Application of Music Therapy in Stroke Rehabilitation: A Research Review
1Kangwon National University, Gangwon-do, Korea
2Conservatory of Music, Shanghai, China
3Ningde Municipal Hospital of Ningde Normal University, Ningde, China
4Animal Medicine, College of Life Sciences, Longyan University, Longyan, China
5Department of Pediatrics, School of Pediatrics, Nanjing Medical University, Nanjing, China
6Fujian Zherong Vocational and Technical School, Ningde City, Fujian Province, China
7Department of Global Convergence, Kangwon National University, Gangwon-do, Republic of Korea
aThese authors contributed equally to this work.
*Correspondence to: Yanjin Wu, Fujian Zherong Vocational and Technical School, Ningde City, Fujian Province, China. E-mail: 651886525@qq.com; Maowei Chen, Department of Global Convergence, Kangwon National University, Republic of Korea. E-mail: muwi@kangwon.ac.kr
Received: April 23 2025; Revised: May 23 2025; Accepted: June 1 2025; Published Online: July 2 2025.
Cite this paper:
Wu K, Li C, Zhu S et al. Application of Music Therapy in Stroke Rehabilitation: A Research Review. BIO Integration 2025; 6: 1–20.
DOI: 10.15212/bioi-2025-0074. Available at: https://bio-integration.org/
Download citation
© 2025 The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/). See https://bio-integration.org/copyright-and-permissions/
Abstract
This article provides a systematic review of music therapy research progress and clinical applications in stroke rehabilitation. Music therapy, through techniques such as Melodic Intonation Therapy (MIT) and Rhythmic Auditory Stimulation (RAS), offers distinct advantages by activating alternative neural pathways and promoting neuroplasticity, which significantly improves emotional regulation, cognitive function, language expression, and motor function in stroke patients. According to clinical evidence, music therapy notably decreases depression and anxiety; promotes neuroplasticity; activates brain regions associated with language and motor function; and improves gait stability and limb coordination. However, current research faces challenges such as insufficient sample sizes, unclear long-term effects, and a lack of standardized protocols. Future studies should incorporate technologies such as artificial intelligence and virtual reality to explore personalized music therapy interventions and establish multi-center collaborative clinical research systems, thereby promoting standardized application of music therapy in stroke rehabilitation.
Keywords
Cognitive function, emotional improvement, language recovery, melodic intonation therapy, motor function, music therapy, neuroplasticity, rhythmic auditory stimulation, stroke rehabilitation.
Introduction
Stroke, the second leading cause of death and the primary cause of disability worldwide, has made rehabilitation an essential issue in the medical field [1]. Traditional rehabilitation methods, such as physical therapy, occupational therapy, and speech training, have been found to aid in motor function and language recovery, but have limitations in addressing emotional disorders and cognitive impairment, and restoring social function [2]. In recent years, music therapy, an emerging treatment integrating art and neuroscience, has become a research hotspot in the field of stroke rehabilitation, because of its non-invasive and multidimensional intervention characteristics [3].
Music therapy activates the limbic system, dopamine reward pathways, and motor cortex through specific musical elements (rhythm, melody, and harmony), thus constituting a distinct neuroregulatory mechanism due to its ability to target multiple neural pathways simultaneously and influence both emotional and motor responses [4]. Music stimulation synchronizes neural oscillations between the auditory and motor cortices, and consequently promotes neuroplasticity, which is crucial for the repair of damaged neural networks after stroke [5]. Techniques including Melodic Intonation Therapy (MIT) and Rhythmic Auditory Stimulation (RAS) have shown efficacy in language and motor recovery [6]. The high prevalence of post-stroke depression (PSD) further highlights the importance of music therapy in emotional regulation [7]. Five-Element Music Therapy has been shown to increase serum serotonin levels and alleviate depressive symptoms, in alignment with Traditional Chinese Medicine theories [8]. Group singing interventions have also been found to enhance social connection, decrease loneliness, and improve quality of life [9].
Music therapy enhances attention, memory, and executive functions through multisensory stimulation [10]. Personalized music listening programs improve Montreal Cognitive Assessment (MoCA) scores in post-stroke cognitive impairment (PSCI), especially in recall and orientation [11]. Combining music therapy with robot-assisted rehabilitation improves motor function and enhances rehabilitation adherence by inducing positive emotions [12].
Language rehabilitation is a core challenge in stroke treatment. MIT activates the right hemisphere language-motor area through interhemispheric mirror effects, and has greater efficacy than traditional speech therapy in treating non-fluent aphasia [13]. Neuroimaging studies have confirmed that MIT induces structural reorganization in the brain and enhances the language conduction efficiency of the right arcuate fasciculus [14]. However, the neural mechanisms of this therapy for East Asian languages require verification in large-scale studies, and the standardization of therapist qualifications must be addressed [15].
In terms of motor function recovery, RAS techniques have been found to improve gait symmetry and walking speed in patients with stroke, by regulating the basal ganglia-thalamus-cortex motor network [16]. When combined with multimodal balance training, RAS enhances dynamic balance in patients with Parkinson’s disease, particularly in the presence of mild cognitive impairment or Hoehn & Yahr stage 4 [6]. Notably, potential applications of music therapy in home rehabilitation are emerging, as its low cost and ease of implementation provide new insights for community-based rehabilitation [17].
Despite its potential, current research faces limitations such as small sample sizes and follow-up periods that are too brief, which weakens evidence for long-term effects [18]. There is also a lack of standardization in treatment protocols, with significant differences in music type, duration, and evaluation criteria, affecting result comparability [19]. Future studies should establish multicenter collaborative networks, conduct large-scale randomized controlled trials, and use neuroimaging techniques, including functional magnetic resonance imaging (fMRI) and EEG, to explore the neural mechanisms of music therapy in depth [20]. Personalized treatment systems based on artificial intelligence should also be developed.
The integration of virtual reality (VR) and wearable devices with music therapy offers an innovative platform [21]. Real-time motion-music mapping systems enable synchronized optimization of motor function training and emotional regulation in an immersive environment. Big data analytics can establish efficacy prediction models for stroke music therapy and consequently enable precise rehabilitation [22]. Combining music therapy with traditional and modern therapies including acupuncture and transcranial magnetic stimulation (TMS) is expected to synergistically enhance rehabilitation outcomes [23].
As global aging increases the demand for stroke rehabilitation, music therapy, because of its unique humanistic care and scientific intervention value, is becoming indispensable in comprehensive stroke rehabilitation systems [24]. Future research should focus on basic mechanisms, clinical practice, and technological innovation to provide safer and more effective humanized rehabilitation programs, to help achieve the “biological-psychological-social” comprehensive rehabilitation model [25].
Current applications of music therapy in stroke rehabilitation
WHO 2023 data indicate that approximately 17 million annual stroke cases occur worldwide, and 75% of survivors experience functional impairment [26]. Traditional rehabilitation methods, although effective in motor and language recovery, have limitations in addressing emotional, cognitive, and social impairment. Music therapy, combining art and neuroscience, has emerged as a promising non-invasive and multidimensional intervention [27].
Core challenges in stroke rehabilitation
Motor dysfunction is a prominent clinical feature following a stroke, with a significant proportion of patients experiencing hemiparesis or gait abnormalities [28]. Damage to the corticospinal tract following a stroke reduces the excitability of the motor cortex, resulting in patients exhibiting asymmetric gait, reduced walking speed, and impaired balance, as reflected in stride length differences, walking speed, and Berg Balance Scale scores [29]. Traditional Bobath therapy improves some aspects of motor function through neurofacilitation techniques; however, its long-term effects on motor pattern reorganization are limited [30]. For example, a study found that combining RAS with treadmill training resulted in a significant increase in walking speed and outperformed Bobath therapy alone in terms of effectiveness [31].
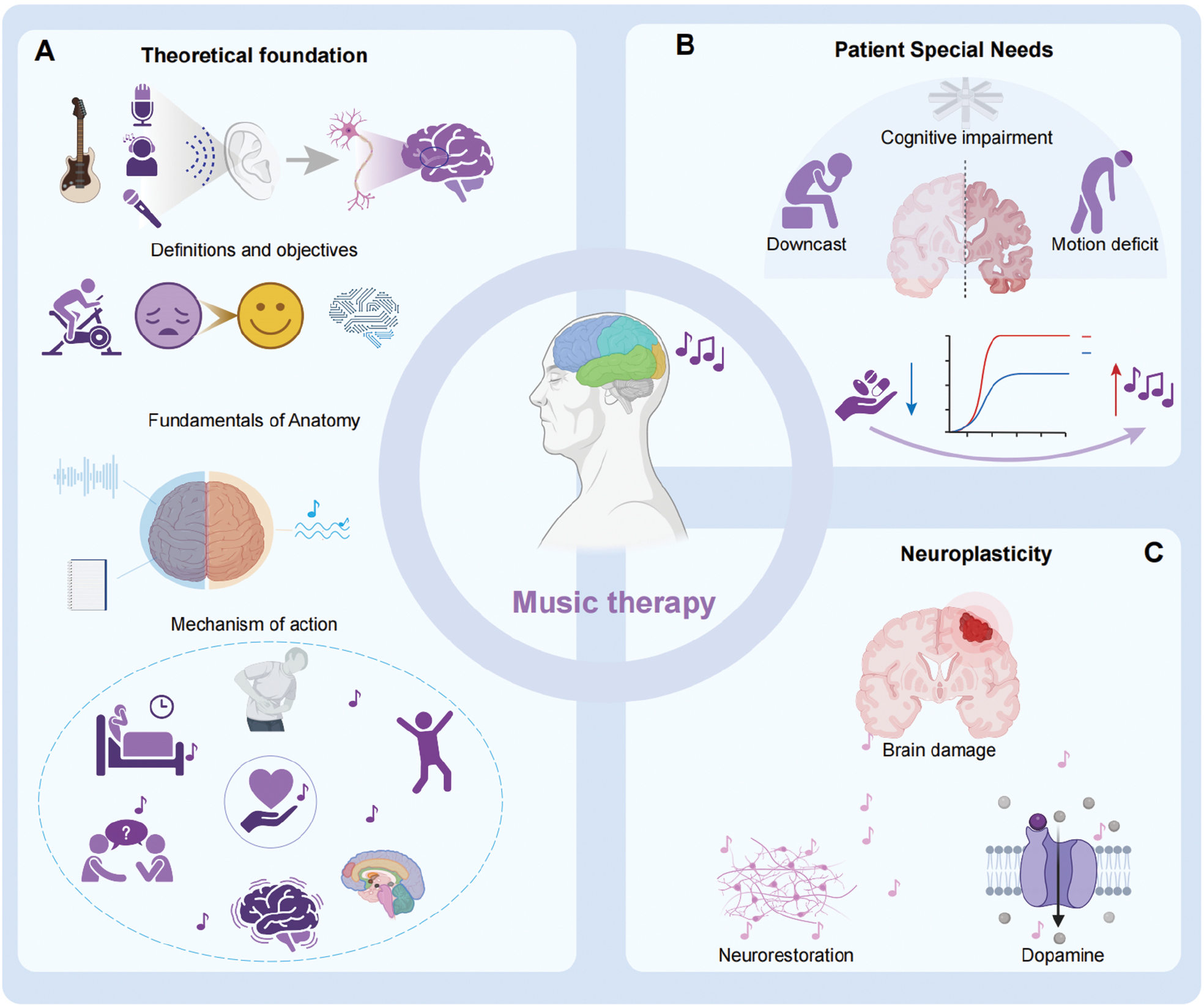
Cognitive impairment is common in stroke patients, with a significant proportion experiencing attention deficits, reduced working memory, and difficulties with executive function (Figure 1) [32]. Metabolic abnormalities in the prefrontal cortex and hippocampal region have been identified as the neurobiological basis underlying this impairment [33]. The average MoCA score of stroke patients is significantly lower compared to healthy controls, indicating impaired cognitive function [34]. Aphasia is a common post-stroke condition, with a substantial proportion of patients showing poor recovery during the early months of rehabilitation [35].
