Advances in Drug Delivery Systems for Osteochondral Tissue Regeneration
1Department of Orthopedics, Seventh Affiliated Hospital of Shanxi Medical University, Linfen People’s Hospital, Linfen, Shanxi 041000, China
2Institute of Orthopaedic & Musculoskeletal Science, Division of Surgery and Interventional Science, University College London, Royal National Orthopaedic Hospital, London HA7 4LP, UK
3College of Chemistry and Life Science, Beijing University of Technology, Beijing 100124, China
4Yongji Disease Control and Prevention Centre, Yongji, Shanxi 044599, China
aThese authors contributed equally to this work.
*Correspondence to: Yaning Zhang, Department of Orthopaedics, Seventh Affiliated Hospital of Shanxi Medical University, Linfen People’s Hospital, Linfen, Shanxi 041000, China. E-mail: zhangyn1965@126.com; Chaozong Liu, Centre for Bioengineering & Surgical Technology, Institute of Orthopaedic & Musculoskeletal Science, University College London, Royal National Orthopaedic Hospital, Stanmore HA7 4LP, UK. E-mail: chaozong.liu@ucl.ac.uk; Bin Li, Department of Orthopaedics, Seventh Affiliated Hospital of Shanxi Medical University, Linfen People’s Hospital, Linfen, Shanxi 041000, China. E-mail: lf09887@126.com
Received: April 20 2025; Revised: June 26 2025; Accepted: July 6 2025; Published Online: July 30 2025
Cite this paper:
Shang J, Zhang J, Liu L et al. Advances in Drug Delivery Systems for Osteochondral Tissue Regeneration. BIO Integration 2025; 6: 1–28.
DOI: 10.15212/bioi-2025-0072. Available at: https://bio-integration.org/
Download citation
© 2025 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
Osteochondral damage is primarily caused by degeneration of articular cartilage due to trauma, degenerative injury. Current approaches to treating cartilage damage typically involve medications, physical therapy, interventional therapy, and surgery. Drug delivery to the cartilage has shown promise in cartilage regeneration and slowing the progression of cartilage degeneration. However, the unique physiologic composition of articular cartilage poses challenges for effective drug delivery. Systemic administration of drugs may lead to inadequate drug distribution within the cartilage. Direct intra-articular injection of drugs can result in rapid clearance and limited retention time of the drug in the joint cavity. In summary, the limited duration of drug efficacy within the joint due to a short half-life and restricted diffusion through cartilage poses challenges for long-term drug therapy. Surgical intervention becomes necessary in cases of severe joint degeneration or ineffectiveness of alternative treatments. Various clinical studies have demonstrated the effectiveness of surgical approaches, such as an osteochondral autograft transplantation system (OATS), autologous chondrocyte implantation (ACI), and microfracture. Unfortunately, these interventions are also associated with potential adverse effects. The ongoing advances in biomaterials for osteochondral tissue regeneration and replacement have led to a growing interest in the utilization of biomaterial-based drug delivery systems for tissue regeneration. The integration of bioactive molecules, drugs, and genes with biomaterials presents a novel strategy for advancing osteochondral regeneration. A desirable drug delivery system should be able to penetrate cartilage tissue before the drug is cleared by synovial capillaries and lymphatic vessels, and bind to components of the cartilage extracellular matrix to reduce the physical deformation of cartilage during locomotion, resulting in a cartilage-specific drug pool. This paper was motivated by the great potential of biomaterials for osteochondral tissue regeneration and reviews recent progress in biomaterial-based drug delivery systems for osteochondral regeneration.
Keywords
bioactive molecules, delivery system, osteochondral regeneration, osteochondral unit.
Introduction
The connective tissue that covers the bony ends of human joints is termed as articular cartilage. The high-water content of articular cartilage helps lubricate the joint and absorb shocks and the collagen strands within articular cartilage provide strength and elasticity. Articular cartilage has the primary function of lubricating the joint and reducing stress during movement [1, 2].
When the osteochondral (OC) unit is damaged due to trauma, degenerative lesions, severe pain and restricted movement can occur. Young individuals might experience cartilage damage due to sports injuries, whereas older adults often have cartilage damage due to the natural deterioration of joints. Factors that increase the risk of cartilage damage include being overweight, a previous joint injury, and some genetic predispositions. The most prevalent type of cartilage damage is associated with osteoarthritis, which results in degenerative changes and breakdown of the articular cartilage [3]. Damage to cartilage can cause degeneration of joints, potentially leading to severe disabilities and significantly impacting patient well-being [3–5].
Classification of OC defects ranges from grade I, which is nearly normal, to grade IV, which indicates a severe abnormality. This grading system is based on the depth of the lesion and the components of the OC unit affected. Specifically, the grading system assesses whether the damage is limited to the cartilage or extends to the cartilage and subchondral bone, which comprise the entire OC unit [6]. It is difficult to regenerate cartilage tissue due to the special structure of cartilage and the lack of blood vessels and lymphatic vessels [7]. Currently, there are several treatment methods for OC repair, including drug therapy, physical therapy, and surgical intervention [8, 9]. Medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), can reduce inflammation and relieve pain. Physical therapy may also improve the strength and flexibility of the affected joint. However, surgical treatment is the last resort treatment option when the joint is severely diseased or does not respond to alternative treatments. Current surgical treatments for OC defects include chondroplasty, joint replacement, the OC autograft transplantation system (OATS), autologous chondrocyte implantation (ACI), and microfracture [10]. However, chondroplasty can only be palliative. While microfracture treatment can temporarily enhance joint function, microfracture treatment frequently result in the formation of fibrous tissue, weakening of the subchondral bone, and a decline the joint functionality over time [11, 12]. ACI involves performing a cartilage biopsy from patients at non-weight-bearing sites, isolating and expanding the chondrocytes in vitro, reimplanting the chondrocytes into the defect, and using periosteal flaps to maintain the implanted chondrocytes in situ. However, this procedure requires two surgical procedures, requires a prolonged recovery time, and frequently has complications due to flap hypertrophy [13]. Microfracture surgery remains a first-line intervention for small-to-medium cartilage defects, demonstrating significant short-term functional improvement and pain reduction within 6–12 months. Histologic studies have confirmed increased cartilage volume via fibrocartilage formation. However, Kreuz et al. reported the following critical long-term limitation: repaired tissue exhibits biomechanical inferiority, leading to progressive degeneration under physiologic loads [8]. This limitation manifests clinically as a functional decline in 68% of patients within 18–24 months postoperatively. Microfracture surgery offers cost-effective arthroscopic management of small-to-medium cartilage defects with low complication rates and rapid recovery. However, the long-term efficacy of microfracture surgery is limited. This approach is contraindicated for defects > 4 cm2 in size, obese patients (BMI > 30 kg/m2), or mal-aligned joints. The OATS remains the gold standard for defects ≤ 10 cm2 in size. The OATS restores hyaline cartilage (type II collagen > 90%) with superior integration strength, though the OATS requires open surgery and carries donor-site morbidity risks. The OATS is also recommended for patients with larger defects or significant joint degeneration [8, 9]. The OATS can improve the prognosis, including a reduction in pain and improvement in function. The OATS has a high long-term success rate and provides good mechanical strength. However, the OATS is an invasive surgical procedure that requires a second donor tissue surgical site. The OATS has a high risk of adverse events related to the donor site and a long recovery time. ACI can effectively repair cartilage defects, improve joint function, and can be used for large cartilage injuries. ACI can provide good mechanical strength and does not require a second surgical site. However, this process requires advanced technical skills, specialized equipment, and professional knowledge. The risk of complications related to the implantation process is high and recovery takes a relatively long time [14, 15]. In conclusion, OC regeneration is a major medical hurdle because of the diverse physiologic characteristics and inherent structures of cartilage and subchondral bone.
Improvements in OC regeneration have been achieved in recent years by combining biological components and biomaterials with suitable biomechanical characteristics and structures. Combining biological components and biomaterials provides a novel therapeutic strategy for restoring, maintaining, or improving the function of OC tissue. Combining biological elements with tissue engineering principles to combine different substrates, cells, and bioactive molecules as vehicles for drug and/or cellular delivery may open new prospects for OC regeneration. In this paper the biomaterial delivery systems developed in recent years have been reviewed to identify the key factors for the success of OC regeneration. Key factors for successful OC regeneration have been considered in this review, as follows: ⅰ) biological structure of osteochondral units; ⅱ) types and combinations of biomaterials; ⅲ) drug of choice; and ⅳ) commonly used delivery systems. Based on this careful analysis, promising directions for the treatment of OC regeneration, which remains one of the most formidable clinical problems in orthopedics and rheumatology, will be discussed.
Biological structure of OC units
The OC unit is a holistic functional entity consisting of articular cartilage, subchondral bone tissue, and osteochondral interfaces, as shown in Figure 1. The structural and functional properties of OC units vary.
Figure 1 Graphical illustration of an osteochondral unit structure. Graphical illustration of the zonal structure of chondrocytes, collagen, and the subchondral bone in the osteochondral unit of the knee joint. Please note that this diagrammatic drawing does not represent the actual dimensions. From top-to-bottom, the zones are the SZ-superficial (10–20%), MZ-middle (40–60%), and DZ-deep zones (30–40%).

Articular cartilage
Articular cartilage is situated on the joint surface and consists of hyaline cartilage, which is known for its elasticity and smooth surface. Articular cartilage acts as a buffer during joint movement and reduces friction between adjacent bones and transfers the mechanical load to subchondral bone [1]. Cartilage tissue has a low cellular density and primarily consists of chondrocytes, which accounts for approximately 2% of the total volume. Chondrocytes aggregate into “cell nests” or “homologous groups” and infiltrate the abundant extracellular matrix (ECM) [16, 17]. Chondrocytes have an essential role in joint stability. The hyaline cartilage ECM is organised into four distinct structural and biochemical regions (surface, middle, deep, and calcified regions), all of which contribute to viscoelastic properties [1]. The ECM is predominantly comprised of collagen (specifically, type II collagen) and proteoglycans with lesser quantities of adherens glycoproteins and elastin fibres [18]. Proteoglycans have a vital role in chondrocyte metabolism [19]. The invasion and differentiation of exogenous progenitor cells is unfavorable due to an extremely limited number of endogenous progenitor cells in articular cartilage and absence of blood vessels, nerves, and lymphatic vessels. Therefore, the innate self-healing ability of articular cartilage is limited [20]. In contrast to bone regeneration, cartilage regeneration poses significant challenges.
In summary, chondrocytes lack blood and have limited proliferative potential. Thus, joint damage caused by trauma or disease frequently requires exogenous interventions to stimulate regeneration [21, 22].
Subchondral bone
Subchondral bone tissue is composed of cortical bone with a dense surface and cancellous bone with distal loose connective tissue and has higher active metabolism than cortical bone [23]. Subchondral bone is well-vascularized and the vascular branches extend into areas of calcified cartilage, which allows for metabolic exchange at the interface between these two tissues and ensures an integrated response to chemical and mechanical stimuli [24]. Calcified cartilage allows for passage of small molecules and is crucial in facilitating biochemical communication between non-calcified cartilage and subchondral bone. The calcified cartilage layer is destroyed in the diseases state and numerous fine fissures within the articular cartilage extend into the subchondral bone. Subchondral bones have blood vessels that reach deep into cartilage [25]. Osteoblasts release chondrolytic substances, such as prostaglandins, leukotrienes, and various (TGF-β, BMP, IGF, and FGF) growth factors, during the remodeling of subchondral bone. These substances travel through microcracks and blood vessels from the bone to the cartilage, reaching the articular cartilage [26] and further leading to cartilage loss. Factors released by articular cartilage that promote inflammation and stimulate osteoclast activity may also contribute to deterioration of subchondral bone by enhancing bone remodeling processes [27].
OC interface
Currently, there is some knowledge regarding the OC interface, which refers to the mineralized region between hyaline cartilage and subchondral bone. This interface is comprised of a layer of calcified cartilage that maintains an efficient junction that is capable of transmitting compressive, tensile, and shear forces from viscoelastic articular cartilage to mineralised subchondral bone [28]. The OC interface is vital in maintaining the structural stability of the joint and inhibits abnormal mineral deposition, bone growth, and invasion of blood vessels from the underlying bone [29].
OC regeneration has become a major challenge due to the different structural composition, biochemistry, biomechanics, and biological characteristics of cartilage and subchondral bone [30]. However, conventional engineered tissue strategies cannot mimic natural microstructures biologically. To address these issues, a combination of biological elements and biomaterials that can act as scaffolds and drug delivery systems would serve as a promising strategy for repairing OC tissues.
Signaling pathways related to articular cartilage repair
Cartilage injury repair is regulated by multiple complex signaling pathways, including the transforming growth factor-beta (TGF-β), bone morphogenetic protein (BMP), fibroblast growth factor (FGF), hypoxia-inducible factor (HIF), winged (Wnt)/β-catenin, nuclear factor κB (NF-κB), mitogen-activated protein kinase (MAPK), and Hedgehog (HH) signaling cascades.
Growth factor (GF) class signal pathways
GF signaling molecules, including TGF-β, BMP, insulin-like growth factor (IGF), and FGF, regulate cellular metabolism and activity during cartilage injury and repair. Specifically, TGF-β stimulates chondrocyte proliferation and cartilage matrix synthesis, thereby promoting anabolism and cartilage defect repair. TGF-β maintains chondrocyte phenotypic stability and induces proteoglycan and type II collagen production through the Smad2/Smad3 pathway. Conversely, TGF-β promotes chondrocyte hypertrophy by stimulating collagen X, MMP-13, osteopontin, alkaline phosphatase, osteocalcin, and vascular endothelial GF expression via Smad1/Smad5/Smad8 signaling. BMP-7 stimulates ECM synthesis in chondrocytes, inhibits catabolic processes induced by interleukin (IL)-1, IL-6, and fibronectin, and promotes mesenchymal stem cell chondrogenesis [31, 32]. FGF-18 induces chondrocyte proliferation and upregulates SOX-9 (a member of the Sox gene family) via fibroblast growth factor receptor 3 (FGFR3) activation, which enhances type II collagen and ECM production [33], while promoting anabolism in human articular chondrocytes. FGF-2 primarily activates FGFR1, upregulates MMP-1 and MMP-13 expression, and enhances ADAMTS (a disintegrin and metalloproteinase with thrombospondin motifs) production. Notably, ADAMTS inhibits cartilage matrix formation [34] and promotes inflammatory cell infiltration. IGF-1 stimulates chondrocyte proliferation, promotes proteoglycan and type II collagen synthesis, induces mesenchymal stem cell chondrogenesis, and maintains chondrocyte phenotype stability.
Wnt/β-catenin pathway
The Wnt signaling pathway has a crucial role in regulating proliferation, differentiation, growth, and other cellular functions [35]. The canonical Wnt pathway primarily functions to inhibit cartilage formation and stimulate hypertrophic differentiation in chondrocytes. Specifically, Wnt1, Wnt4, and Wnt8a activate the β-catenin signaling pathway, thereby promoting chondrocyte hypertrophy and endochondral ossification. Inhibiting Wnt/β-catenin signaling alleviates osteoarthritis (OA) and enhances cartilage repair.
HIF pathway
Chondrocyte survival and functional maintenance depend on adaptive mechanisms mediated by HIF family members. In addition to hypoxia, key cartilage injury factors, including inflammatory cytokines (e.g., IL-1 and tumor necrosis factor-alpha [TNF-α]) and mechanical compression, also upregulate HIF expression. Studies have shown that HIF has a key role in cartilage injury and repair (specifically, hypoxic overexpression of HIF-1α). Hypoxic overexpression of HIF-1α stimulates chondrogenic differentiation of human bone marrow cells, promotes cartilage formation, and inhibits chondrocyte hypertrophy [36]. HIF-1α also enhances type II collagen and proteoglycan expression and facilitate cartilage matrix synthesis, thereby mitigating cartilage damage [37].
HH/smoothened (Smo) pathway
The HH protein family is comprised of Desert (DHH), Sonic (SHH), and Indian Hedgehog (IHH). Among these proteins, IHH signaling critically regulates cartilage formation and chondrocyte proliferation and differentiation in growth plates. Mechanistically, IHH binds its transmembrane receptor (Patched-1 [PTCH1]) and upregulates RUNX-2 expression, the master regulator of chondrocyte hypertrophy, thereby driving chondrocyte hypertrophic differentiation, maturation, endochondral ossification, and ultimately osteophyte formation [38].
MAPK pathway
The MAPK signaling pathway regulates essential processes in skeletal development, including cartilage formation, maturation, and endochondral ossification. Dysregulation of MAPK subfamilies, particularly p38 and ERK, have a critical role in chondrocyte dysfunction during OA pathogenesis and progression. Studies have shown that blocking the P38 signaling pathway can inhibit chondrocyte apoptosis in OA cartilage, reduce the expression of inflammatory cytokines (IL-1β, IL-6, and TNF-α), and delay cartilage injury [39].
NF-κB pathway
NF-κB transcription factors are ubiquitously expressed regulators of inflammation. The NF-κB pathway is activated by multiple stimuli, including fibronectin fragments, pro-inflammatory cytokines (e.g., TNF-α and IL-1β), mechanical stress, and matrix degradation products during cartilage injury. Activated NF-κB, either independently or through crosstalk with pathways (AMPK and Wnt), suppresses chondrocyte anabolism and stimulates catabolic enzyme secretion. This cascade ultimately drives articular cartilage destruction [40].
Biomaterials for OC tissue repair and regeneration
A variety of biocompatible materials are currently used in the regeneration of OC tissue, as detailed in Figure 2. These biocompatible materials include natural, synthetic, metallic, and inorganic polymers [41]. These substances can be crafted into various forms, such as microparticles, nanoparticles, hydrogels, porous matrices, fibres, and combinations of these materials, to facilitate the delivery of therapeutic drugs.
Figure 2 Biomaterials used in osteochondral regeneration mainly included natural polymers, synthetic polymers, and bioceramics.
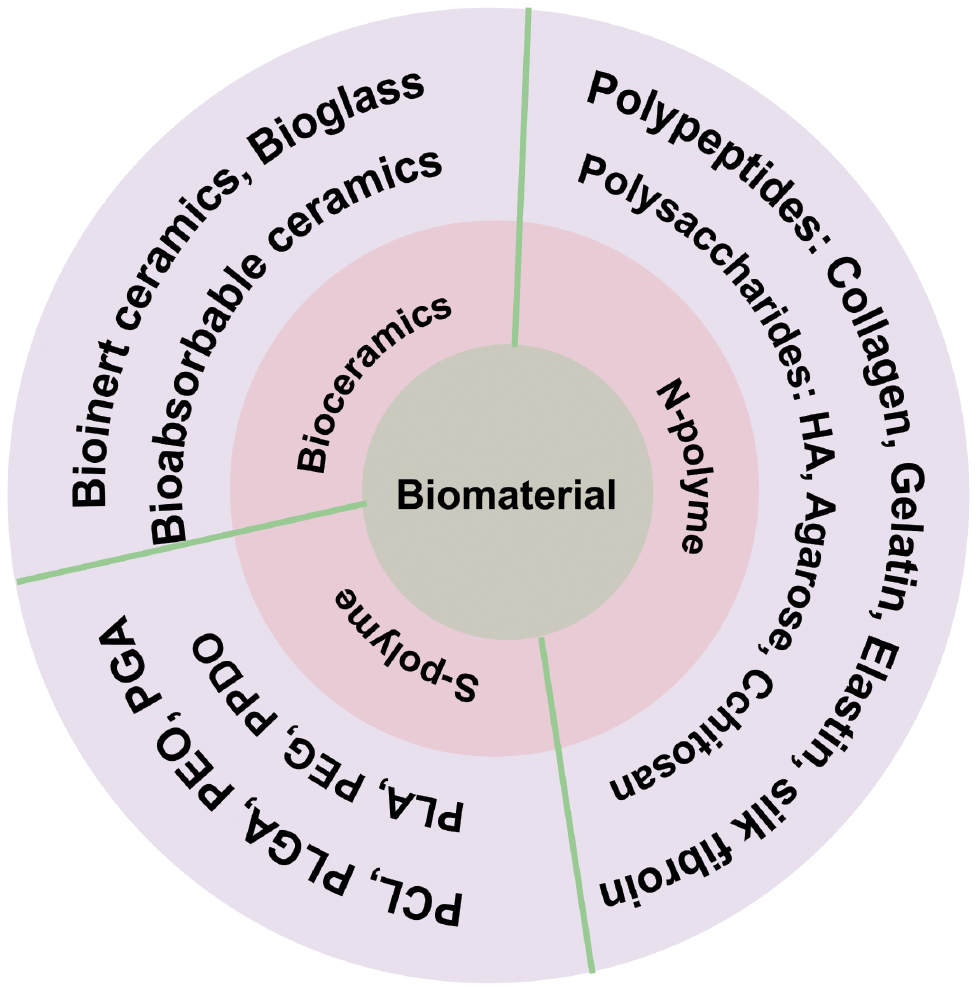
Polymeric materials are widely utilised to regulate and maintain the release of biological elements, such as bioactive molecules, cells, and genes, that will improve and speed up regeneration of functional bone and/or chondrocytes [42, 43]. Polymer materials are divided into natural and synthetic polymers according to the source. Natural polymers are biocompatible, biodegradable, and bionic and have abundant side groups. Natural polymers are structurally like the ECM and are important in OC regeneration [44, 45]. However, natural polymers have potential immunogenicity and uncontrollable degradation rates [44, 46]. In contrast, synthetic polymers have overcome the above problems and have the advantages of easy fabrication and adjustable physicochemical and mechanical properties [46]. Nevertheless, the primary issues related to synthetic polymers include inadequate cell adhesion as well as possible inflammatory responses caused by acidic degradation byproducts [45, 47].
