Wyss HM, Pinchuk L, Beckers HJM, et al. Magnetically actuated glaucoma drainage device for regulating intraocular pressure after implantation. Microsyst Nanoeng 2023;9(1):92. [PMID: 37484503 DOI: 10.1038/s41378-023-00561-9]
- Rykowska I, Nowak I, Nowak R. Soft contact lenses as drug delivery systems: a review. Molecules 2021;26(18):5577. [PMID: 34577045 DOI: 10.3390/molecules26185577]
- Morrison PW, Khutoryanskiy VV. Advances in ophthalmic drug delivery. Ther Deliv 2014;5(12):1297-315. [PMID: 25531930 DOI: 10.4155/tde.14.75]
- Franco P, De Marco I. Contact lenses as ophthalmic drug delivery systems: a review. Polymers (Basel) 2021;13(7):1102. [PMID: 33808363 DOI: 10.3390/polym13071102]
- Choi SW, Kim J. Therapeutic contact lenses with polymeric vehicles for ocular drug delivery: a review. Materials (Basel) 2018;11(7):1125. [PMID: 29966397 DOI: 10.3390/ma11071125]
- Hynes A. The promise of drug-eluting contact lenses. Mod Optom 2024:11-3. Available from: https://modernod.com/topics/contact-lenses/the-promise-of-drug-eluting-contact-lenses/38780/.
- Ciolino JB, Hoare TR, Iwata NG, Behlau I, Dohlman CH, et al. A drug-eluting contact lens. Invest Ophthalmol Vis Sci 2009;50(7):3346-52. [PMID: 19136709 DOI: 10.1167/iovs.08-2826]
- Charman WN. Developments in the correction of presbyopia I: spectacle and contact lenses. Ophthalmic Physiol Opt 2014;34(1):8-29. [PMID: 24205890 DOI: 10.1111/opo.12091]
- van der Worp E, Bornman D, Ferreira DL, Faria-Ribeiro M, Garcia-Porta N, et al. Modern scleral contact lenses: a review. Cont Lens Anterior Eye 2014;37(4):P240-50. [DOI: 10.1016/j.clae.2014.02.002]
- Sart S, Ma T, Li Y. Preconditioning stem cells for in vivo delivery. Biores Open Access 2014;3(4):137-49. [PMID: 25126478 DOI: 10.1089/biores.2014.0012]
- Gillespie RL, Lloyd IC, Black GC. The use of autozygosity mapping and next-generation sequencing in understanding anterior segment defects caused by an abnormal development of the lens. Hum Hered 2014;77(1-4):118-37. [PMID: 25060275 DOI: 10.1159/000362599]
- Bengani LC, Hsu KH, Gause S, Chauhan A. Contact lenses as a platform for ocular drug delivery. Expert Opin Drug Deliv 2013;10(11):1483-96. [PMID: 23875917 DOI: 10.1517/17425247.2013.821462]
- Alvarez-Lorenzo C, Hiratani H, Gómez-Amoza JL, Martínez-Pacheco R, Souto C, et al. Soft contact lenses capable of sustained delivery of timolol. J Pharm Sci 2002;91(10):2182-92. [PMID: 12226845 DOI: 10.1002/jps.10209]
- Pearson RM. A review of the limitations of the first hydrogel contact lenses. Clin Exp Optom 2010;93(1):15-25. [PMID: 19961507 DOI: 10.1111/j.1444-0938.2009.00444.x]
- Topete A, Pinto CA, Barroso H, Saraiva JA, Barahona I, et al. High hydrostatic pressure as sterilization method for drug-loaded intraocular lenses. ACS Biomater Sci Eng 2020;6(7):4051-61. [DOI: 10.1021/acsbiomaterials.0c00412]
- Gulsen D, Chauhan A. Ophthalmic drug delivery through contact lenses. Invest Ophthalmol Vis Sci 2004;45(7):2342-7. [PMID: 15223815 DOI: 10.1167/iovs.03-0959]
- White CJ, Byrne ME. Molecularly imprinted therapeutic contact lenses. Expert Opin Drug Deliv 2010;7(6):765-80. [PMID: 20408742 DOI: 10.1517/17425241003770098]
- Kim J, Peng CC, Chauhan A. Extended release of dexamethasone from silicone-hydrogel contact lenses containing vitamin E. J Control Release 2010;148(1):110-6. [PMID: 20691228 DOI: 10.1016/j.jconrel.2010.07.119]
- Bose P. Next-gen contact lenses: beyond vision correction. News Medical; 2024. Available from: https://www.news-medical.net/health/Next-Gen-Contact-Lenses-Beyond-Vision-Correction.aspx.