Figure 1 Overview of music therapy principles and applications. (A) Theoretical foundation: Music therapy uses various activities, such as auditory stimulation, playing instruments, and singing, to promote healing in physical, mental, and emotional aspects. The left and right hemispheres of the brain process music differently: the left hemisphere handles rhythm and lyrics, whereas the right hemisphere processes melody. The therapy leverages multi-sensory stimuli, including melody and rhythm, to regulate mood, enhance cognitive function, and improve behavior and overall quality of life. (B) Special patient needs: For patients with cognitive impairment and motion deficits, music therapy offers therapeutic benefits. It assists in cognitive rehabilitation by activating various brain areas and helps improve motor function, such as gait and spatio-temporal parameters, through rhythmic auditory strategies. (C) Neuroplasticity: Music therapy aids in neuroplasticity by promoting the reorganization and recovery of neural networks. This therapy has been shown to improve outcomes in patients with brain injury by altering the brain’s white matter structure and enhancing language processing. Additionally, music therapy stimulates the release of dopamine, thereby fostering positive emotional states and improving brain functions such as attention and motor control.
Language impairment, particularly aphasia caused by left-hemisphere damage, is another common post-stroke manifestation [35]. Non-fluent aphasia, resulting from damage to Broca’s area, often results in speech effort, grammatical deficiencies, and other symptoms [36]. The efficacy of traditional speech therapy is limited by active patient participation [37]. Aphasia is a common post-stroke condition, with many patients experiencing difficulty in regaining effective language function within the first months after the stroke [37]. More concerningly, the high incidence of PSD significantly decreases patient quality of life. In patients with PSD, infarct volume has been shown to correlate with increased serum cortisol levels, suggesting that elevated stress responses contribute to exacerbating neurological damage [38].
Mechanisms of action of music therapy
Music therapy can overcome traditional rehabilitation limitations through multidimensional neural modulation (Figure 1) [39]. The core of this therapy involves using musical elements (rhythm, melody, and harmony) to activate the brain’s limbic system, dopaminergic reward pathways, and motor cortex, thereby inducing distinct neural remodeling effects through the simultaneous modulation of emotional, reward, and motor regions [40]. Neuroimaging studies have established that musical stimuli foster neural plasticity by synchronizing β-oscillations (12–30 Hz) in the auditory and motor cortices [41]. For instance, MIT, which transforms language into musical melodies, activates compensatory right-hemisphere mechanisms and has been demonstrated to be more effective than traditional speech therapy for non-fluent aphasia [13]. According to fMRI studies have shown that MIT intervention increases activation in the right inferior frontal gyrus, and this enhancement is positively correlated with improved language expression abilities [42].
Dopamine system regulation is a key mechanism underlying the ability of music therapy to improve mood (Figure 1) [43]. Five Element Music Therapy has been shown to significantly increase serotonin levels in patients with PSD, and its liver-soothing and depression-relieving effects align closely with the principles of Traditional Chinese Medicine [44]. EEG studies have shown that listening to music increases alpha wave activity, suggesting that this enhances a relaxed brain state [45]. Moreover, group singing interventions have been found to improve social connection and activate dopamine release in the prefrontal cortex and striatum, enhancing patients’ sense of loneliness and quality of life [46].
In cognitive rehabilitation, multisensory stimulation through music therapy enhances attention, memory, and executive function (Figure 1) [47]. Personalized music listening programs have been found to improve delayed recall and orientation in patients with PSCI [48]. Studies examining event-related potential have shown that music interventions increase P300 wave amplitude by 18%—a finding reflecting increases in working memory [49]. Notably, combining music therapy with robot-assisted rehabilitation has been shown to significantly improve motor function and enhance rehabilitation adherence by promoting positive emotions, leading to a higher treatment completion rate and better overall outcomes for patients [12].
Clinical advances in music therapy
In motor rehabilitation, RAS technology increases gait symmetry and walking speed in patients with stroke by modulating the basal ganglia-thalamus-cortex motor network (Figure 1) [16]. Combining RAS with treadmill training has been demonstrated to increase walking speed by 13.2% and stride length by 10.7%, and to have particularly significant effects in patients during the subacute phase [50]. RAS, when combined with multimodal balance training, has been found to effectively increase dynamic balance in patients with Parkinson’s disease (3.2±1.8 Mini-BESTest score increase), through a mechanism involving enhanced α-wave synchronization in the frontal-temporal lobes [51]. Notably, RAS is expected to have increasing potential for home-based rehabilitation, as its low cost and ease of implementation provide new opportunities for community rehabilitation (Table 1) [52].
Table 1 Mechanisms and Clinical Functional Mapping of Music Therapy
| Functional Domain | Neurophysiological Mechanism | Key Intervention Elements | Clinical Impact | Rehabilitation Phase | |
|---|---|---|---|---|---|
| Rhythmic Modulation | Activation of basal ganglia-thalamocortical circuits, thus optimizing motor timing encoding |  |
Rhythmic synchronization training | Improved gait symmetry | Motor recovery (subacute phase) |
| Multimodal Integration | Co-activation of auditory-visual-motor association cortices, thus enhancing cross-modal integration |  |
Instrument playing with visual feedback | Enhanced language comprehension in aphasia | Chronic-phase reconstruction |
| Limbic Regulation | Strengthened amygdala-PFC connectivity, thus modulating HPA axis activity |  |
Personalized music listening | Decreased depression/anxiety scores | Acute-phase emotional intervention |
| Cognitive Remodeling | Functional reorganization of DMN and dorsal attention networks, thus enhancing working memory capacity |  |
Structured musical training | Improved executive function test performance | Cognitive rehabilitation (all phases) |
| Neuroplasticity | Increased interhemispheric compensation via the corpus callosum, leading to increased gray matter density |  |
Melodic intonation therapy | Enhanced verbal fluency scores | Chronic-phase neural remodeling |
| Autonomic Regulation | Enhanced vagal tone, which leads to improved heart rate variability (HRV) |  |
Music biofeedback | Decreased physiological stress markers (cortisol) | Acute-phase autonomic stabilization |
In speech rehabilitation, MIT activates the right hemisphere’s language motor areas through cross-hemispheric mirror effects, offering specific advantages in the treatment of non-fluent aphasia by enhancing neural efficiency and promoting structural brain remodeling (Table 1) [53]. Neuroimaging studies have confirmed that MIT induces structural brain remodeling and enhances the language conduction efficiency of the right arcuate fasciculus. A clinical study has shown improvements in phrase generation ability and naming accuracy after an 8-week MIT intervention [54]. However, the neurobiological mechanisms of MIT for East Asian languages require validation in large-scale studies, and the standardization of therapist qualifications must urgently be addressed [55]. The combination of low-frequency repetitive transcranial magnetic stimulation (rTMS) and MIT has been found to improve language fluency by 32% and to significantly outperform either therapy alone (p<0.01) [56].
Music therapy is also gaining attention for treating swallowing dysfunction. Music therapy has been shown to decrease fatigue visual analogue scale (VAS) scores, significantly outperforming other interventions [57]. This effect might be associated with vagus nerve activation induced by music, although further multi-center studies are needed for validation. Additionally, music therapy has shown positive effects in alleviating post-stroke fatigue: music interventions have been shown to decrease fatigue visual analogue scale (VAS) scores by 2.1±0.8, significantly outperforming the control group that received standard post-stroke care without music therapy intervention [58].
Specific applications of music therapy in stroke rehabilitation
Improvements in mood and psychological health
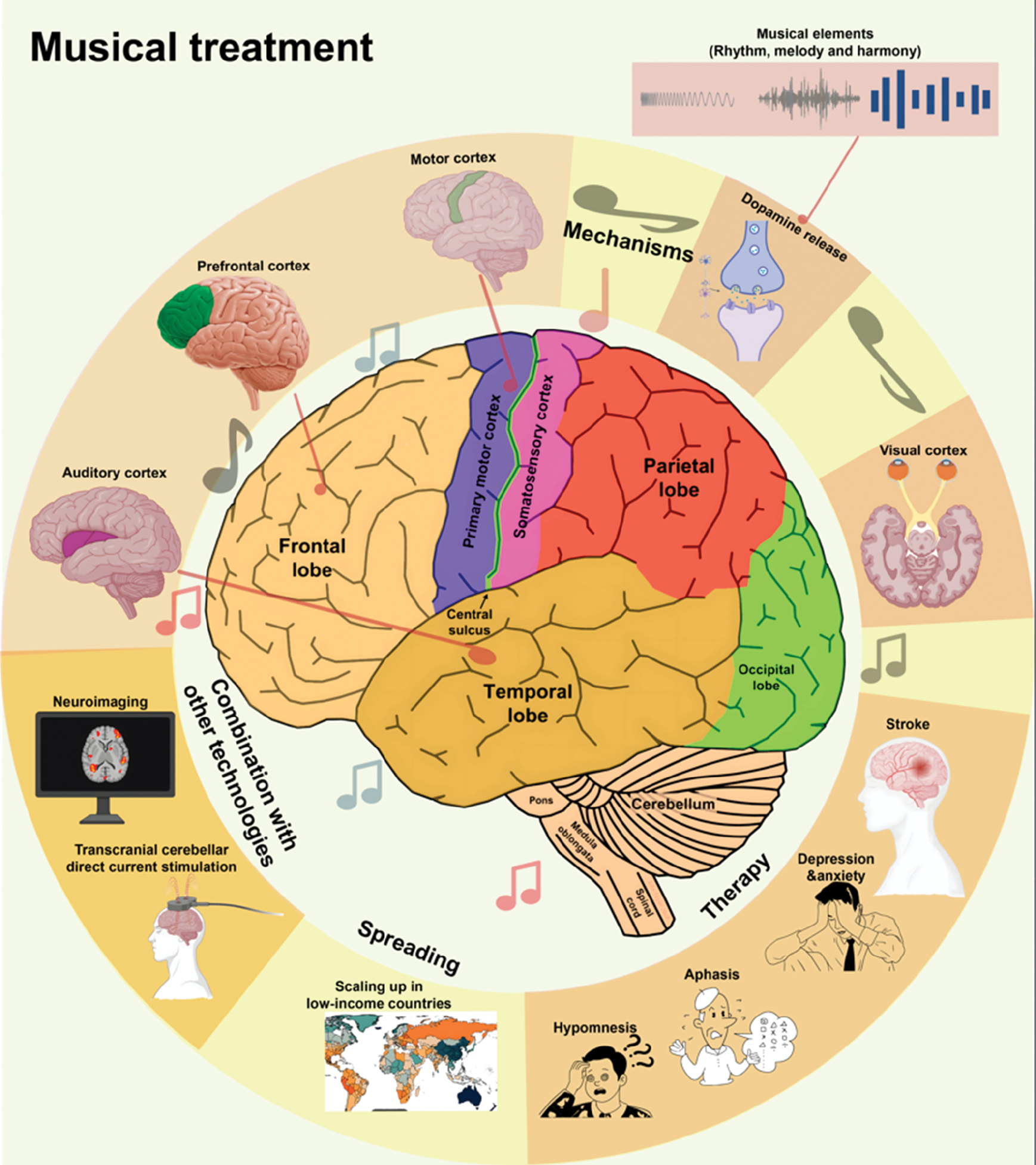
Because PSD is common and has a substantial impact on rehabilitation, emotional regulation plays a crucial role [59]. Music therapy has proven advantages in alleviating depression and anxiety symptoms by modulating neurotransmitter levels and facilitating the reconstruction of social function, particularly through its ability to engage the limbic system and enhance emotional regulation (Figure 2) [60]. Music therapy has been reported to decrease Hamilton Depression Rating Scale (HAMD-17) scores by 4.2±2.1 points and to increase serum serotonin levels by 28.7% in patients with PSD [7], by acting through the dopamine system and limbic system modulation.