Natural polymers
A variety of natural polymers have been used for OC regeneration, including polysaccharides (such as hyaluronic acid [HA] [48, 49], alginate [50, 51], agarose [52, 53], chitosan (CS) [54–56], cellulose derivatives [57]) and proteins (such as collagen [58], gelatin [59, 60], silk fibroin (SF) [61], and fibrin [62]). Natural polymers can facilitate cell interaction, synthesis, and development in tissues due to molecular domains. Collagen, for example, contains the RGD (arginine-Gly-aspartic acid) sequence, which provides extracellular microenvironment signaling that enhances the regenerative process of progenitor cell attachment, migration, proliferation, and differentiation [63]. Gelatin, a derivative of collagen, is a popular natural polymer due to good biodegradability, biocompatibility, biosafety, and cost-effectiveness. Gelatin-based carriers can be used for controlled and continuous delivery of biomolecules to promote the regenerative processes of attachment, migration, proliferation, and differentiation of mesenchymal stem cells (MSCs) [64]. CS polymers share structural similarities with two major cartilage molecules (HA and glycosaminoglycan molecules), which have successfully achieved subchondral bone and cartilage regeneration [65, 66]. Silk polymers obtained from silkworm cocoons or spider silk are also widely used for OC tissue regeneration [67]. Silk polymers can be mixed with synthetic polymers to enhance mechanical stability and make synthetic polymers easier to customize and process [68]. The mechanical properties of silk fibroin combined with nano-CaP are better than pure silk fibroin alone [69].
Synthetic polymers
At present, the commonly used synthetic polymers in OC tissue regeneration include polycaprolactone (PCL), polylactic acid-glycolic acid (PLGA), polyethene oxide (PEO), polyglycolic acid, polylactic acid (PLA), polyethylene glycol (PEG), polylcyclohexanone, and polypropyl fumarate [41, 70]. These polymers are hydrophobic and have rigidity, elasticity and porosity [71], which can be manipulated to achieve appropriate mechanical behaviour based on the properties of the material. Hydrophilicity can be improved by mixing hydrophobic and hydrophilic polymers, which facilitate cell fixation [41, 72, 73]. As mentioned earlier, the main advantages of using synthetic polymers are complete control of the structure and better mechanical properties. Synthetic polymers are also free of disease transmission or polymer supply constraints. However, biocompatibility can become a major concern when matrices made from synthetic polymers are used. In addition, synthetic polymers are prone to degradation and promote inflammation. PLA and PLGA offer the benefit of prolonged release of encapsulated substances over an extended duration. Nevertheless, generation of acidic degradation byproducts causes an inflammatory tissue reaction and leads to denaturation of bioactive factors. Therefore, synthetic polymers have been combined with natural polymers as delivery systems to achieve better biocompatibility [74, 75]. Neutralization between chitosan and PLGA degradation products could be achieved by wrapping chitosan/PLGA microspheres on the surface of BMP-2 [76]. Some studies have shown that PLLA can promote chondrocyte differentiation when combined with natural polymers, such as chitosan and silk, suggesting that delivery systems combining natural and artificial polymers have superior ability to promote OC regeneration [77, 78].
Metal materials
Titanium, titanium alloy, cobalt-chromium alloy, and stainless steel are commonly used metal materials in orthopedics. Metallic materials are characterized by excellent mechanical properties and biological inertness. Titanium and titanium alloys are the predominant metallic materials utilized in orthopedic application due to excellent compatibility and integration with bone tissue [79, 80]. By the mid-1980s, the focus of research on metallic materials began to shift from inert to bioactive and biodegradability. In recent years, magnesium-, strontium-, and zinc-based alloys have been successfully applied to orthopedic implants due to excellent mechanical properties and good bioactivity and biodegradability [81–84]. The combination of metallic materials and bioceramics, such as calcium phosphate, tricalcium phosphate (TCP), and HA, can enhance mechanical properties and promote bone mineralization, further aiding the fixation of implants with subchondral bone [85]. However, metallic materials are limited by inappropriate degradation rates, corrosion, and release of wear particles.
Inorganic materials
Bioceramics and bioapatites in bone have similar physicochemical properties and therefore have similar properties in terms of biodegradability, osteoconductivity, and osteoinducibility. Bioceramics promote bone regeneration by solubilizing and reprecipitating and combining with other ions in the tissue microenvironment to form carbonate apatite, which induces protein adsorption and enables cell attachment and differentiation [86]. Because TCP is more soluble than hydroxyapatite (HAP), the ratio of TCP-to-HAP can be adjusted to adjust the absorption rate of the material and match the rate of bone formation in biphasic biocrystals [41, 71, 87]. Bioceramics include bioinert ceramics, bioabsorbable ceramics, and bioactive glasses. Bioinert ceramics, like alumina and zirconia, can provide sufficient mechanical strength for the regeneration of subchondral bone but bioinert ceramics lack substantial biological interactions with the surrounding tissue. Bioresorbable ceramics, including calcium phosphate, calcium carbonate, calcium phosphate cements, and calcium silicate, can be gradually absorbed and replaced by new bone tissue in vivo [86]. Bioactive glasses (BGs), including silicate, phosphate, or borate based glasses, can be directly combined with surrounding tissues to form adhesive osteogenesis [88]. The excellent bioactivity of BGs can be attributed to the following: i) the interaction between collagen fibres in the vicinity and bone surface, which makes the collagen fibres tightly bound to the bone; and ii) the gradual dissolution and re-precipitation in physiologic fluids result in the formation of hydroxycarbonate apatites, which endow hydroxycarbonate apatites with bone conduction properties [89, 90]. The release of ions, especially cations, is also of great significance for OC regeneration. For example, incorporation of Cu2+ into BG scaffolds greatly enhance cartilage regeneration and OC interface repair, induce the transformation of macrophages to an anti-inflammatory phenotype, and suppress the inflammatory response of OC tissue [91]. BGs are frequently utilized in bone tissue engineering. BGs are resistant to chemical corrosion and wear, which can stimulate bone tissue formation [92–94].
In addition, bioceramics are easy to produce, inexpensive, and safe, making bioceramics widely used. In fact, bioceramics have been used in up to 53% of material applications for subchondral bone regeneration. However, bioceramics also have drawbacks, including limited flexibility, a high tendency to break, excessive rigidity, and inadequate resistance to fractures. Therefore, the development of biomaterials that combine the advantages of bioactive ceramics with polymers to obtain more ductile, tractable, and controllable properties, including stiffness, fracture toughness, porosity, and surface topography, for OC regeneration is a new research direction. For example, the combination of natural and synthetic polymers, such as gelatin, collagen, silk fibroin-based hydrogels and PLA with bioceramics, has resulted in improved mechanical properties and better osteoinduction [95]. Advances in this area have important implications for OC regeneration because improved healing of the subchondral bone leads to better results in cartilage repair.
Analysis of clinical settings
Natural polymers offer significant advantages as drug delivery carriers, including high biocompatibility, biodegradability, and low immunogenicity. These materials enhance cell migration, proliferation, and differentiation, while the specific molecular domains provide structural and functional guidance for cells at various developmental stages. However, natural polymers typically exhibit poor mechanical strength, low stiffness, and higher production costs [96]. Synthetic polymers offer superior mechanical strength, enhanced elasticity, low cytotoxicity, and tunable degradation kinetics compared to natural polymers. The design flexibility enables fabrication into patient-specific architectures with tailored porosity and dimensions that accommodate cell migration dynamics and tissue regeneration requirements [97, 98]. Furthermore, significant advances in electrospinning and 3D printing technologies have enabled faster fabrication of polymer-based carriers. Despite these manufacturing advantages, the inherent lack of biological activity limits interactions with host tissues. Such carriers typically exhibit hydrophobic surfaces that impair cell adhesion and proliferation. To address this finding, researchers have enhanced hydrophilicity and introduced bioactive structures through polymer surface functionalization, especially using plasma coating techniques.
Metal materials are particularly suitable for orthopedic implants addressing subchondral bone defects due to the high load-bearing capacity. However, the non-biodegradability and potential for wear particle generation restrict broader clinical applications. Recent studies have revealed that magnesium and magnesium alloys offer promising alternatives, combining excellent biodegradability and biocompatibility with osteogenic properties. Nevertheless, rapid degradation in the early post-implantation phase compromises mechanical integrity, which hinders utility [99, 100].
Ceramics exhibit high hardness, excellent wear resistance, and favorable biocompatibility. Ceramic implants generate significantly fewer wear particles compared to metallic and polymer-based implants. Nanoceramic composites feature smaller grain sizes than microceramics, enhancing the overall mechanical performance, tribological behavior, and biological functionality in vivo. Bioinert ceramics offer advantages, including support for tissue regeneration, biocompatibility, and improved mechanical strength. However, bioinert ceramics have unstable crack propagation, hydrothermal aging, and high manufacturing costs. Conversely, bioactive ceramics promote direct bone bonding (osteoconduction) and demonstrate high chemical stability but the inherent brittleness and complex processing limit clinical adoption. The advantages and disadvantages of the biomaterials are summarized in Table 1.
Table 1 Common biomaterial types used in osteochondral repair and regeneration: advantages and drawbacks
| Type | Name | Advantages | Drawbacks |
|---|---|---|---|
| Natural polymer | HA | Chemically modifiable, natural GAG in cartilage matrix | Low mechanical strength, requires modification to form 3D structures |
| Alginate | Cytocompatibility and regulated gelation | Low mechanical stability | |
| Chitosan | Biocompatible, non-cytotoxic, contains cartilage components | Slow gelation for in situ applications | |
| Collagen | Excellent biocompatibility, bioresorbable, and natural component of ECM; already used clinically | Immunogenic, poor mechanical strength, expensive | |
| Fibrin | Excellent mechanical properties and high versatility | High shrinking ability, increased degradation rate, and less mechanical stability | |
| Synthetic polymers | PLA | Easily processed, elongated degradation, high strength | Acidic byproducts, auto-catalytic degradation |
| PLGA | Selectable degradation based on co-polymer ratio | Acidic byproducts, poor long-term stability | |
| PEG | Easily functionalized | Non-degradability, no inherent biologic impact | |
| PCL | Great mechanical strength, elasticity | Hydrophobicity, slow degradation, intracellular resorption | |
| Metal Materials | Titanium and its alloys | Excellent mechanical properties, biological inertia | Non-degradability, tiredness, ion leakage, and infection risk |
| Magnesium/strontium/zinc-based alloys | Excellent mechanical properties, good biological activity, biodegradability | Inappropriate degradation rate, corrosion, release of wear particles | |
| Inorganic materials | Bioceramics | Promote bone regeneration and control biodegradation | Fragile, do not resist mechanical stresses |
HA: hyaluronic acid; PLA: polylactic acid; PLGA: poly (lactic-co-glycolic acid); PEG: polyethylene glycol; PCL: polycaprolactone.
Biological cues for OC tissue regeneration drugs
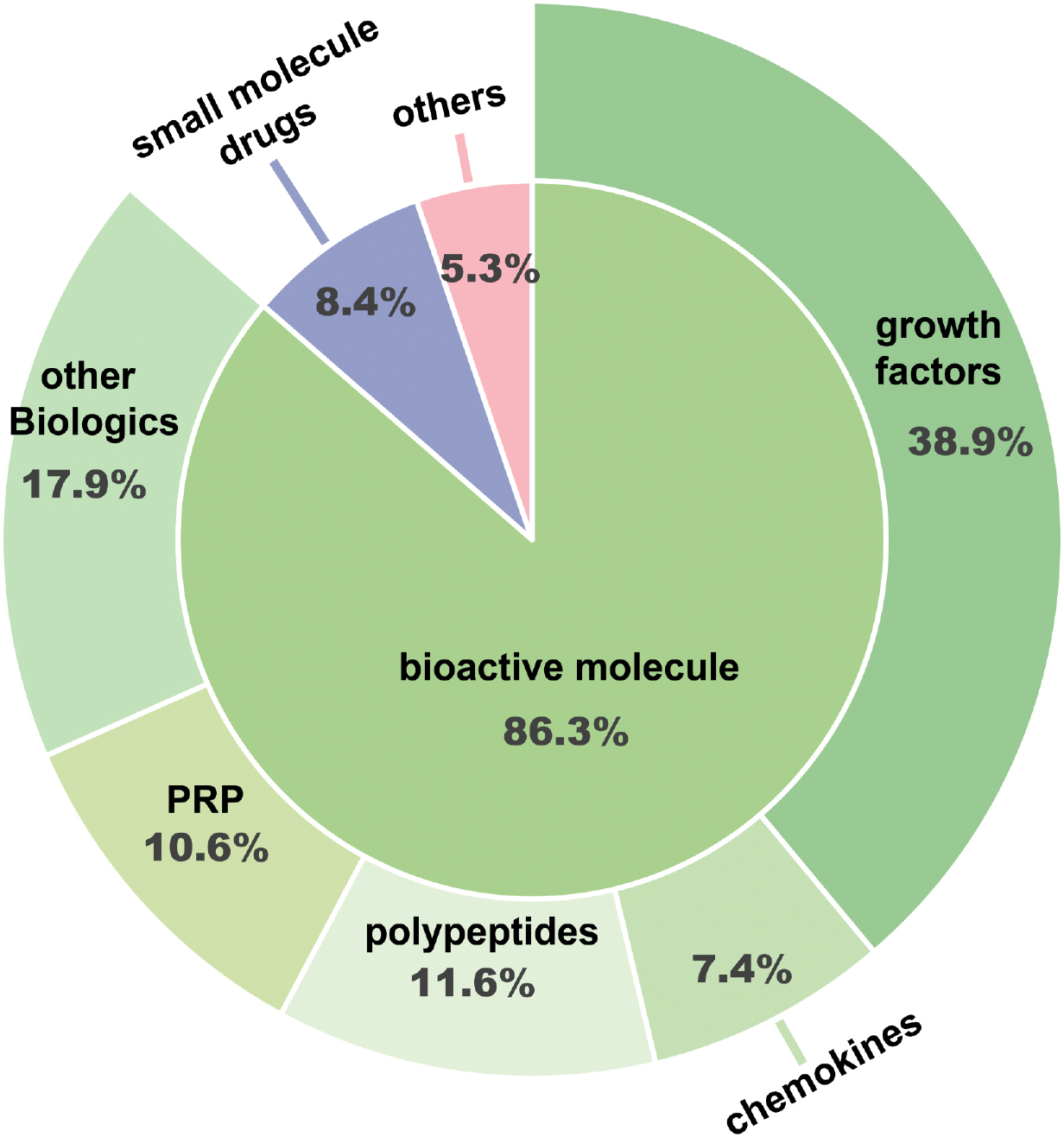
In recent years the therapeutic strategy of combining drugs with biomaterials has received extensive attention in addition to the necessary surgical treatment. These drugs mainly include a series of bioactive molecules, small molecule drugs, and other drugs, as shown in Figure 3.
Figure 3 Drugs used to promote osteochondral regeneration are mainly bioactive molecules, small molecule drugs, and other types of drugs. Among the bioactive molecules wer growth factors (GFs), platelet-rich plasma (PRP), chemokines, peptides, and other types of biological agents (the systems reported since 2015).
GFs
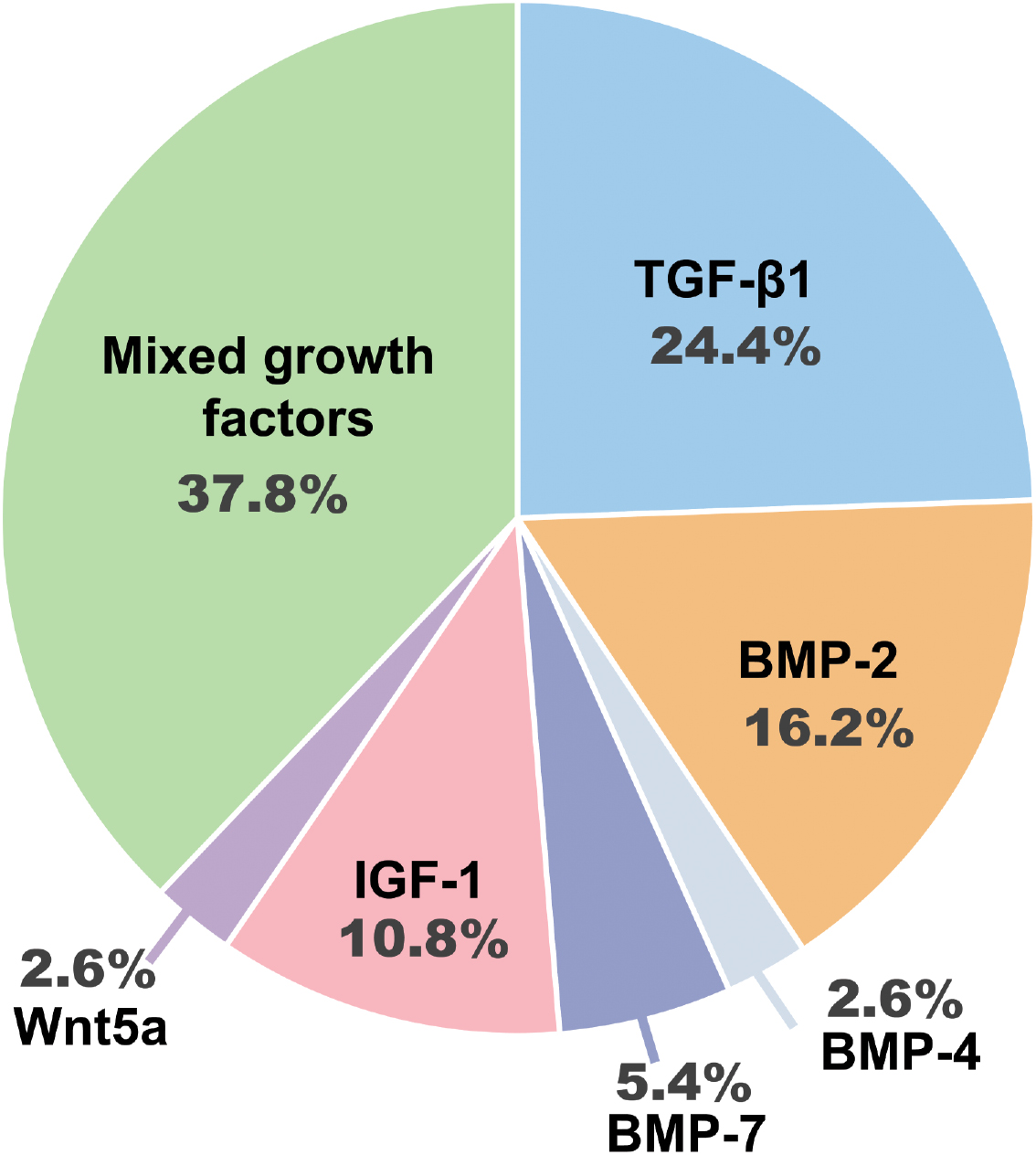
GFs promote the regeneration of new tissues by regulating the synthesis of cellular proteins and interacting with specific transmembrane receptors. GFs stimulate cellular signaling pathways that trigger cell differentiation, growth, proliferation, adhesion, survival, and migration upon binding to GF receptors. A variety of GFs have been used for OC tissue regeneration, as shown in Figure 4. GFs accelerate healing and regeneration of OC tissue through various methods, such as regulation of metalloproteinases and inflammatory markers, recruiting cells, and remodeling and synthesizing the ECM. In particular, the TGF-β superfamily members have a key role in the development of bone and cartilage [101]. TGF-β1 and TGF-β3 have been shown to have effects on cell proliferation and differentiation into osteoblasts or chondrocytes that depend on timing, dosage, and environmental factors [102]. Expression of TGF-β, especially TGF-β1 and TGF-β3, is significantly increased in injured chondrocytes and the efficiency of TGF-β signaling decreases with age [103]. Activated TGF-β1 and TGF-β3 can effectively stimulate the synthesis of aggrecan and type II collagen in chondrocytes and can induce MSCs to differentiate into chondroblasts in vitro. TGF-β1 can induce MSCs to differentiate into ectopic cartilage to repair cartilage defects in vivo [104]. BMPs are members of the TGF-β superfamily of secreted ligands. BMPs can induce the differentiation of MSCs into chondrocytes and osteoblasts and have an important role in the development and formation of bone and cartilage [105]. Specifically, BMP-2, -4, and -7 have been used clinically for bone regeneration. For example, the combined administration of BMP-7/BMP-2 improved healing in a rabbit cartilage injury model. BMP-4-expressing myogenic stem cells enhance chondrogenesis and significantly improved articular cartilage repair in a rat model [104].