- Haworth K, Travis D, Leslie L, Fuller D, Pucker AD. Silicone hydrogel versus hydrogel soft contact lenses for differences in patient-reported eye comfort and safety. Cochrane Database Syst Rev 2023;9(9):CD014791. [PMID: 37724689 DOI: 10.1002/14651858.CD014791.pub2]
- Ishihara K, Shi X, Fukazawa K, Yamaoka T, Yao G, et al. Biomimetic-engineered silicone hydrogel contact lens materials. ACS Appl Bio Mater 2023;6(9):3600-16. [PMID: 37616500 DOI: 10.1021/acsabm.3c00296]
- Said O. Advancing multifocal contact lens design with biometry. Optom Times J 2024;16(1). Available from: https://www.optometrytimes.com/view/advancing-multifocal-contact-lens-design-with-biometry.
- Mertz L. Smart contact lenses keep an eye on health. IEEE Pulse 2023;14(3):20-3. [DOI: 10.1109/MPULS.2023.3294087.
- Kazanskiy NL, Khonina SN, Butt MA. Smart contact lenses—a step towards non-invasive continuous eye health monitoring. Biosensors (Basel) 2023;13(10):933. [PMID: 37887126 DOI: 10.3390/bios13100933]
- Rueff E. Stability is an important quality in toric lenses. Optom Times J 2024;16(7). Available from: https://www.optometrytimes.com/view/stability-is-an-important-quality-in-toric-lenses.
- Sakr A, Kamal A, Jacob L, Homsi R, Butt H. Comprehensive review on the synthesis, properties and applications of nanocomposite contact lenses. Polym Rev 2024;65(1):1-46. [DOI: 10.1080/15583724.2024.2400961]
- Glover K, Mishra D, Gade S, Vora LK, Wu Y, et al. Microneedles for advanced ocular drug delivery. Adv Drug Deliv Rev 2023;201:115082. [PMID: 37678648 DOI: 10.1016/j.addr.2023.115082]
- Thakur Singh RR, Tekko I, McAvoy K, McMillan H, Jones D, et al. Minimally invasive microneedles for ocular drug delivery. Expert Opin Drug Deliv 2017;14(4):525-37. [PMID: 27485251 DOI: 10.1080/17425247.2016.1218460]
- Thakur RR, Tekko IA, Al-Shammari F, Ali AA, McCarthy H, et al. Rapidly dissolving polymeric microneedles for minimally invasive intraocular drug delivery. Drug Deliv Transl Res 2016;6(6):800-15. [PMID: 27709355 DOI: 10.1007/s13346-016-0332-9]
- Rojekar S, Parit S, Gholap AD, Manchare A, Nangare SN, et al. Revolutionizing eye care: exploring the potential of microneedle drug delivery. Pharmaceutics 2024;16(11):1398. [PMID: 39598522 DOI: 10.3390/pharmaceutics16111398]
- Gadzinski P, Froelich A, Wojtylko M, Bialek A, Krysztofiak J, et al. Microneedle-based ocular drug delivery systems – recent advances and challenges. Beilstein J Nanotechnol 2022;13(1):1167-84. [PMID: 36348935 DOI: 10.3762/bjnano.13.98]
- Prausnitz MR. Microneedles for transdermal drug delivery. Adv Drug Deliv Rev 2004;56(5):581-7. [PMID: 15019747 DOI: 10.1016/j.addr.2003.10.023]
- Gupta P, Yadav KS. Applications of microneedles in delivering drugs for various ocular diseases. Life Sci 2019;237:116907. [PMID: 31606378 DOI: 10.1016/j.lfs.2019.116907]
- Patel SR, Lin AS, Edelhauser HF, Prausnitz MR. Suprachoroidal drug delivery to the back of the eye using hollow microneedles. Pharm Res 2011;28(1):166-76. [PMID: 20857178 DOI: 10.1007/s11095-010-0271-y]