Figure 2 Brain regions and mechanisms in musical treatment. This figure highlights the roles of music therapy in activating various brain regions, including the frontal, parietal, temporal, and occipital lobes, as well as the cerebellum and central sulcus. Music therapy influences areas such as the motor cortex for motor function recovery in patients with stroke, the prefrontal cortex for cognitive regulation, and the auditory cortex for processing of rhythm and melody. Additionally, the visual cortex may be involved in multisensory stimulation in some cases. The mechanisms of music therapy are also shown. Rhythm, melody, and harmony modulate brain activity, enhance motor coordination, and influence emotional regulation via dopamine release. Music therapy may be combined with techniques including neuroimaging and transcranial cerebellar direct current stimulation to improve outcomes. The figure also illustrates the global expansion of music therapy, particularly in low-income countries, and its therapeutic applications, including stroke rehabilitation, and treatment for depression, anxiety, sleep issues, and aphasia.
Clinical practice of five-element music therapy
Five-Element Music Therapy, based on the Five-Element Theory in Traditional Chinese Medicine, aligns the five musical tones (角, 徴, 宮, 商, and 羽) with the five internal organs (liver, heart, spleen, lung, and kidney). This modality ameliorates depressive symptoms by influencing cortical areas, the limbic system, and neurotransmitters including serotonin and dopamine, while enhancing neural plasticity and promoting post-stroke recovery [61].
Clinical studies have demonstrated that Five-Element Music Therapy is highly effective in patients with PSD [44]. In a randomized controlled trial involving 237 patients, a 12-week combination of this therapy and acupuncture, compared to CBT, notably decreased HAMD-17 scores and increased serotonin levels [62]. These findings might be explained by the music leading to HPA axis regulation and decreased cortisol secretion. The ability of Five-Element Music Therapy to improve Barthel Index scores further highlights its role in functional recovery [8, 63].
Collective intervention model for social function reconstruction
The collective intervention model for social function reconstruction improves social participation capabilities in patients with stroke through structured group activities [64]. This approach centers on using group interaction to promote coordinated recovery of cognitive, emotional, and motor function [65]. Collective interventions frequently involve choral singing, group discussions, and VR technologies, which enhance patients’ sense of belonging through social support and shared goals [66]. For instance, group singing interventions have been found to activate cortical and subcortical regions of the brain, thereby improving speech clarity and voice timing, whereas social interaction helps alleviate anxiety and loneliness (Table 2) [67]. Patients with Parkinson’s disease in choirs have demonstrated significant improvements in speech fluency and quality of life, along with marked increases in quality of life scores [68].
Table 2 Evidence-Based Application of Music Intervention Strategies in Neurorehabilitation
| Intervention Strategies | Targets and Mechanisms of Action | Applicable Stage | Key Clinical Advantages | Technology Integration Direction | |
|---|---|---|---|---|---|
| Rhythmic Auditory Stimulation (RAS) | Synchronizes motor cortex and basal ganglia activity and consequently optimizes gait cycles | Subacute phase | Improves gait parameters |  |
Wearable beat-synchronized devices |
| Melodic Intonation Therapy (MIT) | Activates language networks via right hemisphere compensation | Chronic phase | Restores speech fluency |  |
VR conversational scenarios |
| Music Biofeedback | Stabilizes autonomic function through vagal modulation | Acute phase | Decreases physiological stress |  |
AI-driven physiological mapping |
| Instrumental Training | Enhanced premotor-cerebellar connectivity for motor control | All phases | Improves upper limb function |  |
Robotic motion capture |
| Multisensory Integration | Strengthens cross-modal integration in the parietal cortex | Chronic cognitive phase | Enhances spatial attention |  |
AR environment embedding |
| Group Improvisation | Activates mirror neuron systems through social music interaction | Social recovery | Increases social cognition |  |
Cloud-based collaborative platforms |
VR and gamified training are key innovations in collective interventions [69]. By simulating social scenarios in immersive virtual environments, patients can practice communication skills in a safe space and gradually regain social function [70]. For example, VR-based role-playing games have been shown to help patients with aphasia activate language-related brain areas through dialogue tasks, thus achieving a 2.3-fold increase over traditional training [71]. Additionally, gamification designs incorporating point-based reward systems have been shown to enhance patient motivation, improve motor coordination, and foster social collaboration skills [72]. The effectiveness of this modality is associated with neural mechanisms: group music activities synchronize brain networks, and consequently enhance emotional resonance and memory consolidation [73]. According to fMRI studies, choir members show greater activation of the amygdala and hippocampus compared to solo singers; this synchronized activation has been suggested to enhance emotional resonance and memory consolidation. Furthermore, collective interventions have been shown to stimulate motor learning through the mirror neuron system [74]. For example, in dance therapy, the basal ganglia are activated as patients imitate others’ movements, and gait symmetry is improved [75].
Cognitive function recovery
PSCI severely affects the ability to perform daily activities (Table 2) [76]. Music therapy, by leveraging multisensory stimulation and activating neural plasticity, plays a pivotal role in the recovery of attention, memory, and executive function, particularly in patients with post-stroke cognitive impairment [77]. Personalized music listening has been shown to improve MoCA scores in patients with PSCI, with significant improvements observed in both delayed recall and orientation, suggesting its effectiveness in cognitive enhancement (Figure 2) [78].
Mechanisms of attention and memory enhancement
Music therapy, through activation of the default mode network and executive control network, enhances the brain’s ability to integrate information [77]. According to fMRI studies, music listening increases activation in the hippocampus and prefrontal cortex, thereby promoting episodic memory consolidation [79]. Notably, music interventions combined with VR technology have been shown to reduce reaction times and error rates in patients with attention deficits [80].
Neural basis of executive function promotion
RAS improves executive function by modulating the basal ganglia-thalamus-cortex loop [81]. RAS interventions have been shown to reduce Stroop test reaction times and enhance working memory capacity, contributing to improved cognitive performance. The mechanism underlying these effects is linked to enhanced β-wave synchronization, which increases functional connectivity between the motor cortex and prefrontal cortex. Notably, RAS interventions have proven particularly effective in patients with mild cognitive impairment, where they significantly slow disease progression [82].
Language function recovery
In patients with aphasia, a common complication following stroke, music therapy, particularly through methods including MIT, has shown distinct advantages in restoring both language expression and comprehension [83]. In patients with non-fluent aphasia, MIT has been shown to significantly improve phrase generation abilities and naming accuracy, surpassing traditional speech therapy in effectiveness (Table 2) [84]. The neural mechanisms underlying MIT involve compensatory activation of the right hemisphere through the mirror neuron system, thus simulating motor patterns for language production.
Interhemispheric mirror effects of MIT
MIT, by converting speech into musical melodies, activates the inferior frontal gyrus and insular cortex in the right hemisphere, and leads to formation of a language-music coupling network. According to fMRI studies, after MIT intervention, the integrity of the right arcuate fasciculus improves, and the speed of language conduction is enhanced [85]. Clinical data have indicated that MIT combined with low-frequency rTMS achieves dual physiological-psychological enhancement effects of enhancing language repetition ability and alleviating depressive symptoms [86].
Synergistic effects of multimodal intervention strategies
Song creation and narrative therapy activate the episodic memory network and facilitate language recovery [87]. Patients with aphasia participating in personalized song creation have shown significant improvements in spontaneous speech and in the accuracy of communicative intent [88]. The underlying mechanism involves coordinated activation of the hippocampus and temporal lobe cortex, thereby strengthening semantic network connectivity. Notably, combining VR with music interventions has been shown to enhance naming accuracy in patients within immersive environments.
Motor function rehabilitation
Motor dysfunction is a prominent clinical manifestation after stroke [89]. Music therapy techniques such as RAS and melodic support therapy have been found to have positive effects in improving gait, limb coordination, and swallowing function [90]. Combining RAS with treadmill training has been shown to improve walking speed, stride length, and balance, leading to better motor coordination and functional recovery (Figure 2) [50]. The underlying neural mechanism involves the synchronization enhancement of the cerebellum-thalamus-cortex loop, thereby facilitating motor pattern reorganization (Table 2) [91].
RAS techniques for gait and balance improvement
RAS synchronizes external rhythm in regulating basal ganglia motor programs. RAS synchronizes external rhythm in regulating basal ganglia motor programs. Consequently, RAS interventions have been shown to reduce gait freezing and improve dynamic balance in patients with Parkinson’s disease, contributing to better overall motor function (Table 2) [92]. Notably, RAS has significantly improved gait symmetry in patients with post-stroke unilateral spatial neglect, resulting in a reduction in step length asymmetry, thereby enhancing overall gait stability [16]. The underlying mechanism involves enhanced spatial attention allocation through excitability regulation in the parietal cortex (Table 3).
Table 3 Multidimensional Framework of Music Therapy in Neurological Rehabilitation
| Core Methods | Neural Intervention Mechanism | Clinical Impact | Target Conditions | ||
|---|---|---|---|---|---|
 |
Emotional Regulation | Personalized music listening/five-tone therapy | Modulates amygdala-PFC connectivity via dopaminergic release in the limbic system | Decreases post-stroke depression and enhances social interaction | Post-stroke mood disorders |
 |
Cognitive Remodeling | Structured rhythm training/melodic intonation therapy | Functional reorganization of DMN and dorsal attention networks, thus enhancing working memory capacity | Improves executive function and attention allocation | Post-stroke cognitive impairment/neurodegenerative disease |
 |
Motor Recovery | Rhythmic auditory stimulation (RAS)/instrumental music | Optimizes motor timing through basal ganglia-cerebellar loop synchronization | Enhances gait symmetry and upper limb coordination | Stroke/Parkinson’s disease movement disorders |
 |
Language Restoration | Melodic intonation therapy (MIT)/songwriting | Activates right Broca’s homolog through mirror neuron system compensation | Improves speech fluency and semantic comprehension | Non-fluent aphasia/primary progressive aphasia |
 |
Neuroplasticity | Multi-sensory integration training | Promotes white matter remodeling and increased gray matter density | Accelerates chronic-phase neural repair | Chronic stroke/brain injury repair |
 |
Social Function | Group improvisation/music biofeedback | Enhances empathy through mirror neuron system activation | Increases social participation and communication motivation | Traumatic brain injury/autism spectrum disorder |
Innovative models of limb coordination training
Music-assisted robotic rehabilitation systems, through real-time motion-music mapping, enhance fun and rehabilitation compliance among patients [93]. The combination of reminiscence music therapy with robotic training significantly increases patients’ sense of self-efficacy and accelerates motor function recovery [94]. Additionally, musical instrument interventions have been shown to improve fine motor skills in the hands, as demonstrated by increased finger dexterity and reduced tremor amplitude [95]. The underlying neural mechanism involves promotion of neuroplasticity through the coordinated activation of the motor cortex and cerebellum (Table 3) [96].
Music interventions for swallowing function recovery
Music-enhanced swallowing programs use rhythmic guidance to improve oral motor control [97]. In one study, after six sessions, patients showed significant improvements in oral motor control and laryngeal elevation. The underlying mechanism might be associated with vagus nerve activation induced by music, thereby enhancing pharyngeal muscle coordination and improving swallowing safety [98]. Notably, the combination of acupuncture with Five Elements Music Therapy has been shown to improve the Water Test grading for swallowing disorders and achieve superior efficacy compared to traditional rehabilitation training alone.