Figure 4 Analysis of growth factors for osteochondral regeneration, including transforming growth factor-β1 (TGF-β1), bone morphogenetic protein (BMP)-2, -4, and -7, insulin-like growth factor-1 (IGF-1), wingless family member 5a (Wnt5a), mixed growth factors, or other types of growth factors (the systems reported since 2015) [214].
TGF-β and BMPs act on a tetrameric receptor complex consisting of two TGF-β type I receptors (TβRI/ALK5) and two type II kinase receptors (TβRII). The tetrameric receptor complex regulates mesenchymal stem cell (MSC) differentiation during bone development, bone formation, and bone homeostasis by regulating classical Smad-dependent (TGF-β/BMP ligands, receptors, and Smads) and non-classical Smad-dependent signaling pathways (p38 mitogen-activated protein kinase/p38 MAPK) [106]. In addition to a role in bone development, TGF-β and BMPs regulate postnatal bone and cartilage maintenance. TGF-βs have an important role in bone construction by osteoblasts and bone destruction by osteoclasts through osteoclast-mediated ATP6I-specific extracellular acidification [107] and cathepsin K-specific ECM proteins [108].
IGF-1 and BMP-2 have been encapsulated within gelatin microparticles and incorporated into a high molecular oligomer [poly (ethylene glycol) fumarate] (OPF) hydrogel matrix with precise spatial distribution. The OPF hydrogel matric promotes subchondral bone formation in a rabbit model of OC injury. Although these dual delivery systems do not improve cartilage repair, the dual delivery systems do show the potential of spatially-directed, multiple GF delivery vehicles for OC tissue repair [109]. Kim et al. [110] constructed a dual hydrogel delivery system consisting of TGF-β3 and IGF-1 to promote OC tissue regeneration in a full-thickness OC defect model in rabbits. A novel nanoparticle that can deliver SDF-1 and BMP-2 simultaneously with high biomolecular loading capacity and prolonged release effect can stimulate MSC migration and promote better OC regeneration. Shi et al. constructed an injectable hydrogel by loading nanosilicate (SN) and stromal cell-derived factor-1 alpha (SDF-1α) into gelatin-methacryloyl (GelMA). The hydrogel effectively promotes the migration and homing of MSCs and has efficient OC repair ability. GelMA has shown good bone regeneration ability in a rat calvarial defect model [111].
Small-molecule drugs
In addition to GFs, much attention has been paid to the potential of small molecule drugs in cartilage repair and regeneration. These small molecules primarily target signaling pathways, enzymes, and receptors that have roles in the formation and upkeep of cartilage. One of the primary mechanisms through which small molecules facilitate the repair and regeneration of cartilage is by stimulating and inducing chondrogenesis. Kartogenin (KGN), a heterocyclic small molecule, can enhance the chondrogenic differentiation of MSCs by upregulating chondrogenic gene expression and characteristic chondrocyte activity. KGN has shown a cartilage regeneration effect in a mouse model [112]. It has been reported that KGN promotes cartilage repair and prevents cartilage degeneration and subchondral bone degradation through the TGFβ/Smad signaling pathway. KGN promotes the formation of a cartilage-like transition zone at the tendon-bone junction and stimulates collagen synthesis [113]. KGN can induce bone marrow stem cells (BMSCs) to differentiate into chondrocytes. In vivo studies have demonstrated the potential cell homing effect of KGN-loaded nanoparticles to recruit endogenous BMSCs and synovial mesenchymal stem cells (SMSCs) [114]. KGN has been increasingly used to promote OC regeneration. For example, a HA hydrogel (m-HA) loaded with KGN PLGA nanoparticles (m-HA+KGN treatment) achieve favorable cartilage repair in a rabbit model [48]. KGN can improve the chondrogenic capacity of human bone marrow stem cells (hBMSCs) in vitro and in vivo and effectively supports the regeneration of hyaline cartilage and subchondral bone in a rat model of OC defects [115]. A bilayer scaffold combined with KGN and human stem cell-specific binding oligonucleotide (aptamer A19S) specifically recognizes and binds to MSCs. By recruiting MSCs to the scaffold, the bilayer scaffold enriched MSCs around OC defects and stimulated MSC directional differentiation. The excellent cartilage and subchondral bone repair ability of the bilayer scaffold was demonstrated by a rat OC defect model [50].
Small-molecule drugs can also selectively modulate the subcellular localisation and downstream transcriptional activity of transcription factors. KGN attaches to filamin A, disturbing the filamin A connection with the transcription factor core binding factor beta subunit (CBFβ) and prompting chondrogenesis by controlling the CBFβ-Runx1 transcription program [116]. In addition, subchondral bone is highly vascularized and tiny branches of the subchondral bone blood vessels can extend into areas of calcified cartilage. This feature allows for metabolic exchange between the two tissues and an integrated response to chemical and mechanical stimuli. Therefore, promoting angiogenesis is crucial for cartilage repair and regeneration. Small molecules, such as vascular endothelial growth factor A (VEGF) and FGF, can promote the growth of new blood vessels and help cartilage repair and regeneration. VEGF is a chondrocyte survival factor during development and is essential for bone formation and bone growth. Increased VEGF expression is associated with catabolic processes in chondrocytes and synoviocytes [117]. It should be noted that although small molecules have demonstrated encouraging outcomes in fostering cartilage repair and regeneration in preclinical studies, additional clinical studies are needed to validate safety and efficacy, as well as to assess long-term efficacy [118].
Although the addition of a single bioactive factor in the delivery system holds promise, the continuous proliferation and differentiation of OC chondrocytes is a complex process involving multiple factors. Therefore, to further improve the tissue regeneration effect, multi-factor combination therapy is necessary.
Anti-inflammatory drugs
Inhibition of inflammation is also a crucial role in fostering cartilage repair and regeneration. Inflammation can lead to cartilage damage and impede the repair process. The use of anti-inflammatory drugs is primarily designed to reduce inflammation and/or pain. Commonly used drugs include acetaminophen, NSAIDs, opioids, and/or glucocorticoids [119]. NSAIDs are the most frequently used drugs for the treatment of articular cartilage damage. NSAIDs inhibit the cyclooxygenase enzymes, COX-1 and COX-2, which convert arachidonic acid into prostaglandin E2, which are the precursors of prostaglandins and prostacyclins that cause inflammation and pain, respectively [120, 121]. However, prolonged use of NSAIDs may adversely affect cartilage repair. NSAIDs hinder the proliferation and differentiation of chondrocytes responsible for cartilage repair and potentially delay healing [122]. Therefore, NSAID administration should be restricted to the acute phase of an injury and used cautiously in chronic cases. In addition, studies suggest that small molecules, such as celecoxib and curcumin, can mitigate inflammation and enhance cartilage repair and regeneration by suppressing the production of inflammatory mediators, such as prostaglandins and TNF-α [123].
Immunomodulators
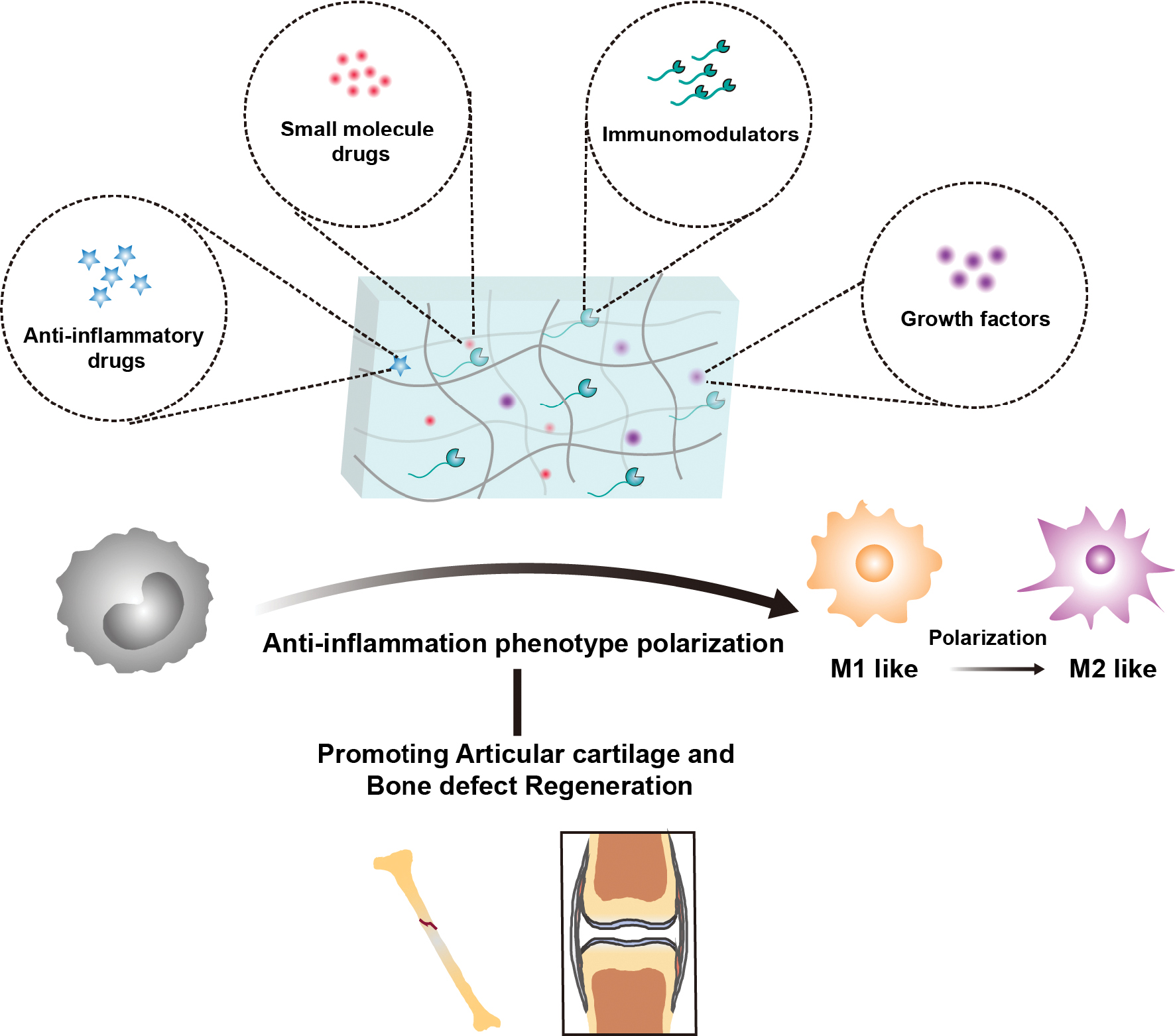
The immune microenvironment is pivotal in the regeneration of bone, cartilage, and soft tissue, especially macrophages. Dysregulated activation of macrophages can impede the process of OC tissue regeneration. Macrophages exist in various phenotypes, including the M0 (resting state), M1, and M2 phenotypes. During the initial phase of tissue repair, macrophages predominantly polarize toward the M1 phenotype and release pro-inflammatory cytokines, including TNF-α, IL-6, and IL-1β. This response promotes inflammation while facilitating the elimination of pathogens, senescent cells, and necrotic debris. In the mid-to-late stages of inflammation, macrophages undergo polarization toward the M2 phenotype and secrete anti-inflammatory cytokines, such as IL-4 and IL-10. This transition facilitates the resolution of inflammation and actively promotes tissue regeneration through matrix remodeling and angiogenesis [124, 125]. The macrophage phenotype is critical in OC repair [126]. OC tissue regeneration can be improved by regulating the polarization of macrophages and promoting the transition from M1-to-M2 macrophages, as shown in Figure 5. Chitosan engages macrophage receptors (CR3/TLR4), which downregulates the MAPK/ERK signaling cascade. This process inhibits NF-κB activation and subsequently suppresses expression of pro-inflammatory mediators, including TNF-α, IL-6, and inducible nitric oxide synthase (iNOS) [127]. Loading blueberry anthocyanins into injectable hydrogels composed of carboxymethyl chitosan (CMC) and HA mediates NF-κB downregulation, promotes polarization of M1 macrophages toward the M2 phenotype, and enhances tissue repair mechanisms [128]. HA engages TLR2 and TLR4 receptors on macrophages, potentiating pro-inflammatory responses through upregulated expression of TNF-α and IL family factors (e.g., IL-1β and IL-6) [129]. A platelet-rich plasma (PRP)-GelMA hydrogel scaffold has successfully polarized M1 macrophages into M2 macrophages by immunomagnetic modulation of the local microenvironment of OC tissue. The PRP-GelMA hydrogel scaffold was shown to promote OC repair in a rabbit model [130].
Figure 5 Schematic diagram of the regulation of macrophage phenotypes by drug delivery systems in osteochondral repair.
Other biological cues
An HA-based microcryogel can induce differentiation of MSCs into cartilage and osteogenesis and has the ability to self-assemble into OC organoids. Implantation of the gel into OC defects in dogs was shown to effectively promote the regeneration of articular cartilage and subchondral bone [131]. The results of a meta-analysis involving 21,163 randomized participants demonstrated significant advantages of HA in the treatment of knee injuries [132].
Oxidative stress caused by high levels of reactive oxygen species (ROS) in the local microenvironment can destroy the repair process following OC injury, which is an adverse factor for poor tissue repair. Evidence suggests that age-related chondrocyte damage is associated with an imbalance of ROS, which are involved in cartilage degradation and chondrocyte death. Overexpression of antioxidant genes in mice reduces joint damage [133]. A nanoenzyme hydrogel effectively alleviated the symptoms of cartilage injury, including suppression of local inflammatory factors and improved osseointegration, by scavenging endogenous overexpressed ROS. These results suggested that reducing oxidative stress is an effective treatment that promotes OC repair [134]. Researchers have designed a hydrogel drug delivery system that combines polyphenol-based SF and the antioxidant, tannic acid (TA), which can eliminate ROS in the local microenvironment, promote BMSC proliferation, and combat oxidative stress. The hydrogel drug delivery system provides a suitable microenvironment for OC regeneration [135]. The combination of biomaterials and bioactive molecules to clear endogenous ROS and provide a suitable local microenvironment for tissue regeneration has become a promising approach for the treatment of OC defects.
Glucosamine is the basic substance for the synthesis of aminoglycans and is a natural component of articular cartilage. Glucosamine decreases with age, which leads to continuous degeneration and wear of articular cartilage. Chondroitin sulfate is a type of glycosaminoglycan that synthesizes proteoglycans and protects chondrocytes. Glucosamine may alleviate pain caused by impaired lubrication function and reduced HA concentration. Glucosamine may alleviate pain caused by impaired lubrication function and reduced HA concentration [136]. Combined chondroitin sulfate-glucosamine therapy reduces serum biomarkers associated with cartilage and bone degradation, prevents cartilage degeneration, and decreases levels of inflammatory mediators, such as IL-1β and TNF-α [137].
OC tissue regenerative drug delivery system
With the continuous development of materials science, a new strategy for OC tissue regeneration is to combine a variety of composite materials to construct an ideal functional delivery system (Table 2), simulate the tissue microenvironment, and achieve the continuous release of bioactive molecules with different spatial and temporal distributions.
Table 2 Bioactive molecule delivery systems currently used in osteochondral regeneration
| Bioactive molecule | Delivery system | Application |
|---|---|---|
| TGF-β1 | PLGA nanoparticle | Increased MSCs adhesion and proliferation; increased cartilage differentiation [156] |
| TGF-β1/IGF-I | PLGA microspheres | Reduced initial burst sustained release [169] |
| TGF-β3/IGF-I | Gelatin Microspheres Hydrogel systems |
Promoted osteochondral tissue regeneration [110] |
| BMP-2 | Alginate PLGA microspheres Hyaluronic hydrogel system |
Sustained release Promoting bone repair [164, 165] |
| BMP-7/TGF-β2 | Nanoparticle | Cartilage regeneration BMSCs chondrogenic differentiation [155] |
| BMP-2/bFGF | Gelatin nanoparticles |
Programmed and sustained release [84] |
| BMP-2/TGF-β3 | Promoted bone formation [182] | |
| BMP-2/IGF-I | Gelatin particles Hydrogel system |
Promotes the subchondral bone formation [109] |
| BMP-2/VEGF | HAp Hydrogel system |
Promoted osteogenesis and angiogenesis [187] controlled and sustained release [190] |
| bFGF/HAp | Hydrogel system | Promoted hyaline cartilage and subchondral bone formation [192] |
TGF: transforming growth factor; BMP: bone morphogenetic protein; PLGA: polylactide-co-glycolide; VEGF: vascular endothelial growth factor; BMSCs: bone marrow mesenchymal stem cells; IGF-I: human insulin-like growth factor I; HAp: hydroxyapatite.
Hydrogel scaffold delivery system
Hydrogels are densely water-filled polymer networks that are simple to create, capable of encapsulating molecules within a hydrated structure, and have been thoroughly researched for regenerating cartilage tissue. The main applications of hydrogels are cellular and bioactive substance delivery systems. The hydrogel delivery system can provide support for chondrocytes and the ECM due to the nature of the hydrogel and the OC organization [138]. The distinctive structure of the hydrogel creates an optimal local microenvironment that supports the chondrogenic differentiation of MSCs and enhances cartilage regeneration. Osteoinduction refers to the ability to stimulate stem and progenitor cells to differentiate into osteogenic lineages in a laboratory setting [139]. Chondrogenesis refers to the process by which MSCs differentiate into chondrocytes [140]. OC regeneration is associated with the generation of cells associated with bone and cartilage. A CS-based hydrogel delivery system has enhanced cartilage regeneration and greatly improved repair of cartilage defects by delivering MSCs and improving the regeneration microenvironment [141]. The ideal hydrogel delivery system should have a microenvironment conducive to MSC adhesion and proliferation, and provide inductive signals to promote osteogenic and chondrogenic differentiation of MSCs.