- Gade S, Glover K, Mishra D, Sharma S, Guy O, et al. Hollow microneedles for ocular drug delivery. J Control Release 2024;371:43-66. [PMID: 38735395 DOI: 10.1016/j.jconrel.2024.05.013]
- Bao Q, Zhang X, Hao Z, Li Q, Wu F, et al. Advances in polysaccharide-based microneedle systems for the treatment of ocular diseases. Nanomicro Lett 2024;16(1):268. [PMID: 39136800 DOI: 10.1007/s40820-024-01477-3]
- Day R. Polysaccharides in ocular tissue. Am J Ophthalmol 1950;33(2):224-6. [PMID: 15405339 DOI: 10.1016/0002-9394(50)90840-3]
- Dou S, Wang Q, Zhang B, Wei C, Wang H, et al. Single-cell atlas of keratoconus corneas revealed aberrant transcriptional signatures and implicated mechanical stretch as a trigger for keratoconus pathogenesis. Cell Discov 2022;8(1):66. [PMID: 35821117 DOI: 10.1038/s41421-022-00397-z]
- Kim JW, Zhang P, Gehlbach P, Iordachita I, Kobilarov M. Micromanipulation in surgery: autonomous needle insertion inside the eye for targeted drug delivery. Arxiv preprint arxiv:2306.17421. 2023. [DOI: 10.48550/arXiv.2306.17421]
- Jiménez-Gómez Y, Alba-Molina D, Blanco-Blanco M, Pérez-Fajardo L, Reyes-Ortega F, et al. Novel treatments for age-related macular degeneration: a review of clinical advances in sustained drug delivery systems. Pharmaceutics 2022;14(7):1473. [PMID: 35890368 DOI: 10.3390/pharmaceutics14071473]
- Wu Y, Vora LK, Donnelly RF, Singh TRR. Rapidly dissolving bilayer microneedles enabling minimally invasive and efficient protein delivery to the posterior segment of the eye. Drug Deliv Transl Res 2023;13(8):2142-58. [PMID: 35713782 DOI: 10.1007/s13346-022-01190-x]
- Giri BR, Jakka D, Sandoval MA, Kulkarni VR, Bao Q. Advancements in ocular therapy: a review of emerging drug delivery approaches and pharmaceutical technologies. Pharmaceutics 2024;16(10):1325. [PMID: 39458654 DOI: 10.3390/pharmaceutics16101325]
- Arribada RG, Rodrigues-Braz D, Silva-Cunha A, Behar-Cohen F. Excipients in drug delivery systems: a comprehensive review of approved inactive ingredients for human ophthalmic formulations. Eur J Pharm Biopharm 2025;208:114637. [PMID: 39837427 DOI: 10.1016/j.ejpb.2025.114637]
- Zaki M, Pardo J, Carracedo G. A review of international medical device regulations: contact lenses and lens care solutions. Cont Lens Anterior Eye 2019;42(2):136-46. [PMID: 30446241 DOI: 10.1016/j.clae.2018.11.001]
- Olowe M, Parupelli SK, Desai S. A review of 3d-printing of microneedles. Pharmaceutics 2022;14(12):2693. [PMID: 36559187 DOI: 10.3390/pharmaceutics14122693]
- Alotaibi TA, Iyire A, Assaf S, Dahmash EZ. Development and characterization of niosomes loaded mucoadhesive biodegradable ocular inserts for extended release of pilocarpine HCL. Futur J Pharm Sci 2024;10(1):22. [DOI: 10.1186/s43094-024-00598-1]
- Anumolu SS, Singh Y, Gao D, Stein S, Sinko PJ. Design and evaluation of novel fast forming pilocarpine-loaded ocular hydrogels for sustained pharmacological response. J Control Release 2009;137(2):152-9. [PMID: 19341773 DOI: 10.1016/j.jconrel.2009.03.016]
- Rathore KS, Nema RK, Sisodia SS. Timolol maleate a gold standard drug in glaucoma used as ocular films and inserts: an overview. Int J Pharm Sci Rev Res 2010;3(1):23-9.