Interdisciplinary integrated treatment models
The integration of music therapy with other rehabilitation technologies achieves synergistic effects (Table 3). Combining music therapy with transcranial direct current stimulation accelerates motor function recovery in patients with stroke by 30% [99]. This effect is due to enhanced excitability modulation of the motor cortex by music stimulation. Additionally, music interventions combined with mindfulness-based stress reduction have been shown to reduce anxiety levels and improve cognitive function, offering dual physiological-psychological benefits [100].
Innovative applications of virtual reality technology
The fusion of VR and music therapy provides an immersive environment for rehabilitation [101]. VR-based music interventions have been shown to improve patients’ motor function more effectively than traditional training in simulation of real-life scenarios [102]. Furthermore, an AI-based personalized music recommendation system that dynamically adjusts music parameters based on physiological indicators, such as heart rate variability, and emotional states has been shown to significantly enhance therapeutic outcomes [103].
Value of community rehabilitation models
Music therapy, because of its low cost and easy implementation, is highly applicable to community-based rehabilitation. Community-based group singing programs have been shown to improve depressive symptoms and increase social participation, while being more cost-effective compared to hospital-based rehabilitation (Table 3) [104]. The success of such programs lies in establishing a “center-radiation” model, wherein a professional team provides technical support, and volunteers assist with daily activities, thus creating a sustainable rehabilitation network.
Clinical research and future directions in music therapy
Existing research findings
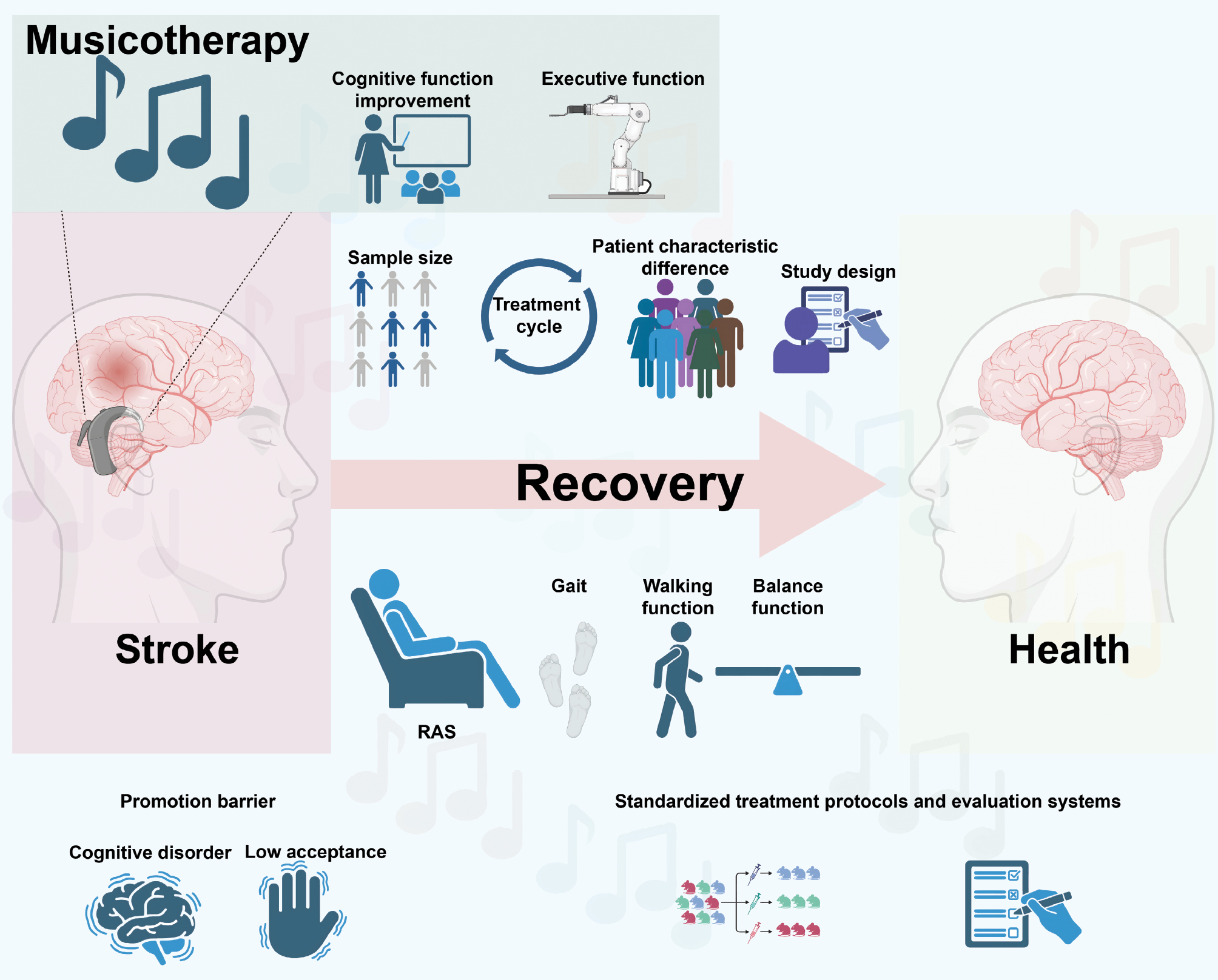
The clinical value of music therapy in stroke rehabilitation has been confirmed by numerous studies (Figure 3). A meta-analysis of 20 RCTs has indicated that Five-Element Music Therapy significantly ameliorates PSD, with substantial improvements in mood regulation [7]. The therapeutic effect is particularly significant for the combination of music therapy with acupuncture treatment, which has been shown to substantially reduce the HAMD-17 score. Serological studies have confirmed that this therapy regulates mood by increasing serotonin levels, aligning with Traditional Chinese Medicine theory regarding liver qi stagnation and emotional regulation [105].
Figure 3 Application of music therapy in stroke recovery. This figure outlines the use of music therapy for stroke rehabilitation, highlighting key components and factors influencing its effectiveness. On the left, the stroke section shows an anatomical profile of the brain with red areas indicating stroke damage, accompanied by an icon resembling a cochlear implant, thereby suggesting the role of music in brain stimulation. Below, two icons represent promotion barriers, including cognitive disorders (brain) and low patient acceptance (hand), which can hinder the widespread use of music therapy. In the recovery section, a pink arrow pointing from stroke to health symbolizes the healing process facilitated by music therapy. Rhythmic Auditory Stimulation (RAS) is depicted with icons of a person sitting, footprints, and a balance beam, signifying improvements in gait, walking function, and balance. Above, icons of sample size, treatment cycle, patient characteristic differences, and study design indicate factors potentially influencing the outcomes of music therapy. The health section on the right shows a healthy brain profile, indicating the recovery achieved through music therapy. Below, icons representing standardized treatment protocols and evaluation systems underscore the importance of structured and consistent approaches in implementing music therapy. Finally, the figure highlights the effects of music therapy on cognitive and executive function. The icon of a woman at a podium suggests improved cognitive function, such as attention and memory, whereas the robotic arm icon indicates enhanced executive function, which is crucial for planning, organization, and decision-making, thereby improving patients’ self-care and daily activities.
Robust evidence supports the use of MIT in language rehabilitation. fMRI studies have indicated activation of the right inferior frontal gyrus and insula, thereby forming a cross-hemispheric language compensation mechanism [13]. After 8 weeks of MIT, patients with non-fluent aphasia have shown significant improvements in phrase generation and naming accuracy [106]. RAS also has advantages in motor rehabilitation. The combination of RAS with treadmill training has been shown to significantly improve walking speed and stride length in patients with stroke, particularly in the subacute phase [107].
Multimodal interventions, such as personalized music listening combined with robotic-assisted rehabilitation, have been shown to improve MoCA scores and the Barthel Index in patients with PSE, demonstrating significant therapeutic benefits [108]. Group singing has been shown to significantly reduce loneliness and improve quality of life scores, providing valuable social and emotional benefits [109]. Together, these studies provide an evidence base for the clinical application of music therapy in stroke rehabilitation.
Challenges faced
Despite substantial progress, the clinical application of music therapy faces multiple challenges (Figure 3). First, research design limitations have limited the strength of the existing evidence (Table 4). Most clinical trials have included small sample sizes, and follow-up periods are often limited, thereby providing weak evidence of long-term efficacy [110]. Previous studies suggested a non-significant trend toward changes in depressive symptoms following music therapy. However, intervention protocols remain poorly standardized, with substantial variability in music characteristics, treatment duration, and outcome measures. In Five-Element Music Therapy, both intervention length and efficacy evaluation criteria vary across studies, and no unified assessment standard has been established [111].
Table 4 Challenges and Strategic Solutions in the Clinical Translation of Music Therapy
| Core Challenges | Current Strategies | Future Breakthroughs | |
|---|---|---|---|
 Standardization Deficits |
Heterogeneous intervention protocols lacking unified criteria | International consensus guidelines | Adaptive clinical trial platforms |
 Sample Representativeness |
Limited diversity in single-center studies with low subgroup power | Multinational research consortia | Phenotype-stratified enrollment |
 Long-term Evidence Gaps |
Dominance of short-term follow-up without stepped care tracking | Remote intelligent monitoring | Decade-long dynamic cohort studies |
 Functional Translation Barriers |
Failure of laboratory cognitive to translate to daily living capacity | VR-based ecological assessment | Community-engaged outcome networks |
 Home-based System Gaps |
Lack of safety/efficacy validation for remote interventions | Wearable-AI integrated monitoring | IoT-supported home rehabilitation |
 Special Population Gaps |
Absence of targeted protocols for patients with TBI and other specific groups | Delphi-based clinical pathways | Severity-stratified treatment tiers |
 Clinical Acceptance Barriers |
Poor adherence because of insufficient mechanistic understanding | Digital twin education systems | Neurologic MT certification programs |
 Technology Integration Gaps |
Disconnect between traditional and modern technological innovation | BCI-driven personalized algorithms | Multimodal biofeedback systems |
Delays in research on neurobiological mechanisms have affected clinical translation. Whereas fMRI studies in Western language speakers have shown that Melodic Intonation Therapy activates language-related areas in the right hemisphere, the tonal nature of East Asian languages such as Chinese may involve different patterns of brain activation, possibly leading to different therapeutic responses [112]. Moreover, the mechanisms through which music therapy affects swallowing function remain unclear. Prior studies have focused primarily on short-term behavioral gains and have lacked neuroimaging support [113]. Standardization of therapist qualifications is also essential, as a significant proportion of speech therapists have not received formal music training.
Structural barriers also hinder clinical promotion of music therapy (Table 4). For instance, in Hungary, only two rehabilitation centers employ music therapists. Insufficient investment and a shortage of professionals limit the widespread use of this modality. Additionally, a significant proportion of patients with stroke have cognitive biases against music therapy, believing that this treatment lacks scientific support. These challenges collectively impede the translation of music therapy from research to clinical practice [114] (Table 4).
Future research directions
Technological integration and innovation
The integration of VR and wearable devices provides an innovative platform for music therapy (Figure 3). A motion–music mapping system reported in prior work uses inertial sensors to translate hemiplegic limb movements into musical feedback, thereby supporting synchronized motor training and emotion-related regulation within an immersive rehabilitation setting [115]. This system’s clinical feasibility has been demonstrated in patients with subacute stroke, with minimal cycle delay and high computational efficiency (quad-core processor). Future efforts should focus on further developing interactive content and evaluating its effects on motor learning, performance retention, and psychological factors [116].
AI-driven personalized treatment plans are an important emerging trend. Deep-learning-based music recommendation systems can analyze patients’ physiological data (EEG and HRV) and emotional states, and use this information to dynamically adjust music parameters, such as tempo and melody complexity [117]. AI-assisted programs have been shown to improve treatment efficacy and enhance patient compliance, providing better overall outcomes in rehabilitation [118]. Integrating multi-omics technologies (e.g., genomics and metabolomics) can also aid in the creation of predictive models for stroke-related music therapy efficacy and enable precise rehabilitation [119].