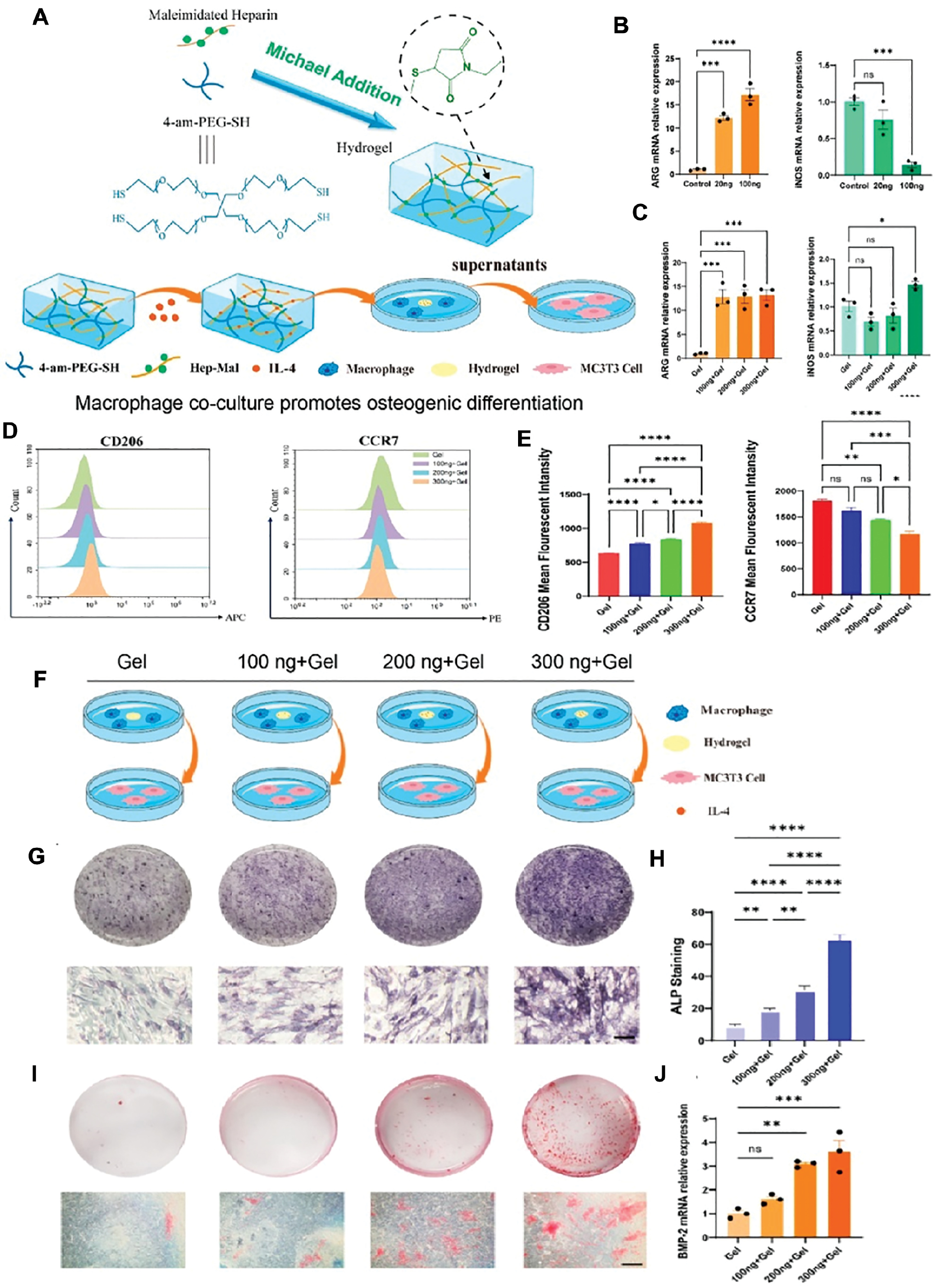
The immunomodulatory hydrogel synthesized by combining the advantages of a hydrogel and M2 macrophages has a very good effect on OC regeneration. Ji et al. [105] developed a macrophage regulatory drug delivery system composed of porous chitosan (CS) microspheres and hydroxypropyl chitin (HPCH) hydrogel, in which dimethyloxyallyl glycine (DMOG) was encapsulated in a thermosensitive HPCH hydrogel (HD). KGN was coupled to porous CS microspheres (CSK-PMS). The prepared HD/CSK-PMS composite hydrogel delivery system can effectively regulate the microenvironment at the defect site, achieve M2 polarization of local macrophages, and promote cartilage regeneration. Rapidly degrading HD is conducive to the regeneration of hyaline cartilage, while highly stable CSK-PMS supports the regeneration of endochondral osteogenesis and subchondral bone. In vitro and in vivo evaluations have shown that the newly developed HD/CSK-PMS, as a controlled drug delivery system, can effectively regulate the microenvironment at OC defects, polarize local pro-inflammatory M1 macrophages into pro-regenerative M2 macrophages, and promote cartilage regeneration. Yang et al. [142] designed a cell adhesion peptide CRGD)-modified PEG hydrogel to improve the ability to promote chondrogenic differentiation by increasing the number of MSCs and inducing macrophage polarization to the M2 phenotype. IL-4 enhances the immunoregulatory capacity of macrophages by promoting anti-inflammatory polarization. IL-4 suppresses pro-inflammatory cytokine expression within OC injury microenvironments, including IL-1β, TNF-α, and IL-6 in synovial fibroblasts and chondrocytes, thereby mitigating tissue-destructive inflammation [143]. Incorporating anti-inflammatory bioactive factors (e.g., IL-4 and anthocyanins) into hydrogel systems attenuates pathologic inflammation and orchestrates pro-regenerative microenvironments through targeted immunomodulation and enhanced cellular cross-talk. Gong et al. [59] designed a hydrogel delivery system containing IL-4, which comprises an IL-4-loaded GelMA upper layer and a porous polycaprolactone and hydroxyapatite (PCL-HAP) lower layer. Sixteen weeks after implantation of the hydrogen delivery system containing IL-4 in a rabbit OC defect repair model, the histologic score of the IL-4-loaded hydrogel delivery system was 24±2, which was 2.18 times higher than the untreated group and 1.5 times higher than the unloaded IL-4 group. These findings indicated that the hydrogel delivery system loaded with IL-4 promotes the regeneration of cartilage and subchondral bone and increases the formation of new cartilage and bone tissue. Zhao et al. [144] modified heparin with maleimide and combined the heparin modification with IL-4 to prepare the PEG-SH hydrogel. The hydrogel loaded with IL-4 has good biological properties. Overexpression of M2 macrophage-related phenotypic genes polarizes M2 in macrophages and regulates the immune microenvironment. The effect of co-culture with MC3T3-E1 cells in promoting osteogenesis is shown in Figure 6.
Figure 6 (A) Hydrogels were produced by Michael addition using maleimide-modified heparin molecules. Macrophage supernatant was used to complete the co-culture experiment. (B–E) Relative expression of M1 and M2 macrophage surface marker genes. (B) Arg and iNOS expression after 48 h of direct addition of IL-4 to the medium. (C) Hydrogel conditioned media conditioned medium after 7 d of incubation for Arg and iNOS expression. (D) Macrophage polarization markers (CD206 and CCR7) detected by flow cytometry in 5 d. (E) Mean fluorescence intensity analysis of CD206 and CCR7. (F) Schematic diagram of the co-culture model. (G) Macrophages treated with hydrogel-conditioned media promoted MC3T3-E1 osteogenesis. ALP staining of macrophages co-cultured for 7 d with different conditioned media (scale bars = 100 μm). (H) ALP quantitative analysis results. (I) Alizarin red staining of macrophages cocultured for 14 d with different conditioned media (scale bars = 100 μm). (J) Relative expression of BMP-2 gene expression in macrophages after co-culture with hydrogel for 5 d. *P < 0.5, **P < 0.01, ***P < 0.001, ****P < 0.0001, ns means no significance. Figure 6 was reproduced from ref [144] with permission from American Chemical Society. Copyright 2024.
The physicochemical properties of the hydrogel delivery system can be customized depending on the choice of material. Zhang et al. [145] designed an enzyme-linked cross-linked SF-laponite (LAP) nanocomposite hydrogel. Incorporation of a small amount of LAP (1% w/v) into SF greatly improved the mechanical properties and hydrophilicity of the hydrogel and promoted the osteogenic and chondrogenic differentiation of BMSCs. SF-LAP hydrogel promoted simultaneous regeneration of cartilage and subchondral bone in a rabbit full-thickness OC defect model. In addition, Zhu et al. [146] added bacterial cellulose to alginate dual network (DN) hydrogel and greatly improved the biological strength of the hydrogel. Two different sizes of HAP, HAP particles, and HAP nanocrystles, were incorporated into the hydrogel to promote the simultaneous repair of cartilage and subchondral bone in the rabbit OC defect model.
In addition, hydrogel delivery can also be tailored according to pH or temperature changes in the local OC microenvironment to control the release of bioactive substances [147]. The continuous release of bioactive substances can provide a continuous chemical signal for tissue regeneration. George et al. [148] designed a pH-responsive double crosslinked hydrogel by combining a crosslinked catechol functional group (DOPA) and OPF. The incorporation of DOPA alters the surface chemistry and mechanical properties of the hydrogel. The attachment and proliferation of pre-osteoblasts were enhanced. Nelson et al. [149] designed an injectable, degradable, sustained-release, and sequential release thermos-responsive hydrogel. This hydrogel prolonged the continuous release of bovine serum albumin (BSA).
While hydrogels offer sustained drug release and chemical signaling capabilities, hydrogels specifically tailored for osteoinduction and chondrogenesis have gained popularity in OC regeneration. However, using bioactive molecules or materials for osteoinduction and chondrogenesis frequently poses challenges, including instability, immunogenicity, high cost, and potential clinical side effects, all of which require careful consideration. Second, due to inherently weak mechanical properties, hydrogels used alone are more suitable to provide injectable and local OC regeneration therapy. Hydrogels are combined with synthetic polymers to improve structural and physical properties to further enhance bone and cartilage regeneration.
Nanoparticle delivery system
Nanomaterials have been developed for the regulation of drug release site and timing due to excellent controlled release properties. Nanocarriers are versatile with respect to size, shape (spherical, rod-shaped, or cuboidal), composition, and surface charge. In addition, the incorporation of nanomaterials can reduce the side effects of irritating and sensitive drugs. Nanomaterials are used as effective drug delivery systems to promote cartilage and bone tissue regeneration based on the advantages of nanomaterials as delivery systems. Frequently used degradable nanomaterials include collagen, CS, HAP, PLA, and PLGA; non-degradable nanomaterials include lipids, dendrimer, silica, and metals [150, 151] A biphasic semi-interpenetrating polymer network (SIPN) hydrogel containing CS nanoparticles for functional cartilage repair [152]. Radhakrishnan et al. [151] designed a hydrogel loaded with CS nanoparticles (CS-NPs) and nano-hydroxyapatite (nHAP) to successfully promote cartilage regeneration and subchondral bone formation. Oliveira et al. [153] showed that dexamethasone-loaded carboxymethyl CS/poly (amido-amine) dendrimer nanoparticles (CMCht/PAMAM) can be used as intracellular nanocarriers. In the absence of typical osteogenic inducers, dexamethasone (Dex) can be used to control the osteogenic differentiation of stem cells in vivo and stimulate new bone formation. Additionally, GFs and target proteins can also promote OC regeneration through nanoparticle delivery systems. Previous studies have shown that nanoparticles loaded with GFs, such as BMP-2, BMP-7, and TGF-β, have the potential to promote cartilage regeneration [154]. Lim et al. [155] designed a nanodelivery system loaded with dual growth factors (BMP-7/TGF-β2) to control the rate of GF release, which is an ideal delivery system for cartilage regeneration and chondrogenic differentiation of MSCs. Castro et al. [156] reported that PLGA nanospheres loaded with TGF-β1 could increase MSCs adhesion, proliferation, and OC differentiation in vitro.
Gelatin, a derivative of collagen, has been widely used to encapsulate bioactive molecules. Injectable colloidal gels fabricated from countercharged gelatin nanospheres have shown great potential for bone fillers and programmed drug delivery due to good clinical manipulation, ease of functionalization, and cost-effectiveness [157]. Gelatin gels overcome the disadvantages of PLGA colloidal gels, such as the lack of cell attachment sites and the release of acidic degradation products, and show obvious advantages in the programmed delivery of bioactive molecules [158]. Wang et al. [159] obtained a continuous release delivery system characterized by rapid bFGF release and durable BMP-2 release by loading bFGF onto cationic nanospheres with low cross-link density and BMP-2 onto anionic nanospheres with high cross-link density. Gelatin nanoparticles have been demonstrated to be suitable carriers for programmed and sustained release of a variety of therapeutic proteins for tissue regeneration.
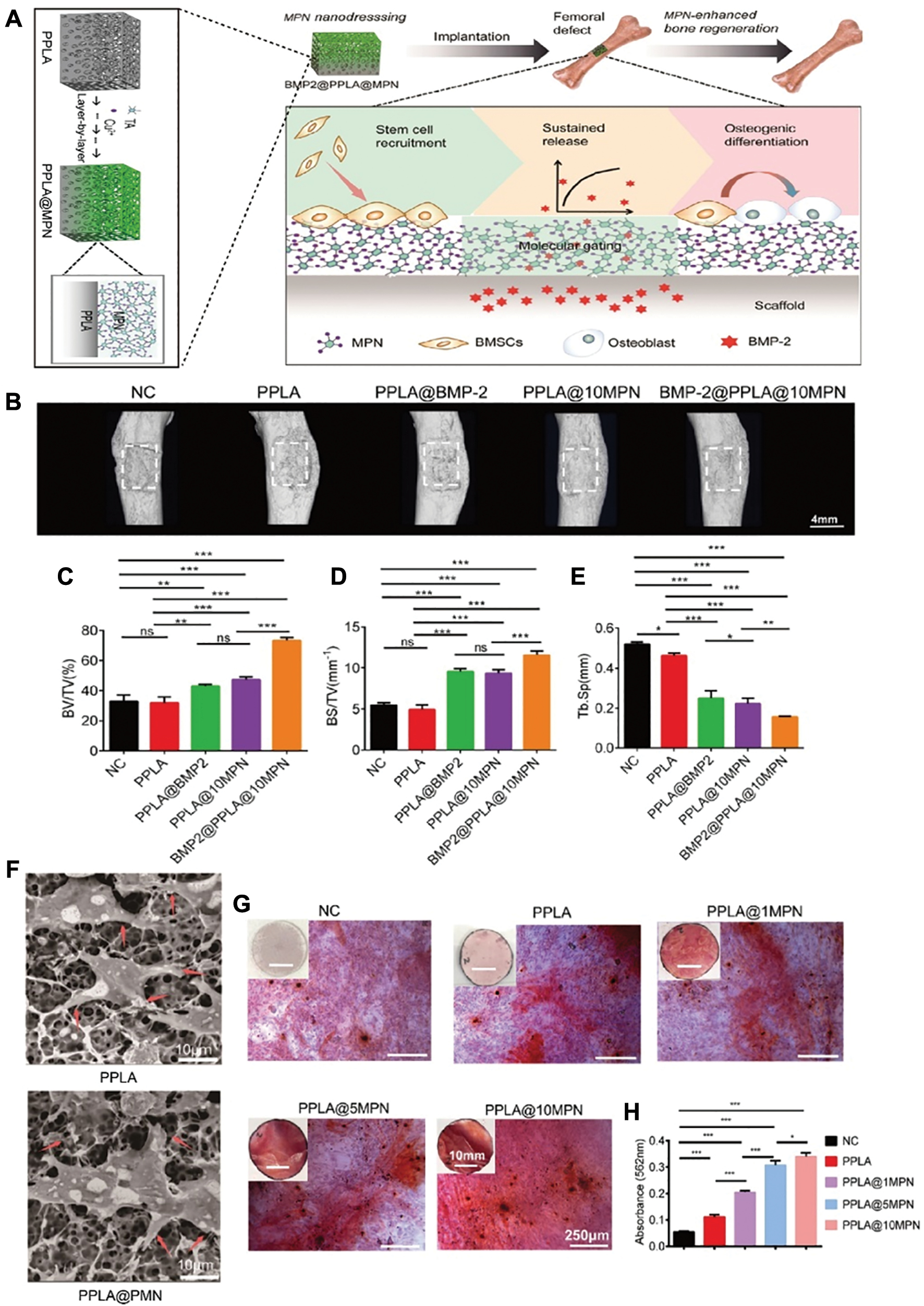
Metal nanoparticles have been widely used in tissue healing and regeneration because of the intrinsic chemical, physical, and biological properties, such as the release of bioactive ions (Ca, Mg, Sr, Si, B, Fe, Cu, and Zn), inducing changes in cell phenotype or regulating the immune microenvironment. Metal nanoparticles can affect stem cell proliferation and differentiation by regulating signaling pathways, ROS production, and multiple transcription factors [160]. The biophysical properties of metal nanoparticles, such as morphology, charge, size, electrostatic interactions, and stiffness, can be modulated by binding to polymers [84]. For example, when metal particles are combined with porous poly(dl-lactide) [PPLA], the bioactive interface provided by metal particles compensates for the lack of bioactive cell-material interface and explosive release of GFs in PPLA, resulting in sustained release of BMP-2 combined with the osteogenic ability of metal particles. The migration and osteogenic differentiation of BMSCs were successfully promoted (Figure 7) [161].
Figure 7 (A) Proposed mechanism of enhanced bone regeneration via MPN nanodressing of the PPLA scaffold in a femoral bone defect model. (B) Micro-CT analysis of bone regeneration in femoral defects at week 4 postoperatively. Representative 3D digital reconstructed planform images. The white color represents the repair area in the femoral bone. (C−E) Quantitative analysis of the mandibular bone by reconstruction and analysis software. (F) SEM images of BMSCs grown on PPLA and PPLA@MPN scaffolds. Red arrows indicate the extension of cellular pseudopodia. (G) Representative photographs of alizarin red staining of BMSCs in different groups at day 14 (macrographs of stained cells are inserted). (H) MPN significantly enhanced the formation of mineral deposition compared with the control PPLA groups. *P < 0.05, **P < 0.01, and ***P < 0.001. Mean values and error bars are defined as the mean and S.D., respectively. Figure 7 was reproduced from ref [161] with permission from American Chemical Society. Copyright 2021.
Microsphere delivery system
Microparticles are more advantageous in the application of controlled drug delivery for OC regeneration than drug-loaded nanomaterials due to side effects, such as early burst release, high chemical toxicity, and short retention time [162]. Therefore, polymeric microparticles have been widely used for the delivery of cells and bioactive substances. Among the polymeric microparticles, alginate and PLGA are most frequently used because the preparation process is gentle and does not affect the activity of the encapsulated bioactive factors [163]. Encapsulated rhBMP-2 in alginate and PLGA microparticles were delivered continuously for 28 d and showed a good ability to promote repair in a rat skull defect model [164]. In one study rhBMP-2 delivered by surface-functionalized strontium alginate microparticles retained biological activity and stimulated higher alkaline phosphatase activity in vitro. rhBMP-2 release was sustained for approximately 3 weeks and successfully induced bone formation and biomechanical firm (a 5.3-fold increase in bone volume fraction and a 2.6-fold increase in bending stiffness [flexion/extension] compared to control) in vivo [165]. In addition, alginate microspheres can autonomously induce calcification in vivo. Crosslinked calcium alginate microspheres were implanted into nude mice and mineralized into calcium phosphate (CaP) in vivo through the interaction between calcium ions and physiologic phosphate ions, which was highly consistent with hydroxyapatite found in bone [166]. This method will have great potential in the application of subchondral bone regeneration.
Bone and/or cartilage repair involves a series of cascades of GFs and chemokines. Therefore, the development of particle delivery systems that combine multiple signaling molecules has become a new research direction. A dual GF delivery system consisting of PLGA and alginate was designed to differentiate MSCs into specific lineages. The microparticle delivery system can suppress the initial burst of biomolecules, resulting in the sustained release of loaded biomolecules together for up to 4 weeks. Moreover, the gene expression of osteogenic markers was significantly upregulated [167]. SOX9-loaded and TGF-β3-coated PLGA microspheres effectively delivered bioactive molecules to hMSCs, which resulted in upregulation of hMSC-specific marker genes and enhanced chondrogenic differentiation of hMSCs [168]. The encapsulation of IGF-I and TGF-β1 in PLGA microspheres clearly reduced the initial burst of both GFs and the sustained release of both GFs in biologically active forms for up to 70 d. SOX9-loaded and TGF-β3-coated PLGA microspheres have great potential in the application of cartilage tissue regeneration [169].
Inorganic polymer delivery system
Studies have shown that promoting simultaneous repair of cartilage and subchondral bone is the best strategy for OC tissue regeneration. Subchondral bone is rich in blood vessels, which provide nutrients for articular cartilage and has the mechanical properties necessary for supporting the joint. Materials possessing adequate compressive strength include metallic materials, BG, and bioceramics and are the best choices for promoting subchondral bone regeneration. In addition, the ability to induce the formation of apatite is another prerequisite for the selection of materials [170].
Ceramic is the most commonly used inorganic material in bone defect repair. However, due to the lack of biological functions of ceramic materials (osteoinduction and osteogenesis), various peptides, proteins, and bioactive molecules are usually modified on the surface of ceramic scaffolds to improve bone conduction [171]. The modified bioceramic scaffolds can induce the biological activity of the local microenvironment of bone tissue and provide suitable mechanical strength and porosity for tissue regeneration. To enhance the osteogenic capability of hydroxyapatite/β-tricalcium phosphate (HAP/β-TCP), the ECM phosphoglycoprotein peptide (MEPE), which is known for its ability to promote osteoblast differentiation, was directly immobilized on HAP/β-TCP particles, then implanted into a mouse skull defect model for microCT and histologic analysis; a marked increase in bone regeneration and bone area associated with physiologic bone remodeling was observed [172]. Zhao et al. [173] designed a BMP-2-loaded calcium-deficient hydroxyapatite (CDHAP) porous scaffold and a sulfated chitosan (SCS)-coated GF delivery system. Studies have shown that SCS coating enhances the in vitro release properties of CDHAP/BMP-2 composites and promotes new bone formation in vivo. Increased bone formation was observed in both HAP/β-TCP-dipyridamole and HAP/β-TCP-BMP-2 groups when HAP/β-TCP was coated with BMP-2 or dipyridamole and implanted into C57B6 and A2AKO mouse models with skull bone defects with a trend toward increased remodeling [174]. In addition to peptides, the incorporation of MSCs also contributed to the overall biological function of ceramic materials. MSCs can effectively undergo osteogenic differentiation and have the ability to injure chemotaxis. Incorporating platelet-derived growth factor (PDGF) and hMSCs into HAP/TCP scaffolds improves the regenerative potential of osteocytes [175].
Another commonly used class of inorganic materials is BG. BGs have excellent bone conduction, osteogenesis, osteoinduction and mechanical strength properties. Specifically, mesoporous bioglass (MBG) has an ordered and adjustable mesoporous pore structure, a large pore volume, a specific surface area, higher drug loading, and better sustained release performance [176, 177]. Sustainable adsorption to release drug molecules for drug and GF delivery in bone regeneration has been significantly developed [178].
However, the inherent shortcomings existing in MBG materials, such as brittleness, high degradability, and surface instability, affect mechanical strength and cytocompatibility [179]. For example, combining MBG with a PLGA polymer significantly improves the biological activity, degradation rate, and controlled release performance of the material for drug delivery [180]. Wu et al. combined SF, which has good biocompatibility and tensile strength, with MBG to optimize the mechanical properties. The drug delivery and cytocompatibility of the materials were evaluated by Dex and BMSCs, respectively. The results showed that SF-MBG scaffolds could induce homogeneous and continuous Dex release and increase the adhesion, proliferation, and osteogenic differentiation of BMSCs [181].
Controlled-release delivery system
OC tissue regeneration is a cascade process regulated by a variety of cytokines and GRs. Simmons et al. designed a co-delivery system using BMP-2 and TGF-β3, which promoted bone formation more significantly than BMP-2 or TGF-β3 alone [182]. Dual delivery of VEGF and BMP-2 enhanced bone bridge and bone defect healing more than either delivery alone in a rat calvaria defect model [183, 184].