- Lee A, Blair HA. Dexamethasone intracanalicular insert: a review in treating post-surgical ocular pain and inflammation. Drugs 2020;80(11):1101-8. [PMID: 32588339 DOI: 10.1007/s40265-020-01344-6]
- Campochiaro PA, Hafiz G, Shah SM, Bloom S, Brown DM, et al. Sustained ocular delivery of fluocinolone acetonide by an intravitreal insert. Ophthalmology 2010;117(7):1393-9. [PMID: 20202684 DOI: 10.1016/j.ophtha.2009.11.024]
- Ara T, Sharma S, Bhat SA, Bhandari A, Deva AS, et al. Preparation and evaluation of ocular inserts of diclofenac sodium for controlled drug delivery. Der Pharm Lett 2014;6(6):93-9.
- Keny S, Sawaikar L. Sustained release of ciprofloxacin hydrochloride and loteprednol etabonate from ophthalmic ocuserts for treatment of bacterial conjunctivitis. Indian J Pharm Sci 2024;86(3):1-9. [DOI: 10.36468/pharmaceutical-sciences.1353]
- Mirzaeei S, Alizadeh M. Design and evaluation of soluble ocular insert for controlled release of chloramphenicol. J Rep Pharm Sci 2017;6(2):123-33. [DOI: 10.4103/2322-1232.222620]
- Alzahrani A, Youssef AAA, Nyavanandi D, Tripathi S, Bandari S, et al. Design and optimization of ciprofloxacin hydrochloride biodegradable 3D printed ocular inserts: full factorial design and in-vitro and ex-vivo evaluations: part II. Int J Pharm 2023;631:122533. [PMID: 36566827 DOI: 10.1016/j.ijpharm.2022.122533]
- Aburahma MH, Mahmoud AA. Biodegradable ocular inserts for sustained delivery of brimonidine tartarate: preparation and in vitro/in vivo evaluation. AAPS PharmSciTech 2011;12(4):1335-47. [PMID: 21979886 DOI: 10.1208/s12249-011-9701-3]
- Shadambikar G, Marathe S, Patil A, Joshi R, Bandari S, et al. Novel application of hot melt extrusion technology for preparation and evaluation of valacyclovir hydrochloride ocular inserts. AAPS PharmSciTech 2021;22(1):1-7. [PMID: 33447869 DOI: 10.1208/s12249-020-01916-5]
- Karnik I, Youssef AA, Joshi P, Munnangi SR, Narala S, et al. Formulation development and characterization of dual drug loaded hot-melt extruded inserts for better ocular therapeutic outcomes: sulfacetamide/prednisolone. J Drug Deliv Sci Technol 2023;84:104558. [DOI: 10.1016/j.jddst.2023.104558]
- Jethava JK, Jethava GK. Design, formulation, and evaluation of novel sustain release bioadhesive in-situ gelling ocular inserts of ketorolac tromethamine. Int J Pharm Investig 2014;4(4):226. [PMID: 25426444 DOI: 10.4103/2230-973X.143131]
- Koradia K, Dedakia A, Koradia H. Development and in vitro-in vivo evaluation of ocular insert containing ketorolac tromethamine and moxifloxacin hydrochloride. Ann Pharm Fr 2025;83(1):163-172. [PMID: 39413968 DOI: 10.1016/j.pharma.2024.10.002]
- Duman G, Yildir I, Macit M, Genç E, Sümer E, et al. Development and evaluation of 3D-printed ocular insert containing liposomal moxifloxacin. J Drug Deliv Sci Technol 2024;92:105353. [DOI: 10.1016/j.jddst.2024.105353]
- Pandey P, Panwar AS, Dwivedi P, Jain P, Agrawal A, et al. Design and evaluation of ocular inserts for controlled drug delivery of acyclovir. Int J Pharm Biol Arch 2011;2(4):1106-10.