Mechanistic research advancements
The application of multimodal neuroimaging techniques is expected to drive breakthroughs in mechanistic research [120]. Simultaneous EEG-fMRI studies have shown that RAS intervention enhances α-wave synchronization in the frontal-temporal lobes; however, its effects on the cerebellum-thalamus-cortex network require further exploration [5]. Research on MIT for East Asian languages should incorporate diffusion tensor imaging technology to clarify the role of the right arcuate fasciculus in tonal language rehabilitation. Additionally, investigating the effects of music therapy on the gut microbiota-gut-brain axis might reveal new mechanisms for improving mood.
Exploration of the neural mechanisms of cross-cultural language therapy is a critical future research direction. As a tonal language, Chinese differs fundamentally in prosodic structure from Western languages [121]. Future large-sample studies should compare MIT’s efficacy between Chinese- and English-speaking patients, to develop Chinese-tailored treatment plans. Moreover, exploration of music therapy’s potential in multilingual aphasia, such as post-stroke bilingual aphasia, also holds great promise [18].
Clinical translation pathways
Strategies for promoting community rehabilitation models must be systematically developed. According to the “center-periphery” model, integrating community volunteer-led music activities with remote guidance from professional therapists can significantly enhance participation in home-based rehabilitation. Future efforts should focus on creating standardized training systems and developing affordable, portable devices, such as smart music gloves, to reduce barriers to community rehabilitation [122].
An integrated multidisciplinary collaborative treatment system is a key direction for future development [123]. The combined application of music therapy with acupuncture and TMS has shown synergistic effects [124]. For example, low-frequency rTMS combined with MIT has been shown to improve language repetition abilities and decrease depressive symptoms [125]. Future work should focus on establishing interdisciplinary treatment guidelines to define the optimal combinations and sequencing of therapies [126].
Conclusion and outlook
Music therapy, an innovative intervention in stroke rehabilitation, provides treatment benefits that cannot be achieved through traditional rehabilitation methods [127]. This modality has been shown to improve emotional, cognitive, language, and motor function through neural modulation and humanistic care [48]. For instance, Five-Element Music Therapy can effectively treat post-stroke depression by modulating serotonin levels, whereas MIT enhances language abilities in patients with non-fluent aphasia through right hemisphere compensation [14, 44]. These findings offer new perspectives for stroke rehabilitation.
The main advantage of music therapy lies in its “biopsychosocial” integrative effects [3]. RAS improves gait parameters by modulating the basal ganglia-thalamic-cortical motor network [128]. Music therapy decreases isolation through group interactions. However, clinical evidence has shown significant heterogeneity: meta-analyses have shown a significant effect of music therapy on post-stroke depression, although with high heterogeneity among studies [129]. Standardized treatment protocols must be developed. Moreover, most clinical trials have had small sample sizes and short follow-up periods, thus limiting the evidence of long-term efficacy [130].
Significant heterogeneity exists in the available clinical evidence. Meta-analyses have shown that music therapy has a meaningful effect on PSD, though the high heterogeneity across studies highlights the importance of developing standardized treatment protocols [7]. For example, the neurobiological mechanisms of MIT in the Chinese-speaking context remain unclear, and the standardization of therapist qualifications must urgently be addressed [131]. Additionally, most clinical trials have included small sample sizes (<50 participants) and insufficient follow-up periods (<6 months), thus leading to a lack of evidence of long-term efficacy.
Technological innovation will be crucial to overcoming these limitations (Table 5). Integrating VR and wearable devices offers an immersive rehabilitation environment. AI-based systems can dynamically adjust music parameters in real time, thereby enhancing training effects [132, 133]. Big data analytics can be used to develop predictive models for music therapy efficacy and to enable precise rehabilitation [134]. Multi-omics techniques and neuroimaging analyses should be used to explore music therapy’s molecular mechanisms in synaptic plasticity, and its effects on brain-derived neurotrophic factor and related pathways [135, 136]. Cross-cultural studies will be essential to understand differences in right hemisphere activation during MIT for East Asian languages [137].
Table 5 Music Therapy Innovation Model and Transformation Challenges
| Core Technology Carrier | Clinical Transformation Scenarios | Mechanism Breakthrough | Key Challenges | |
|---|---|---|---|---|
| Digital Therapeutics Innovation | Virtual reality piano simulation system | Remote sports rehabilitation | Multimodal perception-motor circuit remodeling mechanism | Lack of standardization of motion tracking accuracy |
| Reconstruction of Community Medicine | Multidisciplinary collaboration cloud platform | Chronic aphasia management | Social prescription drives neuroplasticity | Complexity of community resource integration |
| Precision Combined Therapy | Drug-music co- regulation protocol | Post-stroke neuropsychiatric symptoms | Serotonergic-limbic system interaction mechanism | Difficulty in defining dose-response curves |
| Intelligent Control System | Emotional computing dynamic music generation engine | Long-term COVID-19 cognitive rehabilitation | Bidirectional regulatory pathway of the autonomic nervous system- immune axis | Real-time biosignal decoding threshold |
| Humanistic Integration | Life review music narrative intervention | Psychological reconstruction in older patients with stroke | Default mode network-autobiographical memory coupling mechanism | Insufficient validation of cultural fit |
| Inclusive Medical Care Expansion | Wearable beat-synchronized biofeedback device | Parkinson’s disease freezing of gait intervention | Phase resetting mechanism of basal ganglia-thalamus oscillations | Accessibility-quality balance dilemma |
Expanding clinical translation pathways is key to making music therapy widely accessible. The promotion of community-based rehabilitation models must address the shortage of therapists. One possibility for overcoming this challenge is implementing remote rehabilitation via telemedicine platforms to offer expert-guided home rehabilitation (Table 5) [138]. Multidisciplinary collaborative treatment systems, such as combined application of music therapy and acupuncture, may jointly regulate serotonin and dopamine systems, thereby enhancing PSD treatment efficacy (Table 5) [139].
Furthermore, a standardized evaluation system for music therapy must be established, and biomarker-based efficacy assessment tools must be developed. Specific examples include the development of intervention manuals, clinical guidelines, standardized outcome measures, and a professional certification system for music therapists. An intervention manual that specifies the goals of each intervention technique (such as improving language expression in patients with aphasia and enhancing gait symmetry in patients with motor dysfunction) must be developed, and standardized procedures including music selection criteria, treatment activity, and progression criteria must be established. The standardized evaluation of treatment outcomes with standardized outcome indicators will be crucial for assessing the effectiveness of music therapy interventions. Fully validated assessments should be used for target function, such as the MoCA for cognitive function, the HAMD-17 for emotional health, the Boston Aphasia Test for language function, or the Berg Balance Scale for motor function. In addition, a professional certification system for music therapists would ensure consistent quality of care.
As global aging accelerates, stroke incidence has been projected to reach 62 million cases by the year 2050, as projected by the World Health Organization (WHO) in 2020 [140]. The low cost and high accessibility of music therapy should make this strategy key to addressing this challenge [141]. In low-income countries, remote intervention music therapy can be delivered via mobile applications [142]. In high-income countries, integrating music therapy with smart home devices may advance proactive health management models. Additionally, music therapy has potential in rehabilitation for long COVID-19: preliminary research has suggested that singing interventions might mitigate “brain fog” and fatigue symptoms [143, 144]. New applications for music therapy are expected to increase the necessity of understanding its mechanisms.
In conclusion, music therapy has value in stroke rehabilitation, but faces technological, mechanistic, and translational challenges. Future research should focus on basic mechanisms, technological innovations, and clinical practices, to develop safer, more effective, and patient-centered rehabilitation programs. Through interdisciplinary integration and global collaborative networks, music therapy is poised to become a core component of comprehensive stroke rehabilitation systems and to benefit patients worldwide.
Data availability statement
This review article is based on previously published studies and does not include new data generated or analyzed by the authors. All data supporting the findings of this study are available within the cited literature.
Author contributions
Ke Wu, Chenxi Li, and Sike Zhu contributed equally to the conceptualization, literature review, and drafting of the manuscript. Jiajia Zhuang and Ruogu Chen were responsible for methodology guidance and critical revision of the manuscript. Xiuhui Ji contributed to the clinical relevance and interpretation of findings. Yanjin Wu and Maowei Chen supervised the study, provided overall direction, and finalized the manuscript. All authors read and approved the final manuscript.
Funding or acknowledgment
No funding or sponsorship was received for this study. The authors would like to thank all the researchers whose work has contributed to this review.
Conflict of interest
The authors declare that there are no conflicts of interest.
Graphical abstract

Highlights
Music therapy enhances recovery after stroke by simultaneously improving emotional well-being, cognitive processing, speech production, and motor coordination. Techniques such as Melodic Intonation Therapy (MIT) and Rhythmic Auditory Stimulation (RAS) activate specific brain networks and promote neuroplasticity. This personalized, non-invasive, and cost-effective approach holds promise as a complementary rehabilitation strategy. Looking ahead, integration with artificial intelligence, virtual reality, and other multimodal technologies may further expand its clinical applications.
In brief
Music therapy promotes stroke recovery by improving emotional, cognitive, language, and motor functions. Techniques such as MIT and RAS stimulate brain plasticity and support rehabilitation. Future integration with AI and VR may further enhance outcomes.