The precise regulation of drug delivery systems, including chemical modification, physical blending, and surface modification, is essential for the continuous release of bioactive molecules. Yilgor et al. [185] demonstrated that the structure of the delivery system and the mode of delivery of GFs had differential effects on the proliferation and osteogenic differentiation of MSCs. The structure of PCL and PLGA can be designed to achieve controlled and sustained delivery of one or more proteins [186]. Precise spatiotemporal control over the release kinetics of therapeutic agents (e.g., small molecules, genes, peptides, and proteins) is critical for guiding tissue regeneration in controlled delivery systems. Bonani et al. [186] engineered gradient PCL-PLGA nanofibers to achieve directional release. Confocal imaging confirmed close alignment between designed versus actual fluorescent dye distributions within the fibers, which validated gradient fidelity. During degradation, fiber hydration-induced volumetric expansion resulted in progressive diameter increase, spatially constraining molecular diffusion from the scaffold. Subsequent analysis of the PCL-PLGA delivery system time-delayed release kinetics used fluorescent-tagged small molecules and proteins as model therapeutic agents. The results demonstrated exceptional size-dependent release separation. Protein released > 88% separation efficiency at a critical scaffold thickness of 200 μm, while small molecules exceeded 82% efficiency (Figure 8). This finding confirms precise spatiotemporal control over distinct molecular payloads. The hydroxyapatite delivery system loaded with BMP-2 and VEGF prepared using the layer-by-layer assembly (LBL) method can continuously release the two GFs. The BMP-2/VEGF composite delivery system has good osteogenesis and angiogenesis ability in the rabbit skull defect model and can effectively promote new bone formation [187].
Figure 8 (A) Design illustrations and laser confocal image of the PCL-PLGA delivery system. (B) Representative SEM micrographs of the PCL-PLGA nanofibrous scaffold with an internal compositional gradient. Images were taken from the PLGA side. Changes in the nanofiber morphology after 1, 3, and 5 weeks of degradation in phosphate buffer solution at 37 °C. The unchanged PCL nanofibers underneath the PLGA layer were found after 5 weeks of degradation. (scale bar = 10 μm) GPC analyses of the as-spun PCL-PLGA after hydrolytic degradation. (C) GPC curves of PCL-PLGA. (D) Changes in the average molecular weight and remaining PLGA content determined by deconvolution of the GPC curves. (E) Overall remaining mass percentage of the scaffolds determined by the gravimetric method and measurement from GPC curves. (F) Dual-drug release from one surface of the scaffold. Illustration of the compositional pattern of nanofibers. Cumulative release curve of AlbF and AlbT. Comparison of AlbF and AlbT release during the first 10 d. (G) PCL-PLGA scaffold for the sequential release of proteins. Illustration of the compositional pattern of nanofibers. AlbF-loaded PLGA nanofibers were confined in the middle of the scaffold, while AlbT-loaded PLGA nanofibers were close to side B. Cumulative release profiles of AlbF and AlbT to both surfaces of the scaffold. Net release profiles of AlbF and AlbT to side B during the first 12 d. (H) Dual-drug release from the opposite surfaces of the PLGA-PCL-PLGA scaffold. Illustration of the compositional pattern of nanofibers. Cumulative release curve of AlbT and AlbF. Release of green-emitting AlbF was mainly confined to side A, whereas release of red-emitting AlbT is mainly confined to side B. Figure 8 was reproduced from ref [186] with permission from American Chemical Society. Copyright 2012.

In addition to achieving sustained and controlled delivery, the dose of the bioactive molecule loaded into the delivery system is also important. Various strategies have been devised to increase the total payload of bioactive molecules or drugs in the delivery system, allowing for sustained release over time while maintaining effectiveness. For example, delivery systems fabricated using supercritical CO2 technology can enable the continuous delivery of two or more GFs at controlled doses and rates [188]. The VEGF encapsulated porous PLA delivery system prepared by Kanczler et al. can greatly improve the loading rate of VEGF without affecting its biological activity [189]. Hydrogels can also be used to construct delivery systems for controlled and sustained release of therapeutic drugs. Sustained release of BMP-2 was observed throughout the implantation period when BMP-2 was embedded in a polypropylene scaffold with PLGA microspheres surrounded by a VEGF-loaded gelatin hydrogel, which was implanted into an SD rat bone defect model [190].
Multiphase structure delivery system
Biphasic and heterogeneous drug delivery systems have been devised to meet the apparently distinct biological and mechanical demands of cartilage and subchondral bone. These systems often utilize polymers, such as gelatin, collagen, and PLA, for cartilage layers, while bioceramics, such as HA and TCP, are used for subchondral bone layers within biphasic and multiphase scaffolds. Such multiphase delivery systems can create biomimetic regions resembling the layered structure and composition of natural OC tissue, facilitating the concurrent regeneration of cartilage and subchondral bone.
Jiang et al. [191] designed a multiphase delivery system comprised of an agarose gel poly-milk PLGA and 45S5 BG that enables region-specific co-culture of chondrocytes and osteoblasts to generate distinct continuous regions. The multiphase delivery system promoted chondrocyte mineralization, calcification, and subchondral bone formation. Fang et al. [192] constructed a chitosan bilayer gel delivery system with an upper layer of bFGF to induce chondrogenesis and a lower layer of uniformly distributed hydroxyapatite nanoparticles (HAPp). In vitro studies showed that the delivery system could promote upper chondrogenic differentiation and lower osteogenic differentiation. The system promoted both hyaline cartilage and subchondral bone formation and significantly improved osteochondral repair in vivo. Zheng et al. [193] constructed a bilayer delivery system containing a hydrogel upper layer and a polymeric nanofiber lower layer. The upper layer was loaded with the cartilage-inducing drug, KGN, and the lower layer was loaded with the osteogenic-inducing factor, BMP-2-derived polypeptide (P24 polypeptide). The dual-layer delivery system loaded with KGN P24 peptide can induce MSC differentiation into chondrocytes and osteoblasts, respectively. This system significantly promoted the regeneration of OC tissue in rabbit knee joints in vivo. A three-phase GelMA hydrogel delivery system has been developed for OC defect repair. The upper layer of the system is covalently bound to CS to promote the chondrogenic differentiation of BMSCs. The incorporation of hydroxyapatite into the middle and lower layers effectively enhanced angiogenesis and osteogenic induction. Hydroxyapatite significantly promoted cartilage and bone repair in a rabbit OC defect model [194]. Chen et al. [195] constructed a two-layer gene delivery system consisting of a chitosan-gelatin upper layer loaded with a TGF-β1 plasmid and a hydroxyapatite/chitosan-gelatin lower layer loaded with BMP-2 plasmid. This gene delivery system can induce MSCs to differentiate into chondrocytes and osteoblasts in vitro, respectively. The gene delivery system also promoted regeneration of articular cartilage and subchondral bone in a rabbit knee cartilage defect model.
Analysis of the efficacy and limitations of these delivery systems
Hydrogel delivery systems typically utilize ECM-mimetic biomaterials that offer inherent biocompatibility, tunable mechanical properties, and straightforward fabrication. Both natural polymers (e.g., collagen, HA, and chitosan) and synthetic polymers (e.g., PEG, PLA, and PVA) can be engineered into functional hydrogel platforms for controlled therapeutic delivery [196]. Hydrogels enable versatile loading of therapeutic agents, including small molecules, proteins, and DNA through direct integration into polymer matrices during fabrication. These systems exhibit exceptional histocompatibility and biosafety, while simultaneously preserving bioactivity and shielding payloads from enzymatic degradation. However, the inherently low mechanical strength (typically, 0.1–1 MPa tensile strength) critically limits load-bearing applications where cortical bone (> 100 MPa) or metal implants (> 500 MPa) are required. This mechanical deficiency limits utility in orthopedic procedures demanding structural integrity [197]. To overcome mechanical limitations, contemporary research focuses on functionalizing hydrogel scaffolds with compressive reinforcement, which endows rigid load-bearing capability. These engineered systems provide stable mechanical support while establishing direct osteointegration with subchondral bone, accelerating OC regeneration through biomimetic stress transfer. However, long-term toxicity of biomaterials remains critical. Degradation byproducts may exert chronic cytotoxicity or disrupt paracrine signaling. Future studies must address host-material fusion dynamics in cartilage interfaces and off-target effects on regenerative pathways, particularly for synthetic polymer hydrogels.
Metal-based delivery systems synergize high mechanical strength (0.1–1 GPa yield strength) with biocompatibility, enabling long-term use in load-bearing bone regeneration. However, the excessive Young’s modulus (110–200 GPa vs. cortical bone 15–30 GPa) induces stress-shielding effects, triggering bone resorption through Wolff’s law. While controlled porosity reduces stiffness toward trabecular bone levels, intrinsic limitations persist, such as non-degradability, fatigue-induced ion leakage, biofilm susceptibility, and fibrous encapsulation, whic compromises osseointegration.
Nanocarriers offer tunable physicochemical properties, including precisely controlled size (10–500 nm), programmable shapes (spheres, rods, and cubes), tailored composition, adjustable surface charge (± 5–50 mV), and high surface-to-volume ratios, enabling optimized biodistribution, cellular uptake, and therapeutic payload delivery [198]. Nanoparticles (NPs) significantly enhance therapeutic retention in cartilage while potentiating drug efficacy. These delivery systems mitigate enzymatic degradation and reduce intra-articular efflux through size-exclusion effects. Despite advantages, such as high drug-loading capacity and engineerable surface-to-volume ratios, NPs face colloidal instability risks. Critical barriers to clinical translation include undefined in vivo metabolic pathways and potential off-target cytotoxicity, warranting rigorous investigation of biodistribution, immune responses, and long-term articular tissue effects. Microparticles (MPs) exhibit depot-type release kinetics analogous to NPs, leveraging the larger size for extended joint residence times. This effect enables MPs to function as combination drug banks for sustained multi-agent delivery. While MPs demonstrate reduced synovial clearance and narrower release gaps, the micrometer-scale dimensions restrict penetration beyond superficial cartilage layers, limiting therapeutic access to deep OC regions.
Future research direction
Although new progress has been made in the delivery of bioactive molecules and drugs in recent years, the delivery of microRNAs (miRNAs) in OC tissue regeneration has rarely been studied. miRNAs are pivotal in modulating gene expression; tissue repair and regeneration are also regulated by miRNAs [199]. miRNAs have been shown to promote tissue regeneration. For example, Let-7 miRNAs can regulate peripheral nerve regeneration [200]. The multifunctional miRNA, miR-155, is involved in multiple neural repair processes in different CNS pathologic processes [201]. miR-19a/19b can enhance cardiomyocyte proliferation and stimulate cardiac regeneration after myocardial infarction injury [202]. miR-223-3p aids in skeletal muscle regeneration by regulating the equilibrium between pro- and anti-inflammatory factors within the skeletal muscle microenvironment [203]. miRNA expression were associated with protein turnover in articular cartilage tissue regeneration [204] and osteogenic and chondrogenic differentiation of MSCs [205]. These findings suggest that miRNA is a new research strategy and development direction for OC repair.
Immunomodulatory strategies are another avenue to explore tissue regeneration. The immune response to tissue injury plays a crucial role in both the pace and success of the healing process. Consequently, the manipulation of immune cells using biomaterials and drug delivery systems is emerging as an appealing strategy in the field of regenerative medicine [206]. For example, proinflammatory cytokines are detrimental to chondrogenesis and repair in cartilage tissue [207]. Some proinflammatory cytokines, such as TNF-α, IL-1, and IL-17, are major triggers of osteoclast activation in bone tissue and overexpression can lead to bone resorption. Osteoclast activation inhibitors, such as IL-12, IL-18, IL-33, and interferon gamma, inhibit bone resorption. Therefore, the composition of inflammatory cytokines has a decisive role in determining if bone resorption is triggered [208, 209]. This finding suggests that strategies using the regulation of inflammatory cytokines may be a novel approach to promote OC tissue regeneration. Despite a limited understanding of the underlying mechanisms of immunomodulation during tissue regeneration, the emerging field of biomaterial based immunomodulation strategies provides a new perspective for improving tissue regeneration and successfully restoring tissue function, which will promote the development of future tissue regeneration strategies [210, 211].
Perspective summary
Despite significant progress in regenerative medicine, sustained OC repair continues to pose a major scientific and clinical obstacle. With the development of materials science, the delivery of a variety of different bioactive molecules and drugs through composite materials to promote OC tissue regeneration is the trend of future development. However, there are still many challenges that need to be addressed for osteochondrogenic drug delivery systems. Bioactive molecules are affected by the various methods used to load bioactive molecules into the delivery system (e.g., organic solvents, high temperatures, and radiation). These effects can only be compensated by a higher drug load to achieve the desired release kinetics and therapeutic effect. The effectiveness of carrier sterilization in delivery systems has also not been comprehensively evaluated. The choice of sterilization method may affect the stability of bioactive molecules, resulting in the loss of activity of biological signaling pathways.
In addition, although biphasic and multilayer structures can provide a mechanical environment like physiology for OC regeneration, it is difficult for existing biotechnology to biologically mimic the natural microstructure and physiologic properties of cartilage and subchondral bone. The adhesion strength between the two adjacent layers is often insufficient in biphasic or multiphase delivery systems, resulting in delamination of the adjacent layers. In addition, drug delivery systems incorporating bioactive molecules are difficult to store and deliver due to the instability of bioactive molecules during commercialization. Issues, such as large-scale manufacturing, precisely controlled release of bioactive molecules and high medical costs remain to be solved.
In addition to performance optimization, security is also a drug delivery system to consider. Sharafat-Vaziri et al. [212] evaluated the safety and efficacy of a collagen/SF delivery system for repairing OC defects. Tamaddon et al. [213] developed a multilayer OC delivery system for OC tissue heterogeneity and verified the safety and efficacy of the delivery system in a sheep condylar model. In vivo studies showed that the delivery system significantly enhanced bone growth within 12 weeks.
Currently, only a few delivery systems are used in clinical trials of OC defects, mainly including type-I/III collagen [MACI ™ (Vericel Corporation, Cambridge, MA, USA) and Novocart 3D ™ (B. Braun Melsungen AG, Melsungen, Hesse, Germany)], HA (Hyalograft ® C, Fidia Advanced Biopolymers, Abano Terme, Veneto, Italy), PGA, PLA, and polydioxanone (BioSeed C ™, BioTissue Technologies GmbH, Freiburg, Baden-Württemberg, Germany). Recently, hydrogel drug delivery systems have received much attention in the treatment of OC defects. Among the hydrogel drug delivery systems, type-I collagen hydrogels (Koken Atelocollagen Implant KOKEN CO., LTD, Tokyo, Japan), HA hydrogels (CARTISTEM ™, Medipost Co., Ltd, Gangnam-gu, Seoul, South Korea), albumin and HA hydrogels (Novocart Inject ™, TETEC AG, Tübingen, Baden-Württemberg, Germany), fibrin (Chondron ™, Sewon Cellontech Co., Ltd, Mapo-gu, Seoul, South Korea), and agarose and alginate hydrogels (Cartipatch ™, TBF Tissue Engineering, Mende, Lozère, Occitanie, France) have wide application prospects. However, the overall clinical outcome is not satisfactory and more high-level studies and longer follow-up are needed.
In summary, an optimal drug delivery system needs to enhance multiple characteristics, such as size, shape, encapsulation efficiency, deformability, thermal responsiveness, biocompatibility, biodegradability, and cost-effectiveness. How to select the appropriate biomolecules, delivery systems, and processing technologies to construct the optimal therapeutic system and achieve the ideal tissue regeneration effect requires complex design and engineering.
An ideal drug delivery system maintains its physical properties in the OC tissue and supports chondroprogenitor cell proliferation by controlling the release of bioactive molecules to promote chondroprogenitor cell differentiation. In addition, an ideal delivery system should mimic the biomechanics, porosity, and hierarchical microstructure of the OC interface with degradation timing synchronized with the rate of new tissue formation.
Data availability statement
Not applicable.
Authors’ contributions
Conceptualization, J.S. and B.L.; writing—original draft preparation, J.S., J.Z., and L.L; writing-review and editing, Y.Z., C.L., and B.L.; visualization, J.S., J.Z., L.L.,W.K., P.Z., G.S., H.Z., and W.S.; supervision, C.L. and B.L.; project administration, C.L. and B.L.; and funding acquisition, J.R., C.L., and B.L. All authors have read and agreed to the published version of the manuscript.
Ethical approval and consent to participate
No human or animal studies were performed by the authors. Therefore, ethical approval and informed consent were not required.
Acknowledgements
This work was supported by the Engineering and Physical Sciences Research Council via DTP CASE Programme [grant number, EP/T517793/1], the NIHR UCLH BRC- UCL Therapeutic Acceleration Support (TAS) Fund [grant number, 564021 – linked to Lead 557595], and the European Committee via H2020 iP-OSTEO – H2020 programme (project number 824007). This research was funded by The Key Research Project of Linfen City (grant number 2405) and The Basic Research Project of Shanxi Province (grant number 202403021221346).
Conflict of interest
Dr. Chaozong Liu is the Co-Editor-in-Chief of BIO Integration. He was not involved in the peer review or handling of the manuscript. The other authors have no other competing interests to disclose.
Graphical abstract
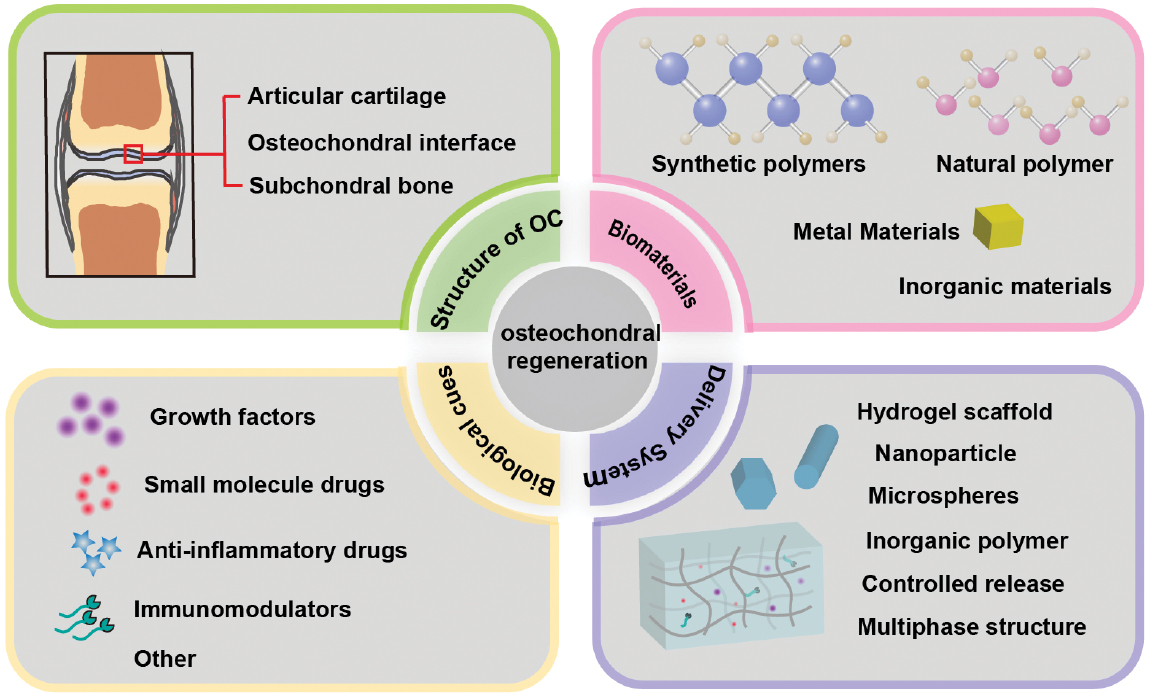
Highlights
- Osteochondral regeneration faces challenges due to cartilage’s avascularity and poor self-repair.
- Biomaterial-based delivery systems (hydrogels, nanoparticles, multiphase scaffolds) enable spatiotemporal control of bioactive cues (growth factors, chondroinductive small molecules).
- These systems enhance penetration, prolong retention, and promote simultaneous cartilage/subchondral bone repair.
- This paper systematically reviews the latest advancements and explores the great potential of biomaterials in drug delivery systems for bone and cartilage regeneration.
- It provides compelling evidence for bone and cartilage tissue regeneration in both basic and clinical research.
In brief
In this paper, the biomaterial delivery systems developed in recent years have been reviewed to identify the key factors for the success of OC regeneration. Key factors for successful OC regeneration have been considered in this review, as follows: i) biological structure of osteochondral units; ii) types and combinations of biomaterials; iii) drug of choice; and iv) commonly used delivery systems.