- Hady MA, El-Zahaby SA. Phospholipid free nano-vesicles of brinzolamide biopolymer ocular insert; design, in vitro and in vivo evaluation. J Pharm Sci 2024;113(8):2178-87. [PMID: 38428457 DOI: 10.1016/j.xphs.2024.02.021]
- Rubião F, Araújo ACF, Sancio JB, Nogueira BS, Franca JR, et al. Topical bimatoprost insert for primary open-angle glaucoma and ocular hypertension treatment–a phase II controlled study. Curr Drug Deliv 2021;18(7):1022-6. [PMID: 33388018 DOI: 10.2174/1567201818666210101112256]
- Dayoub RA, Laham A. Preparation and in-vitro evaluation of timolol maleate loaded ocular inserts by using various polymers. Res J Pharm Technol 2023;16(3):1259-66. [DOI: 10.52711/0974-360x.2023.00208]
- Terreni E, Chetoni P, Burgalassi S, Tampucci S, Zucchetti E, et al. A hybrid ocular delivery system of cyclosporine—a comprising nanomicelle-laden polymeric inserts with improved efficacy and tolerability. Biomater Sci 2021;9(24):8235-48. [DOI: 10.1039/d1bm01453f]
- Terreni E, Burgalassi S, Chetoni P, Tampucci S, Zucchetti E, et al. Development and characterization of a novel peptide-loaded antimicrobial ocular insert. Biomolecules 2020;10(5):664. [PMID: 32344824 DOI: 10.3390/biom10050664]
- Harikumar SL, Balasubramaniam J, Kumar MT, Pandit J. In vitro characterization of physically reinforced ocular inserts of indomethacin. Acta Pharma Sci 2004;46(1).
- Franca JR, Foureaux G, Fuscaldi LL, Ribeiro TG, Castilho RO, et al. Chitosan/hydroxyethyl cellulose inserts for sustained-release of dorzolamide for glaucoma treatment: in vitro and in vivo evaluation. Int J Pharm 2019;570:118662. [PMID: 31491481 DOI: 10.1016/j.ijpharm.2019.118662]
- Saettone MF, Torracca MT, Pagano A, Giannaccini B, Rodriguez L, et al. Controlled release of pilocarpine from coated polymeric ophthalmic inserts prepared by extrusion. Int J Pharm 1992;86(2-3):159-66. [DOI: 10.1016/0378-5173(92)90193-6]
- Taghe S, Mirzaeei S, Alany RG, Nokhodchi A. Polymeric inserts containing Eudragit® l100 nanoparticle for improved ocular delivery of azithromycin. Biomedicines 2020;8(11):466. [PMID: 33142768 DOI: 10.3390/biomedicines8110466]
- Rao MV, Shyale S. Preparation and evaluation of ocular inserts containing norfloxacin. Turk J Med Sci 2004;34(4):239-46.
- Amar A, Ashish K, Ajaykumar P, Anand J. Formulation and evaluation of controlled release ocular inserts of betaxolol hydrochloride. IOSR J Pharm 2012;2(5):34-8. [DOI: 10.9790/3013-25203438]
- Omer S, Zelkó R. A systematic review of drug-loaded electrospun nanofiber-based ophthalmic inserts. Pharmaceutics 2021;13(10):1637. [PMID: 34683930 DOI: 10.3390/pharmaceutics13101637]
- Mirzaeei S, Barfar D. Design and development of antibacterial/anti-inflammatory dual drug-loaded nanofibrous inserts for ophthalmic sustained delivery of gentamicin and methylprednisolone: in vitro bioassay, solvent, and method effects’ evaluation. Adv Pharm Bull 2022;12(3):531-40. [PMID: 35935049 DOI: 10.34172/apb.2022.056]
- Km M, Kulkarni GT. Design, development and evaluation of controlled release levobunolol hydrochloride ocular inserts for glaucoma therapy. J Chronother Drug Deliv 2012;3:87-97.