References
- Syafni AN. Post stroke patient medical rehabilitation. J Ilm Kesehat. Sandi Husada 2020;12:873-877. [DOI: 10.35816/jiskh.v12i2.428]
- Stockbridge MD, Bunker LD, Hillis AE. Reversing the ruin: rehabilitation, recovery, and restoration after stroke. Curr Neurol Neurosci Rep 2022;22:745-755. [PMID: 36181577 DOI: 10.1007/s11910-022-01231-5]
- Strzemecka J. Music therapy in stroke rehabilitation. J Pre Clin Clin Res 2013;7:23-26. [DOI: 10.26444/jpccr/71429]
- Stegemöller EL. Exploring a neuroplasticity model of music therapy. J Music Ther 2014;51:211-227. [PMID: 25316915 DOI: 10.1093/jmt/thu023]
- Thaut MH, Abiru M. Rhythmic auditory stimulation in rehabilitation of movement disorders: a review of current research. Music Percept 2010;27:263-269. [DOI: 10.1525/mp.2010.27.4.263]
- Kadivar Z, Corcos DM, Foto J, Hondzinski JM. Effect of step training and rhythmic auditory stimulation on functional performance in Parkinson patients. Neurorehabil Neural Repair 2011;25:626-635. [PMID: 21436393 DOI: 10.1177/1545968311401627]
- Dayuan Z, Lan L, Hui C, Huanjie L, Deliang L, et al. The effect of music as an intervention for post-stroke depression: a systematic review and meta-analysis. Complement Ther Med 2022;71:102901. [PMID: 36399968 DOI: 10.1016/j.ctim.2022.102901]
- Zhong K, An X, Kong Y. The effectiveness of five-element music therapy for post-stroke depression: a systematic review and meta-analysis. Heliyon 2024;10:e26603. [PMID: 38444465 DOI: 10.1016/j.heliyon.2024.e26603]
- Hendry N, Lynam DS, Lafarge C. Singing for wellbeing: formulating a model for community group singing interventions. Qual Health Res 2022;32:1399-1414. [PMID: 35622710 DOI: 10.1177/10497323221104718]
- Thaut MH. Neurologic music therapy in cognitive rehabilitation. Music Percept 2010;27:281-285. [DOI: 10.1525/mp.2010.27.4.281]
- Fan LP, Quijano-Ruiz A, Wang C, Zhao HW, Wang DN, et al. Effects of personalized music listening on post-stroke cognitive impairment: a randomized controlled trial. Complement Ther Clin Pract 2024;57:101885. [PMID: 39098085 DOI: 10.1016/j.ctcp.2024.101885]
- Liu Q, Liu L, Liu Z, Xu Y, Wang F, et al. Reminiscent music therapy combined with robot-assisted rehabilitation for elderly stroke patients: a pilot study. J Neuroeng Rehabil 2024;21:16. [PMID: 38291426 DOI: 10.1186/s12984-024-01315-y]
- Schlaug G, Norton A, Marchina S, Zipse L, Wan CY. From singing to speaking: facilitating recovery from nonfluent aphasia. Future Neurol 2010;5:657-665. [PMID: 21088709 DOI: 10.2217/fnl.10.44]
- García-Casares N, Barros-Cano A, García-Arnés JA. Melodic intonation therapy in post-stroke non-fluent aphasia and its effects on brain plasticity. J Clin Med 2022;11:3503. [PMID: 35743571 DOI: 10.3390/jcm11123503]
- Hou P-W, Hsu H-C, Lin Y-W, Tang N-Y, Cheng C-Y, et al. The history, mechanism, and clinical application of auricular therapy in traditional Chinese medicine. Evid Based Complement Alternat Med 2015;2015:495684. [PMID: 26823672 DOI: 10.1155/2015/495684]
- Lee SH, Lee KJ, Song CH. Effects of rhythmic auditory stimulation (RAS) on gait ability and symmetry after stroke. J Phys Ther Sci 2012;24:311-314. [DOI: 10.1589/jpts.24.311]
- Du B, Sun T. The application and development of music therapy in rehabilitation medicine. J Contemp Educ Res 2024;8:283-289. [DOI: 10.26689/jcer.v8i7.7812]
- Xu C, He Z, Shen Z, Huang F. Potential benefits of music therapy on stroke rehabilitation. Oxid Med Cell Longev 2022;2022:9386095. [PMID: 35757506 DOI: 10.1155/2022/9386095]
- Koger SM, Chapin K, Brotons M. Is music therapy an effective intervention for dementia? A meta-analytic review of literature. J Music Therapy 1999;36:2-15. [PMID: 10519841 DOI: 10.1093/jmt/36.1.2]
- Lin S-T, Yang P, Lai C-Y, Su Y-Y, Yeh Y-C, et al. Mental health implications of music: insight from neuroscientific and clinical studies. Har Rev Psychiatry 2011;19:34-46. [PMID: 21250895 DOI: 10.3109/10673229.2011.549769]
- Brungardt A, Wibben A, Tompkins AF, Shanbhag P, Coats H, et al. Virtual reality-based music therapy in palliative care: a pilot implementation trial. J Palliat Med 2021;24:736-742. [PMID: 33227225 DOI: 10.1089/jpm.2020.0403]
- Xu W, Liu L, Zhang J. Application analysis based on big data technology in stroke rehabilitation nursing. J Healthc Eng 2021;2021:3081549. [PMID: 34900181 DOI: 10.1155/2021/3081549]
- Xiang C, Huo W. Research progress on the use of music therapy combined with transcranial magnetic stimulation to treat cognitive impairment after stroke. Clin Neurosci Res 2024;2:49-53. [DOI: 10.26689/cnr.v2i1.6280]
- Ard J, Wheeler BL. Music therapy and stroke: an integrative review. Music Medicine 2016;8:146. [DOI: 10.47513/mmd.v8i4.496]
- Micera S, Caleo M, Chisari C, Hummel FC, Pedrocchi A. Advanced neurotechnologies for the restoration of motor function. Neuron 2020;105:604-620. [PMID: 32078796 DOI: 10.1016/j.neuron.2020.01.039]
- Katan M, Luft A. Global burden of stroke. Semin Neurol 2018;38:208-211. [PMID: 29791947 DOI: 10.1055/s-0038-1649503]
- Purdie H. Music therapy with adults who have traumatic brain injury and stroke. Br J Music Ther 1997;11:45-50. [DOI: 10.1177/135945759701100203]
- Dimyan MA, Cohen LG. Neuroplasticity in the context of motor rehabilitation after stroke. Nat Rev Neurol 2011;7:76-85. [DOI: 10.1038/nrneurol.2010.200]
- Jayaram G, Stagg CJ, Esser P, Kischka U, Stinear J, et al. Relationships between functional and structural corticospinal tract integrity and walking post stroke. Clin Neurophysiol 2012;123:2422-2428. [PMID: 22717679 DOI: 10.1016/j.clinph.2012.04.026]
- Levin MF, Panturin E. Sensorimotor integration for functional recovery and the Bobath approach. Motor Control 2011;15:285-301. [PMID: 21628730 DOI: 10.1123/mcj.15.2.285]
- Thaut MH, Leins AK, Rice RR, Argstatter H, Kenyon GP, et al. Rhythmic auditory stimulation improves gait more than NDT/Bobath training in near-ambulatory patients early poststroke: a single-blind, randomized trial. Neurorehabil Neural Repair 2007;21:455-459. [PMID: 17426347 DOI: 10.1177/1545968307300523]
- Nys GMS, Van Zandvoort MJE, De Kort PLM, Jansen BPW, De Haan EHF, et al. Cognitive disorders in acute stroke: prevalence and clinical determinants. Cerebrovasc Dis 2007;23:408-416. [PMID: 17406110 DOI: 10.1159/000101464]
- Browne SE, Lin L, Mattsson A, Georgievska B, Isacson O. Selective antibody-induced cholinergic cell and synapse loss produce sustained hippocampal and cortical hypometabolism with correlated cognitive deficits. Exp Neurol 2001;170:36-47. [PMID: 11421582 DOI: 10.1006/exnr.2001.7700]
- Cumming TB, Bernhardt J, Linden T. The montreal cognitive assessment: short cognitive evaluation in a large stroke trial. Stroke 2011;42:2642-2644. [PMID: 21757673 DOI: 10.1161/STROKEAHA.111.619486]
- Armour M, Cherney LR, Del Toro CM, Maher LM, Raymer AM. Aphasia FAQs for the rehabilitation professional. Arch Phys Med Rehabil 2021;102:1243-1245. [PMID: 33775389 DOI: 10.1016/j.apmr.2021.01.068]
- Ogar JM, Dronkers NF, Brambati SM, Miller BL, Gorno-Tempini ML. Progressive nonfluent aphasia and its characteristic motor speech deficits. Alzheimer Dis Assoc Disord 2007;21:S23-S30. [PMID: 18090419 DOI: 10.1097/WAD.0b013e31815d19fe]
- Barletta V, Calvano M, Curci A, Piccinno A. A new interactive paradigm for speech therapy. In: Abdelnour Nocera J, Kristín Lárusdóttir M, Petrie H, Piccinno A, Winckler M, editors. Human-computer interaction – INTERACT 2023. Lecture notes in computer science. Cham: Springer Nature Switzerland; 2023. pp. 380-385. [DOI: 10.1007/978-3-031-42293-5_39]
- Agarwal A, Iqbaal H. Serum-cortisol levels in severity of stroke. Int J Med Biomed Stud 2020;4:970. [DOI: 10.32553/ijmbs.v4i2.970]
- Liang R, Qian L. The application and advantages of music therapy in the rehabilitation of the elderly. MedSci 2024;1. [DOI: 10.61173/vq9ymv67]
- Galińska E. Music therapy in neurological rehabilitation settings. Psychiatr Pol 2015;49:835-846. [PMID: 26488358 DOI: 10.12740/PP/25557]
- Fujioka T, Ross B, Trainor LJ. Beta-band oscillations represent auditory beat and its metrical hierarchy in perception and imagery. J Neurosci 2015;35:15187-15198. [PMID: 26558788 DOI: 10.1523/JNEUROSCI.2397-15.2015]
- Rota G, Sitaram R, Veit R, Erb M, Weiskopf N, et al. Self-regulation of regional cortical activity using real-time fMRI: the right inferior frontal gyrus and linguistic processing. Hum Brain Mapp 2009;30:1605-1614. [PMID: 18661503 DOI: 10.1002/hbm.20621]
- Kawahata I, Kawahata I, Hasegawa K, Kase R. Music and dopamine – potential in movement disorders. J Brain Nerves 2020:1-4. [DOI: 10.31487/j.JBN.2020.01.02]
- Lin F-C, Huang D-H, He N-N, Qin Y-H, Li S-D, et al. Influence of traditional Chinese medicine five-element musical therapy on depression severity and neurological functional deficit scale in patients with post-stroke depression. 2016 8th International Conference on Information Technology in Medicine and Education (ITME); Fuzhou: IEEE; 2016;199-208. [DOI: 10.1109/ITME.2016.0054]
- Vijayalakshmi K, Sridhar S, Khanwani P. Estimation of effects of alpha music on EEG components by time and frequency domain analysis. International Conference on Computer and Communication Engineering (ICCCE’10); Kuala Lumpur, Malaysia: IEEE; 2010:1-5. [DOI: 10.1109/ICCCE.2010.5556761]
- Williams E, Dingle GA, Clift S. A systematic review of mental health and wellbeing outcomes of group singing for adults with a mental health condition. Eur J Public Health 2018;28:1035-1042. [PMID: 29982515 DOI: 10.1093/eurpub/cky115]
- Mangiacotti A, Hsu MH, Barone C, Di Liberto G, Van Puyvelde M, et al. P3-465: Effects of music therapy in elderly care: cognition, biomarkers, mood and social behaviour. Alzheimer’s & Dementia 2019;15:P1144. [DOI: 10.1016/j.jalz.2019.06.3500]
- Särkämö T, Soto D. Music listening after stroke: beneficial effects and potential neural mechanisms. Ann N Y Acad Sci 2012;1252:266-281. [PMID: 22524369 DOI: 10.1111/j.1749-6632.2011.06405.x]
- George EM, Coch D. Music training and working memory: an ERP study. Neuropsychologia 2011;49:1083-1094. [PMID: 21315092 DOI: 10.1016/j.neuropsychologia.2011.02.001]
- Mainka S, Wissel J, Völler H, Evers S. The use of rhythmic auditory stimulation to optimize treadmill training for stroke patients: a randomized controlled trial. Front Neurol 2018;9:755. [PMID: 30271375 DOI: 10.3389/fneur.2018.00755]
- Capato TTC, De Vries NM, IntHout J, Ramjith J, Barbosa ER, et al. Multimodal balance training supported by rhythmic auditory stimuli in parkinson disease: effects in freezers and nonfreezers. Phys Ther 2020;100:2023-2034. [PMID: 32737973 DOI: 10.1093/ptj/pzaa146]