References
- Sophia Fox AJ, Bedi A, Rodeo SA. The basic science of articular cartilage: structure, composition, and function. Sports Health 2009;1(6):461-8. [PMID: 23015907 DOI: 10.1177/1941738109350438]
- Wei W, Dai H. Articular cartilage and osteochondral tissue engineering techniques: recent advances and challenges. Bioact Mater 2021;6(12):4830-55. [PMID: 34136726 DOI: 10.1016/j.bioactmat.2021.05.011]
- Borrelli J Jr, Olson SA, Godbout C, Schemitsch EH, Stannard JP, et al. Understanding articular cartilage injury and potential treatments. J Orthop Trauma 2019;33(Suppl 6):S6-12. [PMID: 31083142 DOI: 10.1097/BOT.0000000000001472]
- Chubinskaya S, Haudenschild D, Gasser S, Stannard J, Krettek C, et al. Articular cartilage injury and potential remedies. J Orthop Trauma 2015;29(Suppl 12):S47-52. [PMID: 26584267 DOI: 10.1097/BOT.0000000000000462]
- Wilder FV, Hall BJ, Barrett JP Jr, Lemrow NB. History of acute knee injury and osteoarthritis of the knee: a prospective epidemiological assessment. The Clearwater Osteoarthritis Study. Osteoarthritis Cartilage 2002;10(8):611-6. [PMID: 12479382 DOI: 10.1053/joca.2002.0795]
- Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg Am 2003;85-A(Suppl 2):58-69. [PMID: 12721346 DOI: 10.2106/00004623-200300002-00008]
- Natoli RM, Revell CM, Athanasiou KA. Chondroitinase ABC treatment results in greater tensile properties of self-assembled tissue-engineered articular cartilage. Tissue Eng Part A 2009;15(10):3119-28. [PMID: 19344291 DOI: 10.1089/ten.TEA.2008.0478]
- Kreuz PC, Steinwachs MR, Erggelet C, Krause SJ, Konrad G, Uhl M, Südkamp N. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthr Cartil 2006;14(11):1119-25. [PMID: 16815714 DOI: 10.1016/j.joca.2006.05.003]
- Gou GH, Tseng FJ, Wang SH, Chen PJ, Shyu JF, et al. Autologous Chondrocyte Implantation Versus Microfracture in the Knee: A Meta-analysis and Systematic Review. Arthrosc 2020;36(1):289-303. [PMID: 31708355 DOI: 10.1016/j.arthro.2019.06.033]
- Gryglewicz J, Dragan SŁ. Review of surgical management techniques for osteochondral lesions. Ortop Traumatol Rehabil 2023;25(3):157-63. [PMID: 38078352 DOI: 10.5604/01.3001.0053.7978]
- Mithoefer K, McAdams T, Williams RJ, Kreuz PC, Mandelbaum BR. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: an evidence-based systematic analysis. Am J Sports Med 2009;37(10):2053-63. [PMID: 19251676 DOI: 10.1177/0363546508328414]
- Gomoll AH, Madry H, Knutsen G, van Dijk N, Seil R, et al. The subchondral bone in articular cartilage repair: current problems in the surgical management. Knee Surg Sports Traumatol Arthrosc 2010;18(4):434-47. [PMID: 20130833 DOI: 10.1007/s00167-010-1072-x]
- Dewan AK, Gibson MA, Elisseeff JH, Trice ME. Evolution of autologous chondrocyte repair and comparison to other cartilage repair techniques. BioMed Res Int 2014;2014:272481. [PMID: 25210707 DOI: 10.1155/2014/272481]
- Mistry H, Connock M, Pink J, Shyangdan D, Clar C, et al. Autologous chondrocyte implantation in the knee: systematic review and economic evaluation. Health Technol Assess 2017;21(6):1-294. [PMID: 28244303 DOI: 10.3310/hta21060]
- Chimutengwende-Gordon M, Donaldson J, Bentley G. Current solutions for the treatment of chronic articular cartilage defects in the knee. EFORT Open Rev 2020;5(3):156-63. [PMID: 32296549 DOI: 10.1302/2058-5241.5.190031]
- Bosnakovski D, Mizuno M, Kim G, Takagi S, Okumura M, et al. Chondrogenic differentiation of bovine bone marrow mesenchymal stem cells (MSCs) in different hydrogels: influence of collagen type II extracellular matrix on MSC chondrogenesis. Biotechnol Bioeng 2006;93(6):1152-63. [PMID: 16470881 DOI: 10.1002/bit.20828]
- Zhu J. Bioactive modification of poly(ethylene glycol) hydrogels for tissue engineering. Biomaterials 2010;31(17):4639-56. [PMID: 20303169 DOI: 10.1016/j.biomaterials.2010.02.044]
- Muzzarelli RAA, Greco F, Busilacchi A, Sollazzo V, Gigante A. Chitosan, hyaluronan and chondroitin sulfate in tissue engineering for cartilage regeneration: a review. Carbohydr Polym 2012;89(3):723-39. [PMID: 24750856 DOI: 10.1016/j.carbpol.2012.04.057]
- Bottini M, Bhattacharya K, Fadeel B, Magrini A, Bottini N, et al. Nanodrugs to target articular cartilage: An emerging platform for osteoarthritis therapy. Nanomedicine 2016;12(2):255-68. [PMID: 26707894 DOI: 10.1016/j.nano.2015.09.013]
- Luo Y, Sinkeviciute D, He Y, Karsdal M, Henrotin Y, et al. The minor collagens in articular cartilage. Protein Cell 2017;8(8):560-72. [PMID: 28213717 DOI: 10.1007/s13238-017-0377-7]
- Lam J, Lee EJ, Clark EC, Mikos AG. Honing cell and tissue culture conditions for bone and cartilage tissue engineering. Cold Spring Harb Perspect Med 2017;7(12):a025734. [PMID: 28348176 DOI: 10.1101/cshperspect.a025734]
- Gahunia HK, Pritzker KPH. Structure and function of articular cartilage. In: Gahunia HK, et al. editors. Articular cartilage of the knee: health, disease and therapy. New York, NY: Springer New York; 2020. pp. 3-70. [DOI: 10.1007/978-1-4939-7587-7_1]
- Madry H, van Dijk CN, Mueller-Gerbl M. The basic science of the subchondral bone. Knee Surg Sports Traumatol Arthros 2010;18(4):419-33. [PMID: 20119671 DOI: 10.1007/s00167-010-1054-z]
- Oláh T, Madry H. The osteochondral unit: the importance of the underlying subchondral bone. In: Farr J, Gomoll AH, editors. Cartilage restoration: practical clinical applications. Cham: Springer International Publishing; 2018. pp. 13-22.
- Pan J, Wang B, Li W, Zhou X, Scherr T, et al. Elevated cross-talk between subchondral bone and cartilage in osteoarthritic joints. Bone 2012;51(2):212-7. [PMID: 22197997 DOI: 10.1016/j.bone.2011.11.030]
- Oliveira Silva M, Gregory JL, Ansari N, Stok KS. Molecular signaling interactions and transport at the osteochondral interface: a review. Front Cell Dev Biol 2020;8:750. [PMID: 32974333 DOI: 10.3389/fcell.2020.00750]
- Sharma AR, Jagga S, Lee S-S, Nam J-S. Interplay between cartilage and subchondral bone contributing to pathogenesis of osteoarthritis. Int J Mol Sci 2013;14(10):19805-30. [PMID: 24084727 DOI: 10.3390/ijms141019805]
- Donell S. Subchondral bone remodelling in osteoarthritis. EFORT Open Rev 2019;4(6):221-9. [PMID: 31210964 DOI: 10.1302/2058-5241.4.180102]
- Fan X, Wu X, Crawford R, Xiao Y, Prasadam I. Macro, micro, and molecular. changes of the osteochondral interface in osteoarthritis development. Front Cell and Dev Biol 2021;9:659654. [PMID: 34041240 DOI: 10.3389/fcell.2021.659654]
- Sartori M, Pagani S, Ferrari A, Costa V, Carina V, et al. A new bi-layered scaffold for osteochondral tissue regeneration: In vitro and in vivo preclinical investigations. Mater Sci Eng C Mater Biol Appl 2017;70(Pt 1):101-11. [PMID: 27770869 DOI: 10.1016/j.msec.2016.08.027]
- Qasim M, Le NXT, Nguyen TPT, Chae DS, Park S-J, et al. Nanohybrid biodegradable scaffolds for TGF-β3 release for the chondrogenic differentiation of human mesenchymal stem cells. Int J Pharm 2020;581:119248. [PMID: 32240810 DOI: 10.1016/j.ijpharm.2020.119248]
- Fu H-D, Wang H-R, Li D-H. BMP-7 accelerates the differentiation of rabbit mesenchymal stem cells into cartilage through the Wnt/β-catenin pathway. Exp Ther Med 2017;14(6):5424-8. [PMID: 29285071 DOI: 10.3892/etm.2017.5210]
- Li J, Wang X, Ruan G, Zhu Z, Ding C. Sprifermin: a recombinant human fibroblast growth factor 18 for the treatment of knee osteoarthritis. Expert Opin Investig Drugs 2021;30(9):923-30. [PMID: 34427483 DOI: 10.1080/13543784.2021.1972970]
- Hu N, Gong X, Yin S, Li Q, Chen H, et al. Saxagliptin suppresses degradation of type II collagen and aggrecan in primary human chondrocytes: a therapeutic implication in osteoarthritis. Artif Cells Nanomed Biotechnol 2019;47(1):3239-45. [PMID: 31364869 DOI: 10.1080/21691401.2019.1647223]
- Shi J, Chi S, Xue J, Yang J, Li F, et al. Emerging role and therapeutic implication of Wnt signaling pathways in autoimmune diseases. J Immunol Res 2016;2016:9392132. [PMID: 27110577 DOI: 10.1155/2016/9392132]
- Xiao P, Zhu Z, Du C, Zeng Y, Liao J, et al. Silencing Smad7 potentiates BMP2-induced chondrogenic differentiation and inhibits endochondral ossification in human synovial-derived mesenchymal stromal cells. Stem Cell Res Ther 2021;12(1):132. [PMID: 33588941 DOI: 10.1186/s13287-021-02202-2]
- Coimbra IB, Jimenez SA, Hawkins DF, Piera-Velazquez S, Stokes DG. Hypoxia inducible factor-1 alpha expression in human normal and osteoarthritic chondrocytes. Osteoarthritis Cartilage 2004;12(4):336-45. [PMID: 15023385 DOI: 10.1016/j.joca.2003.12.005]
- Bechtold TE, Saunders C, Decker RS, Um H-B, Cottingham N, et al. Osteophyte formation and matrix mineralization in a TMJ osteoarthritis mouse model are associated with ectopic hedgehog signaling. Matrix Biol 2016;52-54:339-54. [PMID: 26945615 DOI: 10.1016/j.matbio.2016.03.001]
- Wang X-P, Xie W-P, Bi Y-F, Wang B-A, Song H-B, et al. Quercetin suppresses apoptosis of chondrocytes induced by IL-1β via inactivation of p38 MAPK signaling pathway. Exp Ther Med 2021;21(5):468. [PMID: 33767763 DOI: 10.3892/etm.2021.9899]
- Duan X, Cai L, Pham CTN, Abu-Amer Y, Pan H, et al. Amelioration of posttraumatic osteoarthritis in mice using intraarticular silencing of periostin via nanoparticle-based small interfering RNA. Arthritis Rheumatol 2021;73(12):2249-60. [PMID: 33982891 DOI: 10.1002/art.41794]
- Zhang B, Huang J, Narayan RJ. Gradient scaffolds for osteochondral tissue engineering and regeneration. J Mater Chem B 2020;8(36):8149-70. [PMID: 32776030 DOI: 10.1039/d0tb00688b]
- Bektas C, Mao Y. Hydrogel microparticles for bone regeneration. Gels 2023;10(1):28. [PMID: 38247752 DOI: 10.3390/gels10010028]
- Johnson AR, Forster SP, White D, Terife G, Lowinger M, et al. Drug eluting implants in pharmaceutical development and clinical practice. Expert Opin Drug Deliv 2021;18(5):577-93. [PMID: 33275066 DOI: 10.1080/17425247.2021.1856072]
- Oliveira ÉR, Nie L, Podstawczyk D, Allahbakhsh A, Ratnayake J, et al. Advances in growth factor delivery for bone tissue engineering. Int J Mol Sci 2021;22(2):903. [PMID: 33477502 DOI: 10.3390/ijms22020903]
- Szwed-Georgiou A, Płociński P, Kupikowska-Stobba B, Urbaniak MM, Rusek-Wala P, et al. Bioactive materials for bone regeneration: biomolecules and delivery systems. ACS Biomater Sci Eng 2023;9(9):5222-54. [PMID: 37585562 DOI: 10.1021/acsbiomaterials.3c00609]
- Vo TN, Kasper FK, Mikos AG. Strategies for controlled delivery of growth factors and cells for bone regeneration. Adv Drug Deliv Rev 2012;64(12):1292-309. [PMID: 22342771 DOI: 10.1016/j.addr.2012.01.016]
- Blackwood KA, Bock N, Dargaville TR, Ann Woodruff M. Scaffolds for growth factor delivery as applied to bone tissue engineering. Int J Polymer Sci 2012;2012(1):1-25. [DOI: 10.1155/2012/174942]
- Yan W, Xu X, Xu Q, Sun Z, Lv Z, et al. An injectable hydrogel scaffold with kartogenin-encapsulated nanoparticles for porcine cartilage regeneration: a 12-month follow-up study. Am J Sports Med 2020;48(13):3233-44. [PMID: 33026830 DOI: 10.1177/0363546520957346]
- Park YB, Ha CW, Kim JA, Han WJ, Rhim JH, et al. Single-stage cell-based cartilage repair in a rabbit model: cell tracking and in vivo chondrogenesis of human umbilical cord blood-derived mesenchymal stem cells and hyaluronic acid hydrogel composite. Osteoarthritis and Cartilage 2017;25(4):570-80. [PMID: 27789339 DOI: 10.1016/j.joca.2016.10.012]
- Hu X, Wang Y, Tan Y, Wang J, Liu H, et al. A difunctional regeneration scaffold for knee repair based on aptamer-directed cell recruitment. Adv Mater 2017;29(15). [PMID: 28185322 DOI: 10.1002/adma.201605235]
- Beigi M-H, Atefi A, Ghanaei H-R, Labbaf S, Ejeian F, et al. Activated platelet-rich plasma improves cartilage regeneration using adipose stem cells encapsulated in a 3D alginate scaffold. J Tissue Eng Regen Med 2018;12(6):1327-38. [PMID: 29522657 DOI: 10.1002/term.2663]
- Zhu Y, Kong L, Farhadi F, Xia W, Chang J, et al. An injectable continuous stratified structurally and functionally biomimetic construct for enhancing osteochondral regeneration. Biomaterials 2019;192:149-58. [PMID: 30448699 DOI: 10.1016/j.biomaterials.2018.11.017]
- Stefani RM, Lee AJ, Tan AR, Halder SS, Hu Y, et al. Sustained low-dose dexamethasone delivery via a PLGA microsphere-embedded agarose implant for enhanced osteochondral repair. Acta Biomater 2020;102:326-40. [PMID: 31805408 DOI: 10.1016/j.actbio.2019.11.052]
- Rajagopal K, Ramesh S, Walter NM, Arora A, Katti DS, et al. In vivo cartilage regeneration in a multi-layered articular cartilage architecture mimicking scaffold. Bone Joint Res 2020;9(9):601-12. [PMID: 33014353 DOI: 10.1302/2046-3758.99.BJR-2019-0210.R2]
- Itha R, Vaishya R, Vaish A, Migliorini F. Management of chondral and osteochondral lesions of the hip: a comprehensive review. Orthopadie (Heidelb) 2024;53(1):23-38. [PMID: 37815635 DOI: 10.1007/s00132-023-04444-9]
- Liu B, Zhao Y, Zhu T, Gao S, Ye K, et al. Biphasic double-network hydrogel with compartmentalized loading of bioactive glass for osteochondral defect repair. Front Bioeng Biotechnol 2020;8:752. [PMID: 32714919 DOI: 10.3389/fbioe.2020.00752]
- Boyer C, Réthoré G, Weiss P, d’Arros C, Lesoeur J, et al. A self-setting hydrogel of silylated chitosan and cellulose for the repair of osteochondral defects: from in vitro characterization to preclinical evaluation in dogs. Front Bioeng Biotechnol 2020;8:23. [PMID: 32117912 DOI: 10.3389/fbioe.2020.00023]
- Gugjoo MB, Amarpal, Abdelbaset-Ismail A, Aithal HP, Kinjavdekar P, et al. Allogeneic mesenchymal stem cells and growth factors in gel scaffold repair osteochondral defect in rabbit. Regen Med 2020;15(2):1261-75. [PMID: 32154762 DOI: 10.2217/rme-2018-0138]
- Gong L, Li J, Zhang J, Pan Z, Liu Y, et al. An interleukin-4-loaded bi-layer 3D printed scaffold promotes osteochondral regeneration. Acta Biomater 2020;117:246-60. [PMID: 33007484 DOI: 10.1016/j.actbio.2020.09.039]
- Gao J, Ding X, Yu X, Chen X, Zhang X, et al. Cell-free bilayered porous scaffolds for osteochondral regeneration fabricated by continuous 3D-printing using nascent physical hydrogel as ink. Adv Healthc Mater 2021;10(3):e2001404. [PMID: 33225617 DOI: 10.1002/adhm.202001404]
- Zhao Y, Ding X, Dong Y, Sun X, Wang L, et al. Role of the calcified cartilage layer of an integrated trilayered silk fibroin scaffold used to regenerate osteochondral defects in rabbit knees. ACS Biomater Sci Eng 2020;6(2):1208-16. [PMID: 33464868 DOI: 10.1021/acsbiomaterials.9b01661]
- Wu Y, Yang Z, Denslin V, Ren X, Lee CS, et al. Repair of osteochondral defects with predifferentiated mesenchymal stem cells of distinct phenotypic character derived from a nanotopographic platform. Am J Sports Med 2020;48(7):1735-47. [PMID: 32191492 DOI: 10.1177/0363546520907137]
- Rezvani Ghomi E, Nourbakhsh N, Akbari Kenari M, Zare M, Ramakrishna S. Collagen-based biomaterials for biomedical applications. J Biomed Mater Res B Appl Biomater 2021;109(12):1986-99. [PMID: 34028179 DOI: 10.1002/jbm.b.34881]
- Song J, Leeuwenburgh SC. Sustained delivery of biomolecules from gelatin carriers for applications in bone regeneration. Ther Deliv 2014;5(8):943-58. [PMID: 25337650 DOI: 10.4155/tde.14.42]
- Notario-Pérez F, Martín-Illana A, Cazorla-Luna R, Ruiz-Caro R, Veiga MD. Applications of chitosan in surgical and post-surgical materials. Marine Drugs 2022;20(6):396. [PMID: 35736199 DOI: 10.3390/md20060396]
- Deng Y, Ren J, Chen G, Li G, Wu X, et al. Injectable in situ cross-linking chitosan-hyaluronic acid based hydrogels for abdominal tissue regeneration. Sci Rep 2017;7(1):2699. [PMID: 28578386 DOI: 10.1038/s41598-017-02962-z]
- Zhou Z, Cui J, Wu S, Geng Z, Su J. Silk fibroin-based biomaterials for cartilage/osteochondral repair. Theranostics 2022;12(11):5103-24. [PMID: 35836802 DOI: 10.7150/thno.74548]
- Ribeiro VP, Pina S, Costa JB, Cengiz IF, García-Fernández L, et al. Enzymatically cross-linked silk fibroin-based hierarchical scaffolds for osteochondral regeneration. ACS Appl Mater Interfaces 2019;11(4):3781-99. [PMID: 30609898 DOI: 10.1021/acsami.8b21259]
- Yan L-P, Silva-Correia J, Oliveira MB, Vilela C, Pereira H, et al. Bilayered silk/silk-nanoCaP scaffolds for osteochondral tissue engineering: In vitro and in vivo assessment of biological performance. Acta Biomater 2015;12:227-41. [PMID: 25449920 DOI: 10.1016/j.actbio.2014.10.021]
- Yin H-M, Li X, Wang P, Ren Y, Liu W, et al. Role of HA and BG in engineering poly(ε-caprolactone) porous scaffolds for accelerating cranial bone regeneration. J Biomed Mater Res A 2019;107(3):654-62. [PMID: 30474348 DOI: 10.1002/jbm.a.36584]
- Xu N, Lu D, Qiang L, Liu Y, Yin D, et al. 3D-Printed composite bioceramic scaffolds for bone and cartilage integrated regeneration. ACS Omega 2023;8(41):37918-26. [PMID: 37867636 DOI: 10.1021/acsomega.3c03284]
- Baker BM, Shah RP, Silverstein AM, Esterhai JL, Burdick JA, et al. Sacrificial nanofibrous composites provide instruction without impediment and enable functional tissue formation. Proc Natl Acad Sci USA 2012;109(35):14176-81. [PMID: 22872864 DOI: 10.1073/pnas.1206962109]