- Souto EB, Dias-Ferreira J, López-Machado A, Ettcheto M, Cano A, et al. Advanced formulation approaches for ocular drug delivery: state-of-the-art and recent patents. Pharmaceutics 2019;11(9):460. [PMID: 31500106 DOI: 10.3390/pharmaceutics11090460]
- Mostafa M, Al Fatease A, Alany RG, Abdelkader H. Recent advances of ocular drug delivery systems: prominence of ocular implants for chronic eye diseases. Pharmaceutics 2023;15(6):1746. [PMID: 37376194 DOI: 10.3390/pharmaceutics15061746]
- https://patents.google.com/.
- Elliott W, Chan J. Eta?lcon a drug-eluting contact lens with ketotifen (acuvue theravision with ketotifen). Intern Med Alert 2022;44(10).
- Novack GD, Barnett M. Ocular drug delivery systems using contact lenses. J Ocul Pharmacol Ther 2020;36(8):595-601. [DOI: 10.1089/jop.2020.0024]
- Kompella UB, Kadam RS, Lee VH. Recent advances in ophthalmic drug delivery. Ther Deliv 2010;1(3):435-56. [PMID: 21399724 DOI: 10.4155/TDE.10.40]
- Gruber E. The state of contact lenses in the United States in the 1990s. Int Contact Lens Clin 1991;18(9-10):P175-7. [DOI: 10.1016/0892-8967(91)90003-I]
- Maulvi FA, Patil RJ, Desai AR, Shukla MR, Vaidya RJ, et al. Effect of gold nanoparticles on timolol uptake and its release kinetics from contact lenses: in vitro and in vivo evaluation. Acta Biomater 2019;86:350-62. [PMID: 30625414 DOI: 10.1016/j.actbio.2019.01.004]
- Yañez F, Martikainen L, Braga ME, Alvarez-Lorenzo C, Concheiro A, et al. Supercritical fluid-assisted preparation of imprinted contact lenses for drug delivery. Acta Biomater 2011;7(3):1019-30. [PMID: 20934541 DOI: 10.1016/j.actbio.2010.10.003]
- Bin Sahadan MY, Tong WY, Tan WN, Leong CR, Bin Misri MN, et al. Phomopsidione nanoparticles coated contact lenses reduce microbial keratitis causing pathogens. Exp Eye Res 2019;178:10-4. [PMID: 30243569 DOI: 10.1016/j.exer.2018.09.011]
- Tripathi S, Yadav KS. Development of brimonidine niosomes laden contact lenses for extended release and promising delivery system in glaucoma treatment. Daru 2024;32(1):161-75. [PMID: 38158475 DOI: 10.1007/s40199-023-00500-z]
- Daull P, Garrigue JS, Liang H, Baudouin C. Use of a cationic emulsion of latanoprost to treat glaucoma patients with ocular surface disease: a preclinical review. J Ocul Pharmacol Ther 2023;39(4):240-51. [PMID: 37015075 DOI: 10.1089/jop.2022.0155]
- Michałkiewicz O, Nowak I, Nowak R, Rykowska I. Daily dispos-able contact lenses as a platform for ocular drug delivery of cyclo-sporine A. Physicochem Probl Miner Process 2023;59(4):172794. [DOI: 10.37190/ppmp/172794]
- Vivero-Lopez M, Muras A, Silva D, Serro AP, Otero A, et al. Resveratrol-loaded hydrogel contact lenses with antioxidant and antibiofilm performance. Pharmaceutics 2021;13(4):532. [PMID: 33920327 DOI: 10.3390/pharmaceutics13040532]
- Salz JJ, Reader AL 3rd, Schwartz LJ, Van Le K. Treatment of corneal abrasions with soft contact lenses and topical diclofenac. J Refract Surg 1994;10(6):640-6. [PMID: 7719534 DOI: 10.3928/1081-597X-19941101-09]