- Chen Y, Baran M, Sundaram H, Rikakis T. A low cost, adaptive mixed reality system for home-based stroke rehabilitation. Annu Int Conf IEEE Eng Med Biol Soc 2011;2011:1827-1830. [PMID: 22254684 DOI: 10.1109/IEMBS.2011.6090520]
- Marchina S, Norton A, Schlaug G. Effects of melodic intonation therapy in patients with chronic nonfluent aphasia. Ann N Y Acad Sci 2023;1519:173-185. [PMID: 36349876 DOI: 10.1111/nyas.14927]
- Tabei KI, Satoh M, Nakano C, Ito A, Shimoji Y, et al. Improved neural processing efficiency in a chronic aphasia patient following melodic intonation therapy: a neuropsychological and functional MRI study. Front Neurol 2016;7:148. [PMID: 27698650 DOI: 10.3389/fneur.2016.00148]
- Zhang X, Li J, Du Y. Melodic intonation therapy on non-fluent aphasia after stroke: a systematic review and analysis on clinical trials. Front Neurosci 2022;15:753356. [PMID: 35153655 DOI: 10.3389/fnins.2021.753356]
- Rubi-Fessen I, Hartmann A, Huber W, Fimm B, Rommel T, et al. Add-on effects of repetitive transcranial magnetic stimulation on subacute aphasia therapy: enhanced improvement of functional communication and basic linguistic skills. A randomized controlled study. Arch Phys Med Rehabil 2015;96:1935-1944.e2. [PMID: 26189201 DOI: 10.1016/j.apmr.2015.06.017]
- Kim SJ. Music therapy protocol development to enhance swallowing training for stroke patients with dysphagia. J Music Ther 2010;47:102-119. [PMID: 21141768 DOI: 10.1093/jmt/47.2.102]
- Dong Y, Badrin S, Badrin S, Tang L. Post-stroke fatigue interventions for stroke survivors: a scoping review. Belitung Nurs J 2024;10:601-613. [PMID: 39601026 DOI: 10.33546/bnj.3526]
- Cooper CL, Phillips LH, Johnston M, Whyte M, MacLeod MJ. The role of emotion regulation on social participation following stroke. Br J Clin Psychol 2015;54:181-199. [PMID: 25272054 DOI: 10.1111/bjc.12068]
- Hou X. The application of music therapy in autism spectrum disorder, depression, and anxiety: effects on symptom relief, social skill enhancement, and emotional regulation. Adv Humanit Res 2024;10:23-27. [DOI: 10.54254/2753-7080/2024.18280]
- Yuan B, Xu X, Xie Z, Lin F, Wu Y. Effects of five-element music on post-stroke depression: a systematic review and meta-analysis. 2021 11th International Conference on Information Technology in Medicine and Education (ITME); Wuyishan, Fujian, China: IEEE; 2021:364-373. [DOI: 10.1109/ITME53901.2021.00080]
- Zhang J, Zhao Y, Li H, Yang Y, Tang Q. Effectiveness of acupuncture plus music therapy for post-stroke depression: systematic review and meta-analysis. Medicine 2024;103:e39681. [PMID: 39287303 DOI: 10.1097/MD.0000000000039681]
- Zhang H, Lai H. Five phases music therapy (FPMT) in Chinese medicine: fundamentals and application. Open Access Lib J 2017;4:1-11. [DOI: 10.4236/oalib.1104190]
- Obembe AO, Eng JJ. Rehabilitation interventions for improving social participation after stroke: a systematic review and meta-analysis. Neurorehabil Neural Repair 2016;30:384-392. [PMID: 26223681 DOI: 10.1177/1545968315597072]
- Raukola-Lindblom M, Elina V, Riitta V. Recovering social participation – experience with a relational group intervention for traumatic brain injury patients. NeuroRehabilitation 2020;47:55-64. [PMID: 32675427 DOI: 10.3233/NRE-203083]
- Tamplin J, Loveridge B, Clarke K, Li Y, J Berlowitz D. Development and feasibility testing of an online virtual reality platform for delivering therapeutic group singing interventions for people living with spinal cord injury. J Telemed Telecare 2020;26:365-375. [PMID: 30823854 DOI: 10.1177/1357633X19828463]
- Särkämö T. Singing for rehabilitation. In: Heydon R, Fancourt D, Cohen AJ, editors. The Routledge companion to interdisciplinary studies in singing. Routledge; 2020. pp. 98-108. [DOI: 10.4324/9781315162546-8]
- Good A, Earle E, Vezer E, Gilmore S, Livingstone S, et al. Community choir improves vocal production measures in individuals living with Parkinson’s disease. J Voice 2025;39:848.e7-848.e20. [PMID: 36642592 DOI: 10.1016/j.jvoice.2022.12.001]
- Peretti O, Spyridis Y, Sesis A, Efstathopoulos G. Gamified First Responder Training Solution in Virtual Reality. 2021 17th International Conference on Distributed Computing in Sensor Systems (DCOSS); Pafos, Cyprus: IEEE; 2021:295-301. [DOI: 10.1109/DCOSS52077.2021.00055]
- Bryant L, Brunner M, Hemsley B. A review of virtual reality technologies in the field of communication disability: implications for practice and research. Disabil Rehabil Assist Technol 2020;15:365-372. [PMID: 30638092 DOI: 10.1080/17483107.2018.1549276]
- Devane N, Behn N, Marshall J, Ramachandran A, Wilson S, et al. The use of virtual reality in the rehabilitation of aphasia: a systematic review. Disabil Rehabil 2023;45:3803-3822. [PMID: 36326199 DOI: 10.1080/09638288.2022.2138573]
- Van Der Kooij K, Van Dijsseldonk R, Van Veen M, Steenbrink F, De Weerd C, et al. Gamification as a sustainable source of enjoyment during balance and gait exercises. Front Psychol 2019;10:294. [PMID: 30881322 DOI: 10.3389/fpsyg.2019.00294]
- Colverson A, Barsoum S, Cohen R, Williamson J. Rhythmic musical activities may strengthen connectivity between brain networks associated with aging-related deficits in timing and executive functions. Exp Gerontol 2024;186:112354. [PMID: 38176601 DOI: 10.1016/j.exger.2023.112354]
- Stewart NAJ, Lonsdale AJ. It’s better together: the psychological benefits of singing in a choir. Psychol Music 2016;44:1240-1254. [DOI: 10.1177/0305735615624976]
- Lossing A, Moore M, Zuhl M. Dance as a treatment for neurological disorders. Body Mov Dance Psych 2017;12:170-184. [DOI: 10.1080/17432979.2016.1260055]
- Ou J, Xu C, Fu Y, Chen Q, Han Y, et al. Post-stroke cognitive impairment: a bibliometric and knowledge-map analysis. NeuroRehabilitation 2023;52:175-186. [PMID: 36565073 DOI: 10.3233/NRE-220203]
- Koshimori Y, Thaut MH. New perspectives on music in rehabilitation of executive and attention functions. Front Neurosci 2019;13:1245. [PMID: 31803013 DOI: 10.3389/fnins.2019.01245]
- King JB, Jones KG, Goldberg E, Rollins M, MacNamee K, et al. Increased functional connectivity after listening to favored music in adults with Alzheimer dementia. J Prev Alzheimers Dis 2019;6:56-62. [PMID: 30569087 DOI: 10.14283/jpad.2018.19]
- Chan MMY, Han YMY. The functional brain networks activated by music listening: a neuroimaging meta-analysis and implications for treatment. Neuropsychology 2022;36:4-22. [PMID: 34636582 DOI: 10.1037/neu0000777]
- Vargas A, Díaz P, Zarraonandia T. Using virtual reality and music in cognitive disability therapy. Proceedings of the International Conference on Advanced Visual Interfaces; Salerno Italy: ACM; 2020;35:1-9. [DOI: 10.1145/3399715.3399916]
- Lesiuk T, Bugos JA, Murakami B. A rationale for music training to enhance executive functions in Parkinson’s disease: an overview of the problem. Healthcare 2018;6:35. [PMID: 29690546 DOI: 10.3390/healthcare6020035]
- Wharton W, Goldstein FC, Zhao L, Steenland K, Levey AI, et al. O4-09-02: Certain antihypertensives may slow the conversion from mild cognitive impairment to Alzheimer’s disease. Alzheimers Dement 2015;11:P290. [DOI: 10.1016/j.jalz.2015.07.394]
- Metasari S, Elisa E. Analysis of melodic intonation therapy (MIT) on speech ability in stroke patients with aphasia at Srondol health center. J Health Sci Med Ther 2024;2:181-190. [DOI: 10.59653/jhsmt.v2i03.974]
- Schlaug G, Marchina S, Norton A. From singing to speaking: why singing may lead to recovery of expressive language function in patients with Broca’s aphasia. Music Percept 2008;25:315-323. [PMID: 21197418 DOI: 10.1525/mp.2008.25.4.315]
- Zhang X, Talifu Z, Li J, Li X, Yu F. Melodic intonation therapy for non-fluent aphasia after stroke: a clinical pilot study on behavioral and DTI findings. iScience 2023;26:107453. [PMID: 37744405 DOI: 10.1016/j.isci.2023.107453]
- Li X, Liu J, Wei S, Yu C, Wang D, et al. Cognitive enhancing effect of rTMS combined with tDCS in patients with major depressive disorder: a double-blind, randomized, sham-controlled study. BMC Med 2024;22:253. [PMID: 38902735 DOI: 10.1186/s12916-024-03443-7]
- Sihvonen AJ, Leo V, Ripollés P, Lehtovaara T, Ylönen A, et al. Vocal music enhances memory and language recovery after stroke: pooled results from two RCTs. Ann Clin Transl Neurol 2020;7:2272-2287. [PMID: 33022148 DOI: 10.1002/acn3.51217]
- Raglio A, Oasi O, Gianotti M, Rossi A, Goulene K, et al. Improvement of spontaneous language in stroke patients with chronic aphasia treated with music therapy: a randomized controlled trial. Int J Neurosci 2016;126:235-242. [PMID: 26000622 DOI: 10.3109/00207454.2015.1010647]
- Good DC. Treatment strategies for enhancing motor recovery in stroke rehabilitation. Neurorehabil Neural Repair 1994;8:177-186. [DOI: 10.1177/136140969400800402]
- Arsovski D. The benefits of music therapy in stroke rehabilitation: a systematic literature review. Multidiscip. Pristup Eduk Rehabil 2024;6:113-123. [DOI: 10.59519/mper6112]
- Silkis IG. Possible mechanisms of interdependent roles of the basal ganglia and cerebellum in the functioning of motor and sensory systems. Integr Physiol 2021;2:135-146. [DOI: 10.33910/2687-1270-2021-2-2-135-146]
- Ye X, Li L, He R, Jia Y, Poon W. Rhythmic auditory stimulation promotes gait recovery in Parkinson’s patients: a systematic review and meta-analysis. Front Neurol 2022;13:940419. [PMID: 35968291 DOI: 10.3389/fneur.2022.940419]
- Rosati G, Oscari F, Reinkensmeyer DJ, Secoli R, Avanzini F, et al. Improving robotics for neurorehabilitation: enhancing engagement, performance, and learning with auditory feedback. IEEE Int Conf Rehabil Robot 2011;2011:5975373. [PMID: 22275577 DOI: 10.1109/ICORR.2011.5975373]
- Liu Q, Liu L, Wu H, Liu Y. Effects of reminiscent music therapy with robot-assisted rehabilitation for poststroke recovery older Chinese. Innov Aging 2024;8:109-109. [DOI: 10.1093/geroni/igae098.0350]
- Costa-Giomi E. Does music instruction improve fine motor abilities? Ann N Y Acad Sci 2005;1060:262-264. [PMID: 16597773 DOI: 10.1196/annals.1360.053]
- Seitz RJ, Matyas TA, Carey LM. Neural plasticity as a basis for motor learning and neurorehabilitation. Brain Impair 2008;9:103-113. [DOI: 10.1375/brim.9.2.103]
- Kim SJ, Yeo MS, Kim SY, Kang SY. A scoping review of music-based interventions for swallowing difficulties: implications for treating older adults with presbyphagia. Front Med 2023;10:1285835. [PMID: 38034547 DOI: 10.3389/fmed.2023.1285835]
- Yeo MS, Hwang J, Lee HK, Kim SJ, Cho SR. Therapeutic singing-induced swallowing exercise for dysphagia in advanced-stage Parkinson’s disease. Front Neurol 2024;15:1323703. [PMID: 38628693 DOI: 10.3389/fneur.2024.1323703]