- Xing J, Zhang M, Liu X, Wang C, Xu N, et al. Multi-material electrospinning: from methods to biomedical applications. Mater Today Bio 2023;21:100710. [PMID: 37545561 DOI: 10.1016/j.mtbio.2023.100710]
- Ondrésik M, Azevedo Maia FR, da Silva Morais A, Gertrudes AC, Dias Bacelar AH, et al. Management of knee osteoarthritis. Current status and future trends. Biotechnol Bioeng 2017;114(4):717-39. [PMID: 27618194 DOI: 10.1002/bit.26182]
- Dai Y, Gao Z, Ma L, Wang D, Gao C. Cell-free HA-MA/PLGA scaffolds with radially oriented pores for in situ inductive regeneration of full thickness cartilage defects. Macromol Biosci 2016;16(11):1632-42. [PMID: 27456077 DOI: 10.1002/mabi.201600218]
- Preethi Soundarya S, Haritha Menon A, Viji Chandran S, Selvamurugan N. Bone tissue engineering: scaffold preparation using chitosan and other biomaterials with different design and fabrication techniques. Int J Biol Macromol 2018;119:1228-39. [PMID: 30107161 DOI: 10.1016/j.ijbiomac.2018.08.056]
- Wu Y, Zhou L, Li Y, Lou X. Osteoblast-derived extracellular matrix coated PLLA/silk fibroin composite nanofibers promote osteogenic differentiation of bone mesenchymal stem cells. J Biomed Mater Res A 2022;110(3):525-34. [PMID: 34494712 DOI: 10.1002/jbm.a.37302]
- Chen K, Li Y, Li Y, Pan W, Tan G. Silk fibroin combined with electrospinning as a promising strategy for tissue regeneration. Macromol Biosci 2023;23(2):e2200380. [PMID: 36409150 DOI: 10.1002/mabi.202200380]
- Kang K, Koh Y, Son J, Yeom JS, Park J, et al. Biomechanical evaluation of pedicle screw fixation system in spinal adjacent levels using polyetheretherketone, carbon-fiber-reinforced polyetheretherketone, and traditional titanium as rod materials. Compos B Eng 2017;130:248-56. [DOI: 10.1016/j.compositesb.2017.07.052]
- Wang D, Chen M-W, Wei Y-J, Geng W-B, Hu Y, et al. Construction of Wogonin nanoparticle-containing strontium-doped nanoporous structure on titanium surface to promote osteoporosis fracture repair. Adv Healthc Mater 2022;11(21):e2201405. [PMID: 36048734 DOI: 10.1002/adhm.202201405]
- Yang K, Zhou C, Fan H, Fan Y, Jiang Q, et al. Bio-functional design, application and trends in metallic biomaterials. Int J Mol Sci 2017;19(1):24. [PMID: 29271916 DOI: 10.3390/ijms19010024]
- Li P, Dai J, Li Y, Alexander D, Čapek J, et al. Zinc based biodegradable metals for bone repair and regeneration: bioactivity and molecular mechanisms. Mater Today Bio 2023;25:100932. [PMID: 38298560 DOI: 10.1016/j.mtbio.2023.100932]
- Nie S, Chen J, Liu C, Zhou C, Zhao J, et al. Effects of extract solution from magnesium alloys supplemented with different compositions of rare earth elements on in vitro epithelial and osteoblast progenitor cells. Front Bioeng Biotechnol 2023;11:1138675. [PMID: 37251562 DOI: 10.3389/fbioe.2023.1138675]
- Brokesh AM, Gaharwar AK. Inorganic biomaterials for regenerative medicine. ACS Appl Mater Interfaces 2020;12(5):5319-44. [PMID: 31989815 DOI: 10.1021/acsami.9b17801]
- Kim J, Kim S, Song I. Octacalcium phosphate, a promising bone substitute material: a narrative review. J Yeungnam Med Sci 2024;41(1):4-12. [PMID: 37157781 DOI: 10.12701/jyms.2023.00010]
- Lin H, Zhang L, Zhang Q, Wang Q, Wang X, et al. Mechanism and application of 3D-printed degradable bioceramic scaffolds for bone repair. Biomater Sci 2023;11(21):7034-50. [PMID: 37782081 DOI: 10.1039/d3bm01214j]
- Ebrahimi M, Botelho MG, Dorozhkin SV. Biphasic calcium phosphates bioceramics (HA/TCP): concept, physicochemical properties and the impact of standardization of study protocols in biomaterials research. Mater Sci Eng C Mater Biol Appl 2017;71:1293-312. [PMID: 27987685 DOI: 10.1016/j.msec.2016.11.039]
- El-Rashidy AA, Roether JA, Harhaus L, Kneser U, Boccaccini AR. Regenerating bone with bioactive glass scaffolds: a review of in vivo studies in bone defect models. Acta Biomater 2017;62:1-28. [PMID: 28844964 DOI: 10.1016/j.actbio.2017.08.030]
- Granel H, Bossard C, Nucke L, Wauquier F, Rochefort GY, et al. Optimized bioactive glass: the quest for the bony graft. Adv Healthc Mater 2019;8(11):e1801542. [PMID: 30941912 DOI: 10.1002/adhm.201801542]
- Jones JR. Review of bioactive glass: from Hench to hybrids. Acta Biomater 2013;9(1):4457-86. [PMID: 22922331 DOI: 10.1016/j.actbio.2012.08.023]
- Lin R, Deng C, Li X, Liu Y, Zhang M, et al. Copper-incorporated bioactive glass-ceramics inducing anti-inflammatory phenotype and regeneration of cartilage/bone interface. Theranostics 2019;9(21):6300-13. [PMID: 31534552 DOI: 10.7150/thno.36120]
- Socci MC, Rodríguez G, Oliva E, Fushimi S, Takabatake K, et al. Polymeric materials, advances and applications in tissue engineering: a review. Bioengineering (Basel) 2023;10(2):218. [PMID: 36829712 DOI: 10.3390/bioengineering10020218]
- Tsiklin IL, Shabunin AV, Kolsanov AV, Volova LT. In vivo bone tissue engineering strategies: advances and prospects. Polymers 2022;14(15):3222. [PMID: 35956735 DOI: 10.3390/polym14153222]
- Ramzan F, Salim A, Khan I. Osteochondral tissue engineering dilemma: scaffolding trends in regenerative medicine. Stem Cell Rev Rep 2023;19(6):1615-34. [PMID: 37074547 DOI: 10.1007/s12015-023-10545-x]
- Ribeiro VP, Pina S, Oliveira JM, Reis RL. Silk fibroin-based hydrogels and scaffolds for osteochondral repair and regeneration. Adv Exp Med Biol 2018;1058:305-25. [PMID: 29691828 DOI: 10.1007/978-3-319-76711-6_14]
- Zhou L, Gjvm VO, Malda J, Stoddart MJ, Lai Y, et al. Innovative tissue-engineered strategies for osteochondral defect repair and regeneration: current progress and challenges. Adv Healthc Mater 2020;9(23):e2001008. [PMID: 33103381 DOI: 10.1002/adhm.202001008]
- Asghari F, Samiei M, Adibkia K, Akbarzadeh A, Davaran S. Biodegradable and biocompatible polymers for tissue engineering application: a review. Artif Cells Nanomed Biotechnol 2017;45(2):185-92. [PMID: 26923861 DOI: 10.3109/21691401.2016.1146731]
- Stratton S, Shelke NB, Hoshino K, Rudraiah S, Kumbar SG. Bioactive polymeric scaffolds for tissue engineering. Bioact Mater 2016;1(2):93-108. [PMID: 28653043 DOI: 10.1016/j.bioactmat.2016.11.001]
- Yazdimamaghani M, Razavi M, Vashaee D, Moharamzadeh K, Boccaccini AR, et al. Porous magnesium-based scaffolds for tissue engineering. Mater Sci Eng C Mater Biol Appl 2017;71:1253-66. [PMID: 27987682 DOI: 10.1016/j.msec.2016.11.027]
- Wang J-L, Xu J-K, Hopkins C, Chow DH-K, Qin L. Biodegradable magnesium-based implants in orthopedics-a general review and perspectives. Adv Sci (Weinh) 2020;7(8):1902443. [PMID: 32328412 DOI: 10.1002/advs.201902443]
- Wang L, You X, Zhang L, Zhang C, Zou W. Mechanical regulation of bone remodeling. Bone Res 2022;10(1):16. [PMID: 35181672 DOI: 10.1038/s41413-022-00190-4]
- Deng ZH, Li YS, Gao X, Lei GH, Huard J. Bone morphogenetic proteins for articular cartilage regeneration. Osteoarthritis Cartilage 2018;26(9):1153-61. [PMID: 29580979 DOI: 10.1016/j.joca.2018.03.007]
- van der Kraan PM. The changing role of TGFβ in healthy, ageing and osteoarthritic joints. Nat Rev Rheumatol 2017;13(3):155-63. [PMID: 28148919 DOI: 10.1038/nrrheum.2016.219]
- Vinatier C, Mrugala D, Jorgensen C, Guicheux J, Noël D. Cartilage engineering: a crucial combination of cells, biomaterials and biofactors. Trends Biotechnol 2009;27(5):307-14. [PMID: 19329205 DOI: 10.1016/j.tibtech.2009.02.005]
- Ji X, Shao H, Li X, Ullah MW, Luo G, et al. Injectable immunomodulation-based porous chitosan microspheres/HPCH hydrogel composites as a controlled drug delivery system for osteochondral regeneration. Biomater 2022;285:121530. [PMID: 35504181 DOI: 10.1016/j.biomaterials.2022.121530]
- Wu M, Chen G, Li Y-P. TGF-β and BMP signaling in osteoblast, skeletal development, and bone formation, homeostasis and disease. Bone Res 2016;4:16009. [PMID: 27563484 DOI: 10.1038/boneres.2016.9]
- Li YP, Chen W, Liang Y, Li E, Stashenko P. Atp6i-deficient mice exhibit severe osteopetrosis due to loss of osteoclast-mediated extracellular acidification. Nat Genet 1999;23(4):447-51. [PMID: 10581033 DOI: 10.1038/70563]
- Chen W, Yang S, Abe Y, Li M, Wang Y, et al. Novel pycnodysostosis mouse model uncovers cathepsin K function as a potential regulator of osteoclast apoptosis and senescence. Hum Mol Genet 2007;16(4):410-23. [PMID: 17210673 DOI: 10.1093/hmg/ddl474]
- Lu S, Lam J, Trachtenberg JE, Lee EJ, Seyednejad H, et al. Dual growth factor delivery from bilayered, biodegradable hydrogel composites for spatially-guided osteochondral tissue repair. Biomaterials 2014;35(31):8829-39. [PMID: 25047629 DOI: 10.1016/j.biomaterials.2014.07.006]
- Kim K, Lam J, Lu S, Spicer PP, Lueckgen A, et al. Osteochondral tissue regeneration using a bilayered composite hydrogel with modulating dual growth factor release kinetics in a rabbit model. J Control Release 2013;168(2):166-78. [PMID: 23541928 DOI: 10.1016/j.jconrel.2013.03.013]
- Shi Z, Zhong Q, Chen Y, Gao J, Pan X, et al. Nanohydroxyapatite, nanosilicate-reinforced injectable, and biomimetic gelatin-methacryloyl hydrogel for bone tissue engineering. Int J Nanomedicine 2021;16:5603-19. [PMID: 34429602 DOI: 10.2147/IJN.S321387]
- Kwon JY, Lee SH, Na H-S, Jung K, Choi J, et al. Kartogenin inhibits pain behavior, chondrocyte inflammation, and attenuates osteoarthritis progression in mice through induction of IL-10. Sci Rep 2018;8(1):13832. [PMID: 30218055 DOI: 10.1038/s41598-018-32206-7]
- Cai J-Y, Zhang L, Chen J, Chen S-Y. Kartogenin and its application in regenerative medicine. Curr Med Sci 2019;39(1):16-20. [PMID: 30868486 DOI: 10.1007/s11596-019-1994-6]
- Shi D, Xu X, Ye Y, Song K, Cheng Y, et al. Photo-cross-linked scaffold with kartogenin-encapsulated nanoparticles for cartilage regeneration. ACS Nano 2016;10(1):1292-9. [PMID: 26757419 DOI: 10.1021/acsnano.5b06663]
- Xu J, Feng Q, Lin S, Yuan W, Li R, et al. Injectable stem cell-laden supramolecular hydrogels enhance in situ osteochondral regeneration via the sustained co-delivery of hydrophilic and hydrophobic chondrogenic molecules. Biomaterials 2019;210:51-61. [PMID: 31075723 DOI: 10.1016/j.biomaterials.2019.04.031]
- Johnson K, Zhu S, Tremblay MS, Payette JN, Wang J, et al. A stem cell-based approach to cartilage repair. Science 2012;336(6082):717-21. [PMID: 22491093 DOI: 10.1126/science.1215157]
- Nagao M, Hamilton JL, Kc R, Berendsen AD, Duan X, et al. Vascular endothelial growth factor in cartilage development and osteoarthritis. Sci Rep 2017;7(1):13027. [PMID: 29026147 DOI: 10.1038/s41598-017-13417-w]
- Faissner S, Gold R. Efficacy and safety of multiple sclerosis drugs approved since 2018 and future developments. CNS Drugs 2022;36(8):803-17. [PMID: 35869335 DOI: 10.1007/s40263-022-00939-9]
- Pinho-Gomes A-C, Cairns J. Evaluation of advanced therapy medicinal products by the National Institute for Health and Care Excellence (NICE): an updated review. Pharmacoecon Open 2022;6(2):147-67. [PMID: 34415514 DOI: 10.1007/s41669-021-00295-2]
- Magni A, Agostoni P, Bonezzi C, Massazza G, Menè P, et al. Management of osteoarthritis: expert opinion on NSAIDs. Pain Ther 2021;10(2):783-808. [PMID: 33876393 DOI: 10.1007/s40122-021-00260-1]
- Solomon DH, Husni ME, Wolski KE, Wisniewski LM, Borer JS, et al. Differences in safety of nonsteroidal antiinflammatory drugs in patients with osteoarthritis and patients with rheumatoid arthritis: a randomized clinical trial. Arthritis Rheumatol 2018;70(4):537-46. [PMID: 29266879 DOI: 10.1002/art.40400]
- Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284(10):1247-55. [PMID: 10979111 DOI: 10.1001/jama.284.10.1247]
- Zhang W, Chen R, Xu X, Zhu L, Liu Y, et al. Construction of biocompatible hydrogel scaffolds with a long-term drug release for facilitating cartilage repair. Front Pharmacol 2022;13:922032. [PMID: 35784682 DOI: 10.3389/fphar.2022.922032]
- Perciani CT, MacParland SA. Lifting the veil on macrophage diversity in tissue regeneration and fibrosis. Sci Immunol 2019;4(40):eaaz0749. [PMID: 31604845 DOI: 10.1126/sciimmunol.aaz0749]
- Oishi Y, Manabe I. Macrophages in inflammation, repair and regeneration. Int Immunol 2018;30(11):511-28. [PMID: 30165385 DOI: 10.1093/intimm/dxy054]
- Brown BN, Ratner BD, Goodman SB, Amar S, Badylak SF. Macrophage polarization: an opportunity for improved outcomes in biomaterials and regenerative medicine. Biomaterials 2012;33(15):3792-802. [PMID: 22386919 DOI: 10.1016/j.biomaterials.2012.02.034]
- Chang S-H, Lin Y-Y, Wu G-J, Huang C-H, Tsai GJ. Effect of chitosan molecular weight on anti-inflammatory activity in the RAW 264.7 macrophage model. Int J Biol Macromol 2019;131:167-75. [PMID: 30771390 DOI: 10.1016/j.ijbiomac.2019.02.066]
- Zhang W, Qi X, Zhao Y, Liu Y, Xu L, et al. Study of injectable Blueberry anthocyanins-loaded hydrogel for promoting full-thickness wound healing. Int J Pharm 2020;586:119543. [PMID: 32561307 DOI: 10.1016/j.ijpharm.2020.119543]
- Stenson WF, Ciorba MA. Nonmicrobial activation of TLRs controls intestinal growth, wound repair, and radioprotection. Front Immunol 2021;11:617510. [PMID: 33552081 DOI: 10.3389/fimmu.2020.617510]
- Jiang G, Li S, Yu K, He B, Hong J, et al. A 3D-printed PRP-GelMA hydrogel promotes osteochondral regeneration through M2 macrophage polarization in a rabbit model. Acta Biomater 2021;128:150-62. [PMID: 33894346 DOI: 10.1016/j.actbio.2021.04.010]
- Yang Z, Wang B, Liu W, Li X, Liang K, et al. In situ self-assembled organoid for osteochondral tissue regeneration with dual functional units. Bioact Mater 2023;27:200-15. [PMID: 37096194 DOI: 10.1016/j.bioactmat.2023.04.002]
- Pereira TV, Jüni P, Saadat P, Xing D, Yao L, et al. Viscosupplementation for knee osteoarthritis: systematic review and meta-analysis. BMJ 2022;378:e069722. [PMID: 36333100 DOI: 10.1136/bmj-2022-069722]
- Bolduc JA, Collins JA, Loeser RF. Reactive oxygen species, aging and articular cartilage homeostasis. Free Radic Biol Med 2019;132:73-82. [PMID: 30176344 DOI: 10.1016/j.freeradbiomed.2018.08.038]
- Zhao Y, Song S, Wang D, Liu H, Zhang J, et al. Nanozyme-reinforced hydrogel as a H2O2-driven oxygenerator for enhancing prosthetic interface osseointegration in rheumatoid arthritis therapy. Nat Commun 2022;13(1):6758. [PMID: 36351899 DOI: 10.1038/s41467-022-34481-5]
- Zhang W, Zhang Y, Li X, Cao Z, Mo Q, et al. Multifunctional polyphenol-based silk hydrogel alleviates oxidative stress and enhances endogenous regeneration of osteochondral defects. Mater Today Bio 2022;14:100251. [PMID: 35469254 DOI: 10.1016/j.mtbio.2022.100251]
- Temple-Wong MM, Raleigh AR, Frisbie DD, Sah RL, McIlwraith CW. Effects of an articular cartilage lubrication with a viscosupplement in vitro and in vivo following osteochondral fractures in horses. Am J Vet Res 2021;82(8):611-8. [PMID: 34296945 DOI: 10.2460/ajvr.82.8.611]
- Terencio MC, Ferrándiz ML, Carceller MC, Ruhí R, Dalmau P, et al. Chondroprotective effects of the combination chondroitin sulfate-glucosamine in a model of osteoarthritis induced by anterior cruciate ligament transection in ovariectomised rats. Biomed Pharmacothe r2016;79:120-8. [PMID: 27044820 DOI: 10.1016/j.biopha.2016.02.005]
- You F, Chen X, Cooper DML, Chang T, Eames BF. Homogeneous hydroxyapatite/alginate composite hydrogel promotes calcified cartilage matrix deposition with potential for three-dimensional bioprinting. Biofabrication 2018;11(1):015015. [PMID: 30524110 DOI: 10.1088/1758-5090/aaf44a]
- Lutolf MP, Gilbert PM, Blau HM. Designing materials to direct stem-cell fate. Nature 2009;462(7272):433-41. [PMID: 19940913 DOI: 10.1038/nature08602]
- Nazempour A, Van Wie BJ. Chondrocytes, mesenchymal stem cells, and their combination in articular cartilage regenerative medicine. Ann Biomed Eng 2016;44(5):1325-54. [PMID: 26987846 DOI: 10.1007/s10439-016-1575-9]
- Li P, Fu L, Liao Z, Peng Y, Ning C, et al. Chitosan hydrogel/3D-printed poly(ε-caprolactone) hybrid scaffold containing synovial mesenchymal stem cells for cartilage regeneration based on tetrahedral framework nucleic acid recruitment. Biomaterials 2021;278:121131. [PMID: 34543785 DOI: 10.1016/j.biomaterials.2021.121131]
- Yang M, Deng R-H, Yuan F-Z, Zhang J-Y, Zhang Z-N, et al. Immunomodulatory PEG-CRGD hydrogels promote chondrogenic differentiation of PBMSCs. Pharmaceutics 2022;14(12):2622. [PMID: 36559119 DOI: 10.3390/pharmaceutics14122622]
- Minardi S, Corradetti B, Taraballi F, Byun JH, Cabrera F, et al. IL-4 release from a biomimetic scaffold for the temporally controlled modulation of macrophage response. Ann Biomed Eng 2016;44(6):2008-19. [PMID: 26951461 DOI: 10.1007/s10439-016-1580-z]
- Zhao Y, Feng X, Zhao Z, Song Z, Wang W, et al. Interleukin-4-loaded heparin hydrogel regulates macrophage polarization to promote osteogenic differentiation. ACS Biomater Sci Eng 2024;10(9):5774-83. [PMID: 39198394 DOI: 10.1021/acsbiomaterials.4c00589]
- Zhang W, Zhang Y, Zhang A, Ling C, Sheng R, et al. Enzymatically crosslinked silk-nanosilicate reinforced hydrogel with dual-lineage bioactivity for osteochondral tissue engineering. Mater Sci Eng C Mater Biol Appl 2021;127:112215. [PMID: 34225867 DOI: 10.1016/j.msec.2021.112215]