- Ucar F, Kadioglu E. Effectiveness of ketorolac-soaked bandage contact lens for pain management after photorefractive keratectomy. Cutan Ocul Toxicol 2023;42(2):55-60. [PMID: 37042853 DOI: 10.1080/15569527.2023.2201832]
- Karlgard CC, Jones LW, Moresoli C. Ciprofloxacin interaction with silicon-based and conventional hydrogel contact lenses. Eye Contact Lens 2003;29(2):83-9. [PMID: 12695709 DOI: 10.1097/01.ICL.0000061756.66151.1C]
- Hyatt AJ, Rajan MS, Burling K, Ellington MJ, Tassoni A, et al. Release of vancomycin and gentamicin from a contact lens versus a fibrin coating applied to a contact lens. Invest Ophthalmol Vis Sci 2012;53(4):1946-52. [PMID: 22408014 DOI: 10.1167/iovs.11-8607]
- Morgan SR, Pilia N, Hewitt M, Moses RL, Moseley R, et al. Controlled in vitro delivery of voriconazole and diclofenac to the cornea using contact lenses for the treatment of Acanthamoeba keratitis. Int J Pharm 2020;579:119102. [PMID: 32007592 DOI: 10.1016/j.ijpharm.2020.119102]
- Dave SB, Toma HS, Kim SJ. Changes in ocular flora in eyes exposed to ophthalmic antibiotics. Ophthalmology 2013;120(5):937-41. [PMID: 23415422 DOI: 10.1016/j.ophtha.2012.11.005]
- Ruben M, Watkins R. Pilocarpine dispensation for the soft hydrophilic contact lens. Br J Ophthalmol 1975;59(8):455-8. [PMID: 1203231 DOI: 10.1136/bjo.59.8.455]
- Xu B, Liu T. Travoprost loaded microemulsion soaked contact lenses: improved drug uptake, release kinetics and physical properties. J Drug Deliv Sci Technol 2020;57:101792. [DOI: 10.1016/j.jddst.2020.101792]
- Yan F, Liu Y, Han S, Zhao Q, Liu N. Retracted article: bimatoprost imprinted silicone contact lens to treat glaucoma. AAPS PharmSciTech 2020;21(2):63. [PMID: 31933030 DOI: 10.1208/s12249-020-1622-6]
- Malaekeh-Nikouei B, Vahabzadeh SA, Mohajeri SA. Preparation of a molecularly imprinted soft contact lens as a new ocular drug delivery system for dorzolamide. Curr Drug Deliv 2013;10(3):279-85. [PMID: 23360228 DOI: 10.2174/1567201811310030004]
- C De Guzman LM, De Guzman GQ, Borromeo EC. Brinzolamide-loaded soft contact lens for ophthalmic delivery. Ther Deliv 2022;13(4):233-47. [PMID: 35615865 DOI: 10.4155/tde-2022-0005]
- Razeghinejad MR, Sawchyn AK, Katz LJ. Fixed combinations of dorzolamide-timolol and brimonidine-timolol in the management of glaucoma. Expert Opin Pharmacother 2010;11(6):959-68. [PMID: 20307220 DOI: 10.1517/14656561003667540]
- Centofanti M, Oddone F, Gandolfi S, Hommer A, Boehm A, et al. Comparison of travoprost and bimatoprost plus timolol fixed combinations in open-angle glaucoma patients previously treated with latanoprost plus timolol fixed combination. Am J Ophthalmol 2010;150(4):575-80. [PMID: 20688314 DOI: 10.1016/j.ajo.2010.05.003]
- Strohmaier K, Snyder E, DuBiner H, Adamsons I; the Dorzolamide-Timolol Study Group. The efficacy and safety of the dorzolamide—timolol combination versus the concomitant administration of its components. Ophthalmology 1998;105(10):1936-44. [PMID: 9787367 DOI: 10.1016/s0161-6420(98)91045-4]