- Aravantinou-fatorou A, Georgakopoulou V, Spandidos D, Papalexis P, Tarantinos K, et al. Effects of music therapy accompanied by transcranial direct current stimulation on the recovery from aphasia following stroke: a single-center retrospective cohort study. World Acad Sci J 2022;4:42. [DOI: 10.3892/wasj.2022.177]
- Yildirim D, Çiriş Yildiz C, Ozdemir FA, Harman Özdoğan M, Can G. Effects of a mindfulness-based stress reduction program on stress, depression, and psychological well-being in patients with cancer: a single-blinded randomized controlled trial. Cancer Nurs 2024;47:E84-E92. [PMID: 36480346 DOI: 10.1097/NCC.0000000000001173]
- Optale G, Capodieci S, Pinelli P, Zara D, Gamberini L, et al. Music-enhanced immersive virtual reality in the rehabilitation of memoryrelated cognitive processes and functional abilities: a case report. Presence Teleop Virt Environ 2001;10:450-462. [DOI: 10.1162/1054746011470217]
- Amirthalingam J, Paidi G, Alshowaikh K, Iroshani Jayarathna A, Salibindla DBAMR, et al. Virtual reality intervention to help improve motor function in patients undergoing rehabilitation for cerebral palsy, Parkinson’s disease, or stroke: a systematic review of randomized controlled trials. Cureus 2021;13:e16763. [PMID: 34367835 DOI: 10.7759/cureus.16763]
- Nemade B, Prajapati S, Thorat Y, Khadke A. AI based music recommendation system using deep learning. Int Res J Mod Eng Technol Sci 2024. [DOI: 10.56726/IRJMETS47832]
- Coulton S, Clift S, Skingley A, Rodriguez J. Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: randomised controlled trial. Br J Psychiatry 2015;207:250-255. [PMID: 26089304 DOI: 10.1192/bjp.bp.113.129908]
- Lam So RW, Wong HS, Ko KM. A Traditional Chinese medicine approach in treating depression by promoting liver Qi circulation: a western medicine perspective. Chinese Med 2015;06:187-195. [DOI: 10.4236/cm.2015.64021]
- van der Meulen I, van de Sandt-Koenderman WM, Heijenbrok-Kal MH, Visch-Brink EG, Ribbers GM. The efficacy and timing of melodic intonation therapy in subacute aphasia. Neurorehabil Neural Repair 2014;28:536-544. [PMID: 24449708 DOI: 10.1177/1545968313517753]
- Hayden R, Clair AA, Johnson G, Otto D. The effect of rhythmic auditory stimulation (RAS) on physical therapy outcomes for patients in gait training following stroke: a feasibility study. Int J Neurosci 2009;119:2183-2195. [PMID: 19916847 DOI: 10.3109/00207450903152609]
- Fotakopoulos G, Kotlia P. The value of exercise rehabilitation program accompanied by experiential music for recovery of cognitive and motor skills in stroke patients. J Stroke Cerebrovasc Dis 2018;27:2932-2939. [PMID: 30072173 DOI: 10.1016/j.jstrokecerebrovasdis.2018.06.025]
- Reagon C, Gale N, Enright S, Mann M, Van Deursen R. A mixed-method systematic review to investigate the effect of group singing on health related quality of life. Complement Ther Med 2016;27:1-11. [PMID: 27515869 DOI: 10.1016/j.ctim.2016.03.017]
- Kostis JB, Dobrzynski JM. Limitations of randomized clinical trials. Am J Cardiol 2020;129:109-115. [PMID: 32560898 DOI: 10.1016/j.amjcard.2020.05.011]
- Hurkmans J, De Bruijn M, Boonstra AM, Jonkers R, Bastiaanse R, et al. Music in the treatment of neurological language and speech disorders: a systematic review. Aphasiology 2012;26:1-19. [DOI: 10.1080/02687038.2011.602514]
- Huang K, Itoh K, Kwee IL, Nakada T. Neural strategies for reading Japanese and Chinese sentences: a cross-linguistic fMRI study of character-decoding and morphosyntax. Neuropsychologia 2012;50:2598-2604. [PMID: 22820634 DOI: 10.1016/j.neuropsychologia.2012.07.011]
- Park MS, Choi JY, Song Y-J, Choi H, Park E-J, et al. Systematic review of behavioral therapy to improve swallowing functions of patients with Parkinson’s disease. Gastroenterol Nurs 2019;42:65-78. [PMID: 30585913 DOI: 10.1097/SGA.0000000000000358]
- Juhos-Kiss E, Vass L, Pusztafalvi H. Zeneterapeuták intézményi jelenléte a magyarországi aphasiaterápiában. Orvosi Hetilap 2023;164:747-752. [DOI: 10.1556/650.2023.32752]
- Murad D, Ye F, Barone M, Wang Y. Motion initiated music ensemble with sensors for motor rehabilitation. 2017 International Conference on Orange Technologies (ICOT); Singapore, Singapore: IEEE; 2017;87-90. [DOI: 10.1109/ICOT.2017.8336095]
- Tuominen PPA, Saarni LA. The use of virtual technologies with music in rehabilitation: a scoping systematic review. Front Virtual Real 2024;5:1290396. [DOI: 10.3389/frvir.2024.1290396]
- Savle V, Sarvade P, Gavli R, Bidkar V, Chitari A, et al. Deep learning based song recommendation system using facial expression and heart rate. IOSR J Comput Eng 2024;26:1-7. [DOI: 10.9790/0661-2606010107]
- Ghozali MT. Predicting patient adherence in healthcare using artificial intelligence and machine learning techniques: a narrative review. 2024 8th International Conference on I-SMAC (IoT in Social, Mobile, Analytics and Cloud) (I-SMAC); Kirtipur, Nepal: IEEE; 2024;1211-1215. [DOI: 10.1109/I-SMAC61858.2024.10714843]
- Li W, Shao C, Zhou H, Du H, Chen H, et al. Multi-omics research strategies in ischemic stroke: a multidimensional perspective. Ageing Res Rev 2022;81:101730. [PMID: 36087702 DOI: 10.1016/j.arr.2022.101730]
- Wang B, Yan T. Multi-modal neuroimaging technique: innovations and applications. Brain Sci Adv 2023;9:53-55. [DOI: 10.26599/BSA.2023.9050017]
- Hirst D. Melody metrics for prosodic typology: comparing English, French and Chinese. Interspeech 2013;14:572-576. [DOI: 10.21437/Interspeech.2013-158]
- Friedman N, Chan V, Zondervan D, Bachman M, Reinkensmeyer DJ. MusicGlove: motivating and quantifying hand movement rehabilitation by using functional grips to play music. 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society; Boston, MA: IEEE; 2011;2359-2363. [DOI: 10.1109/IEMBS.2011.6090659]
- Ee C, Lake J, Firth J, Hargraves F, De Manincor M, et al. An integrative collaborative care model for people with mental illness and physical comorbidities. Int J Ment Health Syst 2020;14:83. [PMID: 33292354 DOI: 10.1186/s13033-020-00410-6]
- Mania I, Kaur J. Music combined with transcranial magnetic stimulation for the treatment of depression. Music Med 2020;12:253. [DOI: 10.47513/mmd.v12i4.750]
- Barwood CHS, Murdoch BE, Whelan B-M, Lloyd D, Riek S, et al. The effects of low frequency Repetitive Transcranial Magnetic Stimulation (rTMS) and sham condition rTMS on behavioural language in chronic non-fluent aphasia: short term outcomes. NeuroRehabilitation 2011;28:113-128. [PMID: 21447912 DOI: 10.3233/NRE-2011-0640]
- Ahluwalia MS, Vogelbaum MA, Chao ST, Mehta MM. Brain metastasis and treatment. F1000Prime Rep 2014;6:114. [PMID: 25580268 DOI: 10.12703/P6-114]
- Rajendran T, Summa-Chadwick M. The scope and potential of music therapy in stroke rehabilitation. J Integr Med 2022;20:284-287. [PMID: 35534380 DOI: 10.1016/j.joim.2022.04.006]
- McIntosh GC, Brown SH, Rice RR, Thaut MH. Rhythmic auditory-motor facilitation of gait patterns in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 1997;62:22-26. [PMID: 9010395 DOI: 10.1136/jnnp.62.1.22]
- Abell RV, Baird AD, Chalmers KA. Group singing and health-related quality of life in Parkinson’s disease. Health Psychol 2017;36:55-64. [PMID: 27584976 DOI: 10.1037/hea0000412]
- Tamplin J, Baker FA, Grocke D, Berlowitz DJ. Thematic analysis of the experience of group music therapy for people with chronic quadriplegia. Top Spinal Cord Inj Rehabil 2014;20:236-247. [DOI: 10.1310/sci2003-236]
- Van Der Meulen I, Van De Sandt-Koenderman ME, Ribbers GM. Melodic intonation therapy: present controversies and future opportunities. Arch Phys Med Rehabil 2012;93:S46-S52. [PMID: 22202191 DOI: 10.1016/j.apmr.2011.05.029]
- Sveistrup H. Motor rehabilitation using virtual reality. J NeuroEngineering Rehabil 2004;1:10. [PMID: 15679945 DOI: 10.1186/1743-0003-1-10]
- Hutchinson K, Sloutsky R, Collimore A, Adams B, Harris B, et al. A music-based digital therapeutic: proof-of-concept automation of a progressive and individualized rhythm-based walking training program after stroke. Neurorehabil Neural Repair 2020;34:986-996. [PMID: 33040685 DOI: 10.1177/1545968320961114]
- Verma P, Mishra N, Srivastava V. Machine learning for personalized medicine: tailoring treatment strategies through data analysis. Pharma Innovation 2019;8:11-14. [DOI: 10.22271/tpi.2019.v8.i3Sa.25249]
- Zhao X, Yang A, Zhang Z-C, Yang YT, Zhao X-M. Deciphering the genetic architecture of human brain structure and function: a brief survey on recent advances of neuroimaging genomics. Brief Bioinform 2023;24:bbad060. [PMID: 36847697 DOI: 10.1093/bib/bbad060]
- Blum K, Simpatico T, Febo M, Rodriquez C, Dushaj K, et al. Hypothesizing music intervention enhances brain functional connectivity involving dopaminergic recruitment: common neuro-correlates to abusable drugs. Mol Neurobiol 2017;54:3753-3758. [PMID: 27246565 DOI: 10.1007/s12035-016-9934-y]
- Matrone C, Brattico E. The power of music on Alzheimer’s disease and the need to understand the underlying molecular mechanisms. J Alzheimers Dis Parkinsonism 2015;5:3. [DOI: 10.4172/2161-0460.1000196]
- Balikuddembe JK, Reinhardt JD. Can digitization of health care help low-resourced countries provide better community-based rehabilitation services? Phys Ther 2020;100:217-224. [PMID: 31680158 DOI: 10.1093/ptj/pzz162]
- Hadidi NN, Huna Wagner RL, Lindquist R. Nonpharmacological treatments for post-stroke depression: an integrative review of the literature. Res Gerontol Nurs 2017;10:182-195. [PMID: 28556875 DOI: 10.3928/19404921-20170524-02]
- Yousufuddin M, Young N. Aging and ischemic stroke. Aging 2019;11:2542-2544. [PMID: 31043575 DOI: 10.18632/aging.101931]
- Kemper KJ, Danhauer SC. Music as therapy. South Med J 2005;98:282-288. [PMID: 15813154 DOI: 10.1097/01.SMJ.0000154773.11986.39]
- Leschallier De Lisle G, Oudin A, Bourla A, Ferreri F, Mouchabac S. Musicotherapy mobile applications: what level of evidence and potential role in psychiatric care? A systematic review. Front Psychiatry 2024;15:1366575. [PMID: 38911704 DOI: 10.3389/fpsyt.2024.1366575]
- Chandan JS, Brown KR, Simms-Williams N, Bashir NZ, Camaradou J, et al. Non-pharmacological therapies for post-viral syndromes, including long COVID: a systematic review. Int J Environ Res Public Health 2023;20:3477. [PMID: 36834176 DOI: 10.3390/ijerph20043477]
- Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain–gut axis in psychiatric and inflammatory disorders. Front Psychiatry 2018;9:44. [PMID: 29593576 DOI: 10.3389/fpsyt.2018.00044]