- Zhu X, Chen T, Feng B, Weng J, Duan K, et al. Biomimetic bacterial cellulose-enhanced double-network hydrogel with excellent mechanical properties applied for the osteochondral defect repair. ACS Biomater Sci Eng 2018;4(10):3534-44. [PMID: 33465904 DOI: 10.1021/acsbiomaterials.8b00682]
- Singh NK, Lee DS. In situ gelling pH- and temperature-sensitive biodegradable block copolymer hydrogels for drug delivery. J Control Release 2014;193:214-27. [PMID: 24815421 DOI: 10.1016/j.jconrel.2014.04.056]
- George MN, Liu X, Miller AL 2nd, Zuiker E, Xu H, et al. Injectable pH-responsive adhesive hydrogels for bone tissue engineering inspired by the underwater attachment strategy of marine mussels. Biomater Adv 2022;133:112606. [PMID: 35525750 DOI: 10.1016/j.msec.2021.112606]
- Nelson DM, Ma Z, Leeson CE, Wagner WR. Extended and sequential delivery of protein from injectable thermoresponsive hydrogels. J Biomed Mater Res A 2012;100(3):776-85. [PMID: 22237975 DOI: 10.1002/jbm.a.34015]
- Park K-S, Kim B-J, Lih E, Park W, Lee S-H, et al. Versatile effects of magnesium hydroxide nanoparticles in PLGA scaffold-mediated chondrogenesis. Acta Biomater 2018;73:204-16. [PMID: 29673840 DOI: 10.1016/j.actbio.2018.04.022]
- Radhakrishnan J, Manigandan A, Chinnaswamy P, Subramanian A, Sethuraman S. Gradient nano-engineered in situ forming composite hydrogel for osteochondral regeneration. Biomaterials 2018;162:82-98. [PMID: 29438883 DOI: 10.1016/j.biomaterials.2018.01.056]
- Radhakrishnan J, Subramanian A, Sethuraman S. Injectable glycosaminoglycan-protein nano-complex in semi-interpenetrating networks: a biphasic hydrogel for hyaline cartilage regeneration. Carbohydr Polym 2017;175:63-74. [PMID: 28917911 DOI: 10.1016/j.carbpol.2017.07.063]
- Oliveira JM, Kotobuki N, Tadokoro M, Hirose M, Mano JF, et al. Ex vivo culturing of stromal cells with dexamethasone-loaded carboxymethylchitosan/poly(amidoamine) dendrimer nanoparticles promotes ectopic bone formation. Bone 2010;46(5):1424-35. [PMID: 20152952 DOI: 10.1016/j.bone.2010.02.007]
- Yilgor P, Tuzlakoglu K, Reis RL, Hasirci N, Hasirci V. Incorporation of a sequential BMP-2/BMP-7 delivery system into chitosan-based scaffolds for bone tissue engineering. Biomaterials 2009;30(21):3551-9. [PMID: 19361857 DOI: 10.1016/j.biomaterials.2009.03.024]
- Lim SM, Oh SH, Lee HH, Yuk SH, Im GI, et al. Dual growth factor-releasing nanoparticle/hydrogel system for cartilage tissue engineering. J Mater Sci Mater Med 2010;21(9):2593-600. [PMID: 20577785 DOI: 10.1007/s10856-010-4118-1]
- Castro NJ, O’Brien J, Zhang LG. Integrating biologically inspired nanomaterials and table-top stereolithography for 3D printed biomimetic osteochondral scaffolds. Nanoscale 2015;7(33):14010-22. [PMID: 26234364 DOI: 10.1039/c5nr03425f]
- Wang H, Bongio M, Farbod K, Nijhuis AWG, van den Beucken J, et al. Development of injectable organic/inorganic colloidal composite gels made of self-assembling gelatin nanospheres and calcium phosphate nanocrystals. Acta Biomater 2014;10(1):508-19. [PMID: 24012604 DOI: 10.1016/j.actbio.2013.08.036]
- Wang H, Boerman OC, Sariibrahimoglu K, Li Y, Jansen JA, et al. Comparison of micro- vs. nanostructured colloidal gelatin gels for sustained delivery of osteogenic proteins: bone morphogenetic protein-2 and alkaline phosphatase. Biomaterials 2012;33(33):8695-703. [PMID: 22922022 DOI: 10.1016/j.biomaterials.2012.08.024]
- Wang H, Zou Q, Boerman OC, Nijhuis AWG, Jansen JA, et al. Combined delivery of BMP-2 and bFGF from nanostructured colloidal gelatin gels and its effect on bone regeneration in vivo. J Control Release 2013;166(2):172-81. [PMID: 23266450 DOI: 10.1016/j.jconrel.2012.12.015]
- Abdal Dayem A, Lee SB, Cho S-G. The impact of metallic nanoparticles on stem cell proliferation and differentiation. Nanomaterials (Basel) 2018;8(10):761. [PMID: 30261637 DOI: 10.3390/nano8100761]
- Zhang Y, Li K, Shen L, Yu L, Ding T, et al. Metal phenolic nanodressing of porous polymer scaffolds for enhanced bone regeneration via interfacial gating growth factor release and stem cell differentiation. ACS Appl Mater Interfaces 2022;14(1):268-77. [PMID: 34961319 DOI: 10.1021/acsami.1c19633]
- Cho W-S, Thielbeer F, Duffin R, Johansson EMV, Megson IL, et al. Surface functionalization affects the zeta potential, coronal stability and membranolytic activity of polymeric nanoparticles. Nanotoxicology 2014;8(2):202-11. [PMID: 23379633 DOI: 10.3109/17435390.2013.773465]
- Lim MPA, Lee WL, Widjaja E, Loo SCJ. One-step fabrication of core-shell structured alginate-PLGA/PLLA microparticles as a novel drug delivery system for water soluble drugs. Biomater Sci 2013;1(5):486-93. [PMID: 32482012 DOI: 10.1039/c3bm00175j]
- Quinlan E, López-Noriega A, Thompson E, Kelly HM, Cryan SA, et al. Development of collagen-hydroxyapatite scaffolds incorporating PLGA and alginate microparticles for the controlled delivery of rhBMP-2 for bone tissue engineering. J Control Release 2015;198:71-9. [PMID: 25481441 DOI: 10.1016/j.jconrel.2014.11.021]
- Abbah SA, Liu J, Goh JCH, Wong H-K. Enhanced control of in vivo bone formation with surface functionalized alginate microbeads incorporating heparin and human bone morphogenetic protein-2. Tissue Eng Part A 2013;19(3-4):350-9. [PMID: 22894570 DOI: 10.1089/ten.TEA.2012.0274]
- Lee CSD, Moyer HR, Gittens RAI, Williams JK, Boskey AL, et al. Regulating in vivo calcification of alginate microbeads. Biomaterials 2010;31(18):4926-34. [PMID: 20363022 DOI: 10.1016/j.biomaterials.2010.03.001]
- Choi DH, Park CH, Kim IH, Chun HJ, Park K, et al. Fabrication of core-shell microcapsules using PLGA and alginate for dual growth factor delivery system. J Control Release 2010;147(2):193-201. [PMID: 20647022 DOI: 10.1016/j.jconrel.2010.07.103]
- Park JS, Lim H-J, Yi SW, Park K-H. Stem cell differentiation-related protein-loaded PLGA microspheres as a novel platform micro-typed scaffold for chondrogenesis. Biomed Mater 2016;11(5):055003. [PMID: 27586647 DOI: 10.1088/1748-6041/11/5/055003]
- Jaklenec A, Hinckfuss A, Bilgen B, Ciombor DM, Aaron R, et al. Sequential release of bioactive IGF-I and TGF-beta 1 from PLGA microsphere-based scaffolds. Biomaterials 2008;29(10):1518-25. [PMID: 18166223 DOI: 10.1016/j.biomaterials.2007.12.004]
- Giavaresi G, Branda F, Causa F, Luciani G, Fini M, et al. Poly(2-hydroxyethyl methacrylate) biomimetic coating to improve osseointegration of a PMMA/HA/glass composite implant: in vivo mechanical and histomorphometric assessments. Int J Artif Organs 2004;27(8):674-80. [PMID: 15478538 DOI: 10.1177/039139880402700805]
- Poh CK, Ng S, Lim TY, Tan HC, Loo J, et al. In vitro characterizations of mesoporous hydroxyapatite as a controlled release delivery device for VEGF in orthopedic applications. J Biomed Mater Res A 2012;100(11):3143-50. [PMID: 22826183 DOI: 10.1002/jbm.a.34252]
- Acharya B, Chun S-Y, Kim S-Y, Moon C, Shin H-I, et al. Surface immobilization of MEPE peptide onto HA/β-TCP ceramic particles enhances bone regeneration and remodeling. J Biomed Mater Res B Appl Biomater 2012;100(3):841-9. [PMID: 22278974 DOI: 10.1002/jbm.b.32648]
- Zhao J, Shen G, Liu C, Wang S, Zhang W, et al. Enhanced healing of rat calvarial defects with sulfated chitosan-coated calcium-deficient hydroxyapatite/bone morphogenetic protein 2 scaffolds. Tissue Eng Part A 2012;18(1-2):185-97. [PMID: 21830854 DOI: 10.1089/ten.TEA.2011.0297]
- Ishack S, Mediero A, Wilder T, Ricci JL, Cronstein BN. Bone regeneration in critical bone defects using three-dimensionally printed β-tricalcium phosphate/hydroxyapatite scaffolds is enhanced by coating scaffolds with either dipyridamole or BMP-2. J Biomed Mater Res B Appl Biomater 2017;105(2):366-75. [PMID: 26513656 DOI: 10.1002/jbm.b.33561]
- Behnia H, Khojasteh A, Soleimani M, Tehranchi A, Atashi A. Repair of alveolar cleft defect with mesenchymal stem cells and platelet derived growth factors: a preliminary report. J Craniomaxillofac Surg 2012;40(1):2-7. [PMID: 21420310 DOI: 10.1016/j.jcms.2011.02.003]
- Wu C, Chang J. Mesoporous bioactive glasses: structure characteristics, drug/growth factor delivery and bone regeneration application. Interface Focus 2012;2(3):292-306. [PMID: 23741607 DOI: 10.1098/rsfs.2011.0121]
- Zhao YF, Loo SCJ, Chen YZ, Boey FYC, Ma J. In situ SAXRD study of sol-gel induced well-ordered mesoporous bioglasses for drug delivery. J Biomed Mater Res A 2008;85(4):1032-42. [PMID: 17937413 DOI: 10.1002/jbm.a.31545]
- Arcos D, Vallet-Regí M. Sol-gel silica-based biomaterials and bone tissue regeneration. Acta Biomater 2010;6(8):2874-88. [PMID: 20152946 DOI: 10.1016/j.actbio.2010.02.012]
- Wu C, Zhang Y, Ke X, Xie Y, Zhu H, et al. Bioactive mesopore-glass microspheres with controllable protein-delivery properties by biomimetic surface modification. J Biomed Mater Res A 2010;95(2):476-85. [PMID: 20648544 DOI: 10.1002/jbm.a.32873]
- Baino F, Fiume E. 3D printing of hierarchical scaffolds based on mesoporous bioactive glasses (MBGs)-fundamentals and applications. Materials (Basel) 2020;13(7):1688. [PMID: 32260374 DOI: 10.3390/ma13071688]
- Wu C, Zhang Y, Zhu Y, Friis T, Xiao Y. Structure-property relationships of silk-modified mesoporous bioglass scaffolds. Biomaterials 2010;31(13):3429-38. [PMID: 20122721 DOI: 10.1016/j.biomaterials.2010.01.061]
- Simmons CA, Alsberg E, Hsiong S, Kim WJ, Mooney DJ. Dual growth factor delivery and controlled scaffold degradation enhance in vivo bone formation by transplanted bone marrow stromal cells. Bone 2004;35(2):562-9. [PMID: 15268909 DOI: 10.1016/j.bone.2004.02.027]
- Patel ZS, Young S, Tabata Y, Jansen JA, Wong MEK, et al. Dual delivery of an angiogenic and an osteogenic growth factor for bone regeneration in a critical size defect model. Bone 2008;43(5):931-40. [PMID: 18675385 DOI: 10.1016/j.bone.2008.06.019]
- Young S, Patel ZS, Kretlow JD, Murphy MB, Mountziaris PM, et al. Dose effect of dual delivery of vascular endothelial growth factor and bone morphogenetic protein-2 on bone regeneration in a rat critical-size defect model. Tissue Eng Part A 2009;15(9):2347-62. [PMID: 19249918 DOI: 10.1089/ten.tea.2008.0510]
- Yilgor P, Sousa RA, Reis RL, Hasirci N, Hasirci V. Effect of scaffold architecture and BMP-2/BMP-7 delivery on in vitro bone regeneration. J Mater Sci Mater Med 2010;21(11):2999-3008. [PMID: 20740306 DOI: 10.1007/s10856-010-4150-1]
- Bonani W, Motta A, Migliaresi C, Tan W. Biomolecule gradient in micropatterned nanofibrous scaffold for spatiotemporal release. Langmuir 2012;28(38):13675-87. [PMID: 22950580 DOI: 10.1021/la302386u]
- Chen S, Shi Y, Zhang X, Ma J. Evaluation of BMP-2 and VEGF loaded 3D printed hydroxyapatite composite scaffolds with enhanced osteogenic capacity in vitro and in vivo. Mater Sci Eng C Mater Biol Appl 2020;112:110893. [PMID: 32409051 DOI: 10.1016/j.msec.2020.110893]
- Bai Y, Bai L, Zhou J, Chen H, Zhang L. Sequential delivery of VEGF, FGF-2 and PDGF from the polymeric system enhance HUVECs angiogenesis in vitro and CAM angiogenesis. Cell Immunol 2018;323:19-32. [PMID: 29111157 DOI: 10.1016/j.cellimm.2017.10.008]
- Kanczler JM, Barry J, Ginty P, Howdle SM, Shakesheff KM, et al. Supercritical carbon dioxide generated vascular endothelial growth factor encapsulated poly(DL-lactic acid) scaffolds induce angiogenesis in vitro. Biochem Biophys Res Commun 2007;352(1):135-41. [PMID: 17112464 DOI: 10.1016/j.bbrc.2006.10.187]
- Kempen DHR, Lu L, Heijink A, Hefferan TE, Creemers LB, et al. Effect of local sequential VEGF and BMP-2 delivery on ectopic and orthotopic bone regeneration. Biomaterials 2009;30(14):2816-25. [PMID: 19232714 DOI: 10.1016/j.biomaterials.2009.01.031]
- Jiang J, Tang A, Ateshian GA, Guo XE, Hung CT, et al. Bioactive stratified polymer ceramic-hydrogel scaffold for integrative osteochondral repair. Ann Biomed Eng 2010;38(6):2183-96. [PMID: 20411332 DOI: 10.1007/s10439-010-0038-y]
- Fang J, Liao J, Zhong C, Lu X, Ren F. High-strength, biomimetic functional chitosan-based hydrogels for full-thickness osteochondral defect repair. ACS Biomater Sci Eng 2022;8(10):4449-61. [PMID: 36070613 DOI: 10.1021/acsbiomaterials.2c00187]
- Zheng L, Li D, Wang W, Zhang Q, Zhou X, et al. Bilayered scaffold prepared from a kartogenin-loaded hydrogel and BMP-2-derived peptide-loaded porous nanofibrous scaffold for osteochondral defect repair. ACS Biomater Sci Eng 2019;5(9):4564-73. [PMID: 33448830 DOI: 10.1021/acsbiomaterials.9b00513]
- Wang W, Li H, Song P, Guo Y, Luo D, et al. Photo-crosslinked integrated triphasic scaffolds with gradient composition and strength for osteochondral regeneration. J Mater Chem B 2024;12(5):1271-84. [PMID: 38186375 DOI: 10.1039/d3tb02031b]
- Chen J, Chen H, Li P, Diao H, Zhu S, et al. Simultaneous regeneration of articular cartilage and subchondral bone in vivo using MSCs induced by a spatially controlled gene delivery system in bilayered integrated scaffolds. Biomaterials 2011;32(21):4793-805. [PMID: 21489619 DOI: 10.1016/j.biomaterials.2011.03.041]
- Kadri R, Bacharouch J, Elkhoury K, Ben Messaoud G, Kahn C, et al. Role of active nanoliposomes in the surface and bulk mechanical properties of hybrid hydrogels. Mater Today Bio 2020;6:100046. [PMID: 32259100 DOI: 10.1016/j.mtbio.2020.100046]
- Elkhoury K, Morsink M, Sanchez-Gonzalez L, Kahn C, Tamayol A, et al. Biofabrication of natural hydrogels for cardiac, neural, and bone tissue engineering applications. Bioact Mater 2021;6(11):3904-23. [PMID: 33997485 DOI: 10.1016/j.bioactmat.2021.03.040]
- Di Francesco M, Primavera R, Fiorito S, Cristiano MC, Taddeo VA, et al. Acronychiabaueri analogue derivative-loaded ultradeformable vesicles: physicochemical characterization and potential applications. Planta Med 2017;83(5):482-91. [PMID: 27542175 DOI: 10.1055/s-0042-112225]
- Sen CK, Ghatak S. miRNA control of tissue repair and regeneration. Am J Pathol 2015;185(10):2629-40. [PMID: 26056933 DOI: 10.1016/j.ajpath.2015.04.001]
- Li S, Wang X, Gu Y, Chen C, Wang Y, et al. Let-7 microRNAs regenerate peripheral nerve regeneration by targeting nerve growth factor. Mol Ther 2015;23(3):423-33. [PMID: 25394845 DOI: 10.1038/mt.2014.220]
- Roitbak T. MicroRNAs and regeneration in animal models of CNS disorders. Neurochem Res 2020;45(1):188-203. [PMID: 30877519 DOI: 10.1007/s11064-019-02777-6]
- Gao F, Kataoka M, Liu N, Liang T, Huang Z-P, et al. Therapeutic role of miR-19a/19b in cardiac regeneration and protection from myocardial infarction. Nat Commun 2019;10(1):1802. [PMID: 30996254 DOI: 10.1038/s41467-019-09530-1]
- Cheng N, Liu C, Li Y, Gao S, Han Y-C, et al. MicroRNA-223-3p promotes skeletal muscle regeneration by regulating inflammation in mice. J Biol Chem 2020;295(30):10212-23. [PMID: 32493731 DOI: 10.1074/jbc.RA119.012263]
- Hsueh M-F, Önnerfjord P, Bolognesi MP, Easley ME, Kraus VB. Analysis of “old” proteins unmasks dynamic gradient of cartilage turnover in human limbs. Sci Adv 2019;5(10):eaax3203. [PMID: 31633025 DOI: 10.1126/sciadv.aax3203]
- Duan L, Liang Y, Xu X, Xiao Y, Wang D. Recent progress on the role of miR-140 in cartilage matrix remodelling and its implications for osteoarthritis treatment. Arthritis Res Ther 2020;22(1):194. [PMID: 32811552 DOI: 10.1186/s13075-020-02290-0]
- Julier Z, Park AJ, Briquez PS, Martino MM. Promoting tissue regeneration by modulating the immune system. Acta Biomater 2017;53:13-28. [PMID: 28119112 DOI: 10.1016/j.actbio.2017.01.056]
- van der Kraan PM. The interaction between joint inflammation and cartilage repair. Tissue Eng Regen Med 2019;16(4):327-34. [PMID: 31413937 DOI: 10.1007/s13770-019-00204-z]
- Schett G. Effects of inflammatory and anti-inflammatory cytokines on the bone. Eur J Clin Invest 2011;41(12):1361-6. [PMID: 21615394 DOI: 10.1111/j.1365-2362.2011.02545.x]
- Gibon E, Lu LY, Nathan K, Goodman SB. Inflammation, ageing, and bone regeneration. J Orthop Translat 2017;10:28-35. [PMID: 29094003 DOI: 10.1016/j.jot.2017.04.002]
- Vishwakarma A, Bhise NS, Evangelista MB, Rouwkema J, Dokmeci MR, et al. Engineering immunomodulatory biomaterials to tune the inflammatory response. Trends Biotechnol 2016;34(6):470-82. [PMID: 27138899 DOI: 10.1016/j.tibtech.2016.03.009]
- Zhang B, Su Y, Zhou J, Zheng Y, Zhu D. Toward a better regeneration through implant-mediated immunomodulation: harnessing the immune responses. Adv Sci (Weinh) 2021;8(16):e2100446. [PMID: 34117732 DOI: 10.1002/advs.202100446]
- Sharafat-Vaziri A, Khorasani S, Darzi M, Saffarian Z, Alizadeh Z, et al. Safety and efficacy of engineered tissue composed of silk fibroin/collagen and autologous chondrocytes in two patients with cartilage defects: a pilot clinical trial study. Knee 2020;27(5):1300-9. [PMID: 33010742 DOI: 10.1016/j.knee.2020.06.015]
- Tamaddon M, Blunn G, Tan R, Yang P, Sun X, et al. In vivo evaluation of additively manufactured multi-layered scaffold for the repair of large osteochondral defects. Biodes Manuf 2022;5(3):481-96. [PMID: 35846348 DOI: 10.1007/s42242-021-00177-w]
- Lesage C, Lafont M, Guihard P, Weiss P, Guicheux J, et al. Material-assisted strategies for osteochondral defect repair. Adv Sci (Weinh) 2022;9(16):e2200050. [PMID: 35322596 DOI: 10.1002/advs.202200050]