- Jiang J, Gill HS, Ghate D, McCarey BE, Patel SR, et al. Coated microneedles for drug delivery to the eye. Invest Ophthalmol Vis Sci 2007;48(9):4038-43. [PMID: 17724185 DOI: 10.1167/iovs.07-0066]
- Amer M, Chen RK. Hydrogel-forming microneedle arrays for sustained and controlled ocular drug delivery. J Eng Sci Med Diagn Ther 2020;3(4):041003. [DOI: 10.1115/1.4048481]
- Jiang J, Moore JS, Edelhauser HF, Prausnitz MR. Intrascleral drug delivery to the eye using hollow microneedles. Pharm Res 2009;26(2):395-403. [PMID: 18979189 DOI: 10.1007/s11095-008-9756-3]
- Mahadevan G, Sheardown H, Selvaganapathy P. PDMS embedded microneedles as a controlled release system for the eye. J Biomater Appl 2013;28(1):20-7. [PMID: 22262574 DOI: 10.1177/0885328211433778]
- Edelhauser HF, Verhoeven RS, Burke B, Struble CB, Patel SR. Intraocular distribution and targeting of triamcinolone acetonide suspension administered into the suprachoroidal space. Invest Ophthalmol Vis Sci 2014;55(13):5259.
- Chiang B, Kim YC, Edelhauser HF, Prausnitz MR. Circumferential flow of particles in the suprachoroidal space is impeded by the posterior ciliary arteries. Exp Eye Res 2016;145:424-31. [PMID: 26976663 DOI: 10.1016/j.exer.2016.03.008]
- Hosoya K-I, Tachikawa M. The inner blood-retinal barrier: molecular structure and transport biology. In: Cheng CY, editor. Biology and regulation of blood-tissue barriers. Advances in experimental medicine and biology, Vol 763. New York, NY: Springer; 2013. pp. 85-104. [DOI: 10.1007/978-1-4614-4711-5_4]
- Gu B, Liu J, Li X, Ma Q, Shen M, et al. Real-time monitoring of suprachoroidal space (SCS) following SCS injection using ultra-high resolution optical coherence tomography in guinea pig eyes. Invest Ophthalmol Vis Sci 2015;56(6):3623-34. [PMID: 26047049 DOI: 10.1167/iovs.15-16597]
- Chiang B, Kim YC, Doty AC, Grossniklaus HE, Schwendeman SP, et al. Sustained reduction of intraocular pressure by supraciliary delivery of brimonidine-loaded poly(lactic acid) microspheres for the treatment of glaucoma. J Control Release 2016;228:48-57. [PMID: 26930266 DOI: 10.1016/j.jconrel.2016.02.041]
- Ciulla T, Yeh S. Microinjection via the suprachoroidal space: a review of a novel mode of administration. Am J Manag Care 2022;28(suppl 13):S243-52. [PMID: 36395492 DOI: 10.37765/ajmc.2022.89270]
- Kim YC, Edelhauser HF, Prausnitz MR. Targeted delivery of antiglaucoma drugs to the supraciliary space using microneedles. Invest Ophthalmol Vis Sci 2014;55(11):7387-97. [PMID: 25212782 DOI: 10.1167/iovs.14-14651]
- Wang H, Xu J, Xiang L. Microneedle-mediated transcutaneous immunization: potential in nucleic acid vaccination. Adv Healthc Mater 2023;12(23):e2300339. [PMID: 37115817 DOI: 10.1002/adhm.202300339]
- Jiang X, Jin Y, Zeng Y, Shi P, Li W. Self-implantable core–shell microneedle patch for long-acting treatment of keratitis via programmed drug release. Small 2024;20(29):2310461. [DOI: 10.1002/smll.202310461]